CVS
Asking for Preferences
"CVS" is ambiguous without more context. Here are the most common interpretations:
-
Chorionic Villus Sampling - A prenatal diagnostic procedure done around 10-13 weeks of pregnancy to test for chromosomal/genetic conditions (e.g., Down syndrome). Involves taking a small sample of placental tissue.
-
Cardiovascular System - The heart and blood vessel system; a common topic in anatomy, physiology, and medicine.
-
CVS Pharmacy - A major US retail pharmacy chain (formerly Consumer Value Stores).
-
CSV (Comma-Separated Values) - A file format used for tabular data in spreadsheets and databases.
-
Concurrent Versions System - A legacy source code version control system in software development.
Could you clarify what you're asking about? For example:
- "CVS procedure risks" - I'd cover the prenatal test
- "CVS anatomy" - I'd cover the cardiovascular system
- "CVS stock price" - I'd look up the pharmacy company
- "CVS file format" - I'd explain the data format
CVA
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Here is a thorough overview of CVA (Cerebrovascular Accident / Stroke):
CVA - Cerebrovascular Accident (Stroke)
Definition
A stroke (CVA) is the interruption of blood flow to the brain or brainstem resulting in impaired neurological function lasting more than 24 hours. Neurological impairment that resolves within 24 hours is called a transient ischemic attack (TIA) or "mini-stroke." - Gray's Anatomy for Students
Epidemiology
- Over 795,000 strokes per year in the United States; 15 million worldwide annually
- Prevalence in persons >65 years: ~60 per 1,000; in >75 years: ~95 per 1,000
- Fifth leading cause of death in the US, but ~75% of stroke victims survive
- Estimated 1 in 200 individuals will sustain a CVA in their lifetime
- Campbell-Walsh-Wein Urology
Classification
Strokes are broadly divided into two types:
1. Ischemic Stroke (~85% of cases)
Caused by blockage of cerebral blood supply. Further subdivided into:
- Thrombotic - clot forms locally in a cerebral vessel (often on atherosclerotic plaque)
- Embolic - the most common type; emboli (often from carotid artery atherosclerotic plaques) migrate and block smaller intracranial vessels
2. Hemorrhagic Stroke (~15%)
Caused by rupture of a blood vessel, leading to bleeding into or around the brain.
Risk Factors
- Hypertension (most significant modifiable risk factor)
- Diabetes mellitus
- Smoking
- Atrial fibrillation
- Atherosclerosis / hyperlipidemia
- In younger patients: clotting disorders, oral contraceptive use, illicit substances (e.g., cocaine)
Clinical Presentation
Symptoms depend on the location and distribution of impaired brain perfusion. Common features include:
| Symptom | Notes |
|---|---|
| Hemiparesis / hemiplegia | Contralateral to the lesion |
| Hemisensory loss | Contralateral |
| Visual field deficits | Homonymous hemianopia |
| Dysarthria / aphasia | Dominant hemisphere lesions |
| Ataxia | Cerebellar or posterior circulation |
| Decreased level of consciousness | Large territory infarcts |
| Urinary incontinence | 32-79% on admission; a poor prognostic sign |
Urinary incontinence within 7 days of stroke is a powerful prognostic indicator for poor survival and functional dependence - more so than depressed consciousness. - Campbell-Walsh-Wein Urology
Imaging
Stroke is a neurological emergency - urgent imaging is required to distinguish ischemic from hemorrhagic stroke before treatment.
