Differential diagnosis of homer worth’s rossets
Reading File
Finding Sources
Searching the Web
Homer Wright rosettes differential diagnosis pathology tumors
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Now I have comprehensive information. Let me compile the full answer.
Note on terminology: The correct eponym is Homer-Wright rosettes (named after pathologist James Homer Wright, 1869-1928). There is no eponym called "Homer Worth's rosettes." This appears to be a slight misspelling/mispronunciation.
Homer-Wright Rosettes - Overview
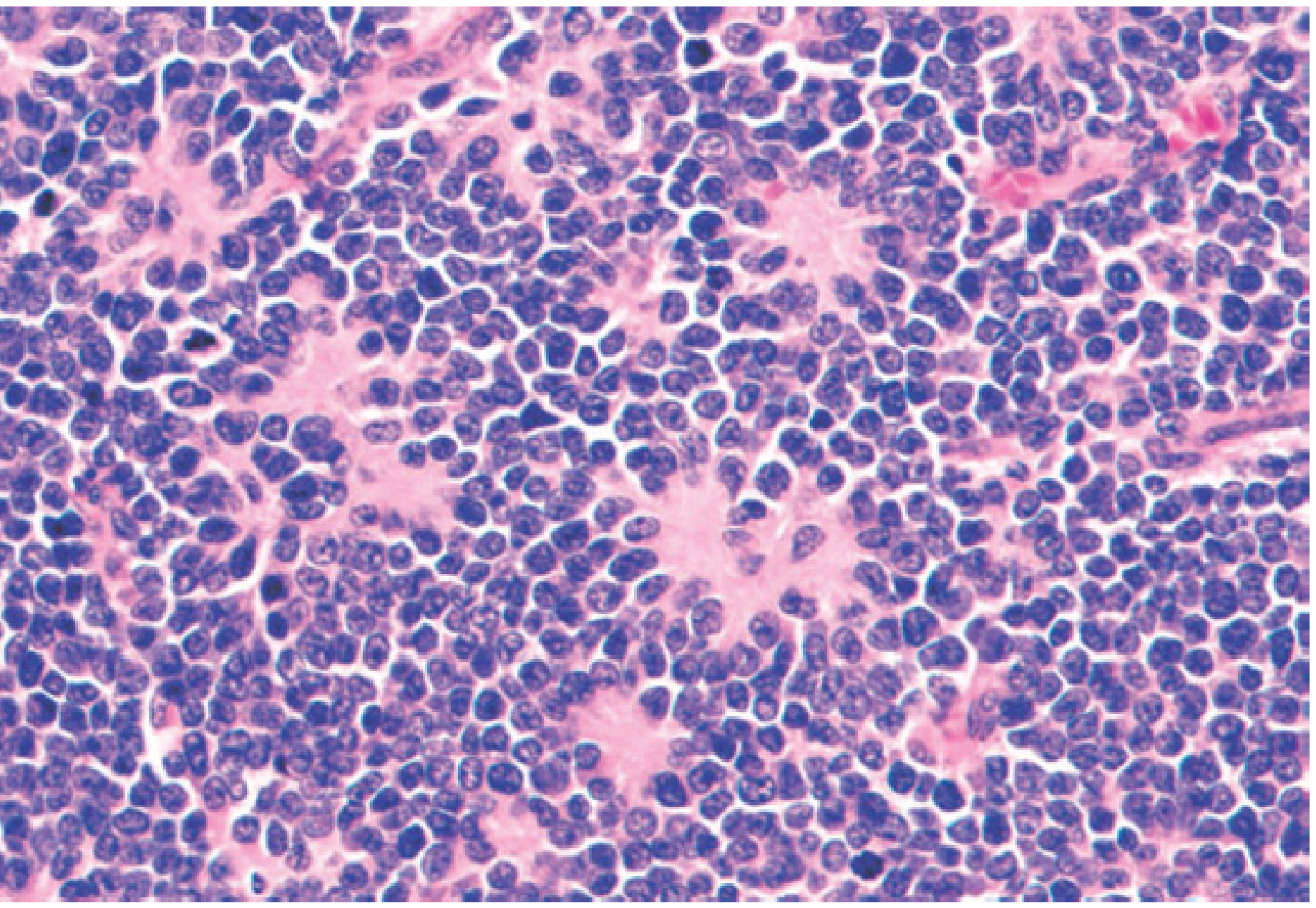
Homer-Wright rosettes (also called Homer-Wright pseudorosettes) are a histological pattern in which small, round blue tumor cells palisade concentrically around a central fibrillary core of neuropil - importantly, there is no central lumen (this distinguishes them from true rosettes such as Flexner-Wintersteiner rosettes).
The central core is composed of eosinophilic, fibrillary neuritic processes, reflecting neuronal differentiation of the tumor cells.