CT Scan (first-line, urgent)
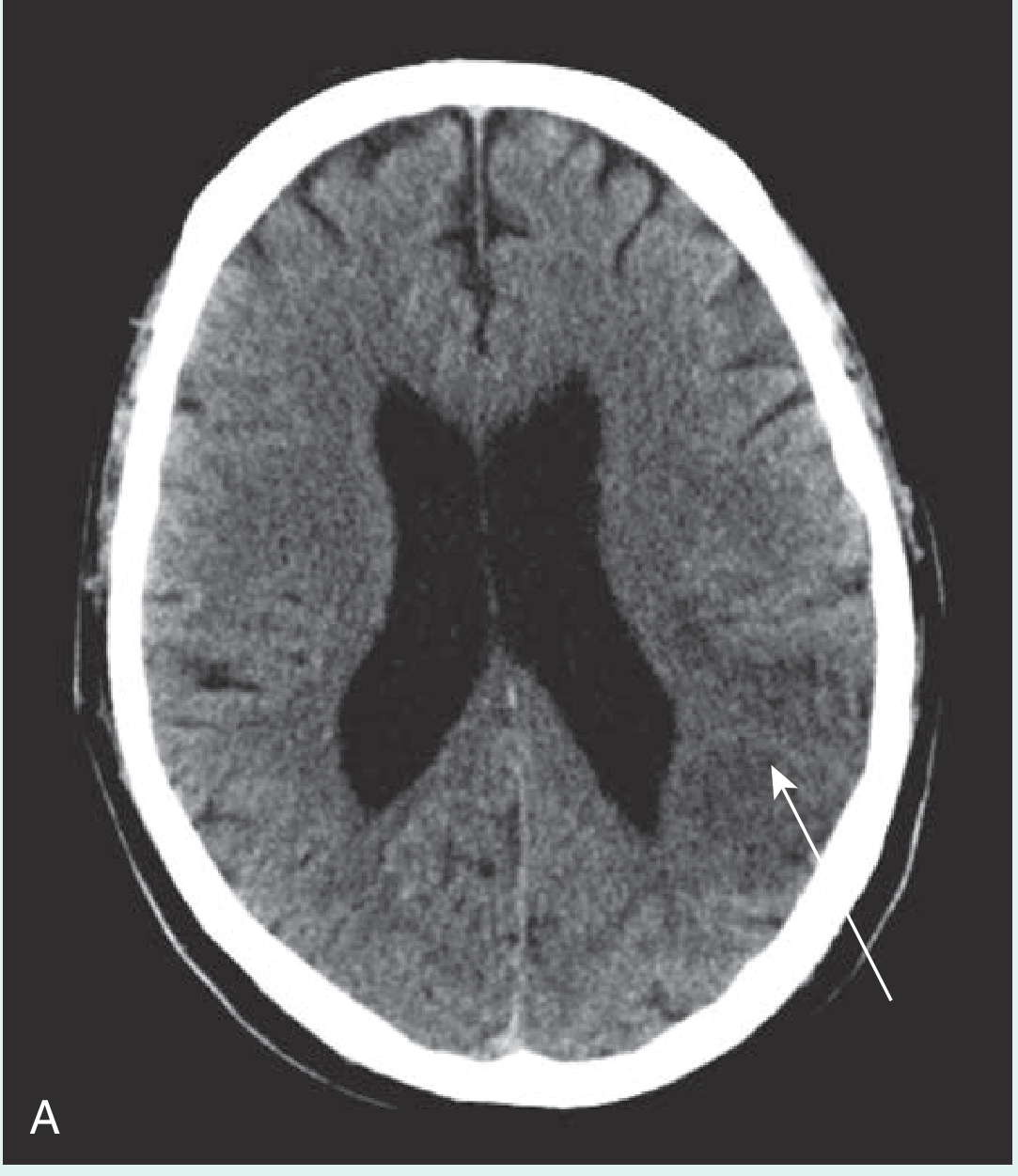
- Early CT may be normal or show a darker low-density area in ischemic stroke
- Identifies hemorrhagic strokes (for which thrombolysis is contraindicated)
- Excludes alternative diagnoses (e.g., tumor)
MRI (better soft tissue resolution, follow-up)
- Acute stroke: bright on DWI + dark on ADC map = restricted diffusion (changes persist ~1 week)
- T2-weighted: bright area representing infarcted tissue
- Better for small strokes missed on CT
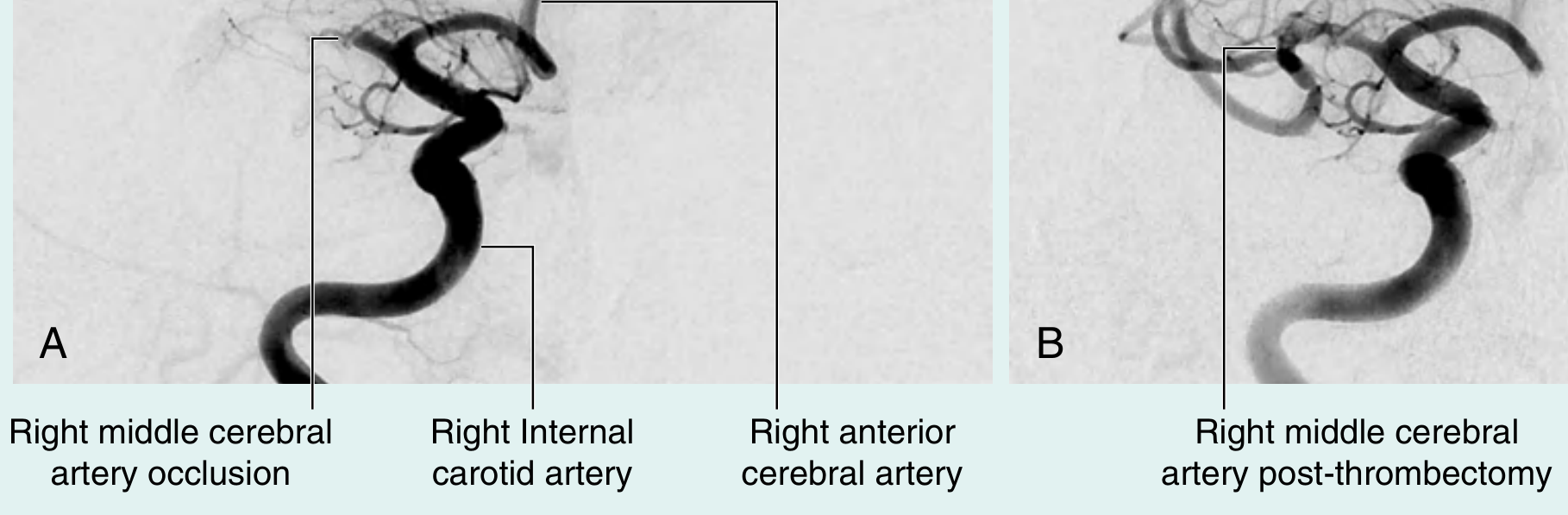
Cerebral Angiography
Treatment
Acute Management
- IV tPA (tissue plasminogen activator) - thrombolytic therapy for ischemic stroke; effective if given within 3-4.5 hours of symptom onset; contraindicated in hemorrhagic stroke
- Mechanical thrombectomy - catheter-based clot removal; can be performed up to 24 hours in selected patients
- Supportive care: airway, blood pressure management, glucose control
Post-Acute / Rehabilitation
- Multidisciplinary team: neurologist, physiotherapist, speech & language therapist, occupational therapist
- Antiplatelet therapy (e.g., aspirin) for secondary prevention in ischemic stroke
- Cardiovascular risk factor modification: blood pressure control, statins, smoking cessation, diabetes management
Carotid Endarterectomy
- For significant carotid artery stenosis contributing to embolic stroke risk
Key Complications / Sequelae
- Impaired mobility / paralysis
- Cognitive impairment
- Dysphasia
- Urinary and fecal incontinence
- Depression
- Dysphagia (aspiration risk)
- Death (especially when urinary incontinence present at admission - hazard ratio 2.8 at 3 months)
Sources: Gray's Anatomy for Students, Campbell-Walsh-Wein Urology, Fischer's Mastery of Surgery, Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.