Differential Diagnosis: Tumors Showing Homer-Wright Rosettes
The presence of Homer-Wright rosettes narrows the differential to neuroblastic/neuroectodermal tumors, but several entities can show this pattern:
1. Neuroblastoma (Prototype/Classic)
- Most strongly associated with Homer-Wright pseudorosettes
- Arises from neural crest cells of the sympathetic ganglia and adrenal medulla
- Small, round blue cells with hyperchromatic nuclei and scant cytoplasm
- Cells palisade around central neuritic processes (neuropil)
- IHC: NSE+, synaptophysin+, chromogranin+, NB84+, tyrosine hydroxylase+; MIC-2 (CD99) negative
- Catecholamine metabolites (VMA/HVA) elevated in serum/urine
- Source: Robbins, Cotran & Kumar Pathologic Basis of Disease; Mulholland & Greenfield's Surgery, 7e
2. Medulloblastoma
- Most common malignant brain tumor of childhood (~20% of pediatric CNS tumors)
- Arises in the posterior fossa (cerebellar vermis)
- Highly cellular tumor with dark-staining, round, hyperchromatic nuclei; scant cytoplasm
- Forms Homer-Wright rosettes + expresses neuronal markers (synaptophysin+); GFAP less common
- Four WHO molecular subgroups: WNT-activated, SHH-activated, Group 3, Group 4
- Source: Harrison's Principles of Internal Medicine 22E; Robbins, Cotran & Kumar
3. Esthesioneuroblastoma (Olfactory Neuroblastoma)
- Accounts for 5% of sinonasal malignancies; arises in the olfactory groove
- Characterized by both Homer-Wright pseudorosettes (no lumen) and Flexner-Wintersteiner rosettes (true, with lumen)
- Small blue cells with lobular architecture and prominent microvascularity
- IHC: S-100 protein+, NSE+; cytokeratin negative
- Source: KJ Lee's Essential Otolaryngology; Scott-Brown's Otorhinolaryngology
4. Primitive Neuroectodermal Tumor (PNET) / Peripheral PNET
- Shares major histopathologic features with neuroblastoma
- Sheets of small round cells that may form Homer-Wright rosettes
- Key differentiator from neuroblastoma: MIC-2 (CD99) positive in PNET, negative in neuroblastoma
- t(12;22)(q24;q12) translocation highly specific for PNET (helps distinguish from neuroblastoma)
- Source: Dermatology 2-Volume Set 5e; Henry's Clinical Diagnosis; Campbell-Walsh Urology
5. Pineoblastoma
- Highly malignant pineal region tumor; primitive embryonal appearance
- Can show Homer-Wright rosettes (and also Flexner-Wintersteiner rosettes in some cases)
- WHO Grade 4; associated with bilateral retinoblastoma ("trilateral retinoblastoma")
6. Merkel Cell Carcinoma (MCC)
- Primary cutaneous neuroendocrine carcinoma
- May show rosette-like structures resembling Homer-Wright rosettes of neuroblastoma
- IHC: CK20+, synaptophysin+, chromogranin+ (key marker - paranuclear dot pattern of CK20)
- Source: Dermatology 2-Volume Set 5e
7. Ewing Sarcoma / Ewing Sarcoma Family Tumors (ESFTs)
- Histologically: sheets of small round cells that may form Homer-Wright rosettes
- ESFT subclassified into Ewing sarcoma or peripheral primitive neuroectodermal tumor
- Key genetic marker: t(11;22)(q24;q12) - EWSR1::FLI1 fusion (most common); CD99 strongly positive
- Source: Henry's Clinical Diagnosis; Robbins, Cotran & Kumar
8. Cutaneous Metastatic Neuroblastoma
- In children: blue-purple dermal papules ("blueberry muffin" pattern)
- Ill-defined infiltrative mass in dermis/subcutis with Homer Wright-type rosette formation
- Fibrillary center is the histologic hallmark
- Source: Dermatology 2-Volume Set 5e
9. Metastatic Malignant Melanoma (rare mimicker)
- Rare but documented - metastatic melanoma can occasionally form Homer-Wright rosettes, mimicking a neuroblastic tumor
- IHC differentiates: S-100+, HMB-45+, Melan-A+ in melanoma; neuronal markers absent
- Source: PubMed PMID 12783323
Key Distinguishing Features at a Glance
| Tumor | Location | Key IHC/Genetics | Other Rosettes |
|---|---|---|---|
| Neuroblastoma | Adrenal/sympathetic ganglia | NSE+, NB84+, VMA/HVA↑, MIC-2- | None |
| Medulloblastoma | Posterior fossa (cerebellum) | Synaptophysin+, GFAP±, WNT/SHH subtypes | None typical |
| Esthesioneuroblastoma | Olfactory groove | S-100+, NSE+, CK- | Flexner-Wintersteiner also present |
| PNET | Peripheral/CNS | MIC-2 (CD99)+, t(12;22) | None |
| Pineoblastoma | Pineal gland | Synaptophysin+, GFAP- | Flexner-Wintersteiner possible |
| Merkel Cell Carcinoma | Skin | CK20+ (paranuclear dot), CD56+ | Rosette-like only |
| Ewing Sarcoma | Bone/soft tissue | CD99 strong+, t(11;22) EWSR1::FLI1 | None |
Important Distinction: Homer-Wright vs. Flexner-Wintersteiner Rosettes
| Feature | Homer-Wright | Flexner-Wintersteiner |
|---|---|---|
| Central lumen | Absent (pseudorosette) | Present (true rosette) |
| Center content | Fibrillary neuropil | Empty lumen |
| Classic tumor | Neuroblastoma, medulloblastoma | Retinoblastoma |
| Differentiation implies | Neuronal (neuropil) | Photoreceptor (retinal) |
The bottom line: Homer-Wright rosettes are a marker of neuroblastic/neuronal differentiation and their presence should prompt consideration of neuroblastic tumors first, then broader small round blue cell tumors with neural features. IHC (NSE, synaptophysin, NB84, CD99, S-100, CK20) and molecular studies (MYCN amplification, characteristic translocations) are essential to narrow the differential.
This is a shared conversation. Sign in to Orris to start your own chat.