hospital acquired infections with recent guidelines
Reading File
Searching PubMed
"healthcare associated infections" AND "guidelines"
Searching the Web
hospital acquired infections guidelines 2024 2025 CDC IDSA recommendations
Finding Sources
Searching PubMed
"healthcare associated infection" AND prevention AND "bundle"
Searching PubMed
"CLABSI" OR "CAUTI" OR "VAP" AND prevention guidelines
Reading File
Reading Article
Reading Article
Reading File
Searching PubMed
"Clostridioides difficile" OR "MRSA" AND hospital infection prevention
Reading File
Reading Web Page
hospital acquired infection types prevention guidelines 2024 2025
Loading Image
I now have everything needed for a thorough, well-sourced response. Here it is:
Hospital-Acquired Infections (HAIs) - Nosocomial Infections
Definition
A hospital-acquired infection (HAI), also called a nosocomial infection, is an infection acquired during hospital care that was not present or incubating at admission. Infections occurring more than 48 hours after admission are classified as nosocomial. They may be endemic (constant background rate) or epidemic (outbreak above baseline).
The WHO and CDC extend this definition to infections acquired in any healthcare setting, including long-term care facilities and outpatient settings.
- Park's Textbook of Preventive and Social Medicine, p. 409
Epidemiology (CDC 2024 Data)
The CDC 2024 HAI Progress Report - the most current national data - shows:
- Approximately 1 in 31 US hospital patients acquires at least one HAI every day
- 2024 marked the third consecutive year of declining HAI rates following pandemic-era surges
- Data collected from >38,000 US healthcare facilities via NHSN (National Healthcare Safety Network)
- Long-term acute care hospitals showed a 23% decrease in VAEs and 15% drop in C. difficile infections in 2024
- Inpatient rehabilitation facilities saw an 18% drop in C. difficile and 8% decline in CAUTIs
- 17 states performed better on at least 2 infection types in 2024 compared to 2023
Sites of Nosocomial Infection
The most common sites (French National Prevalence Survey):
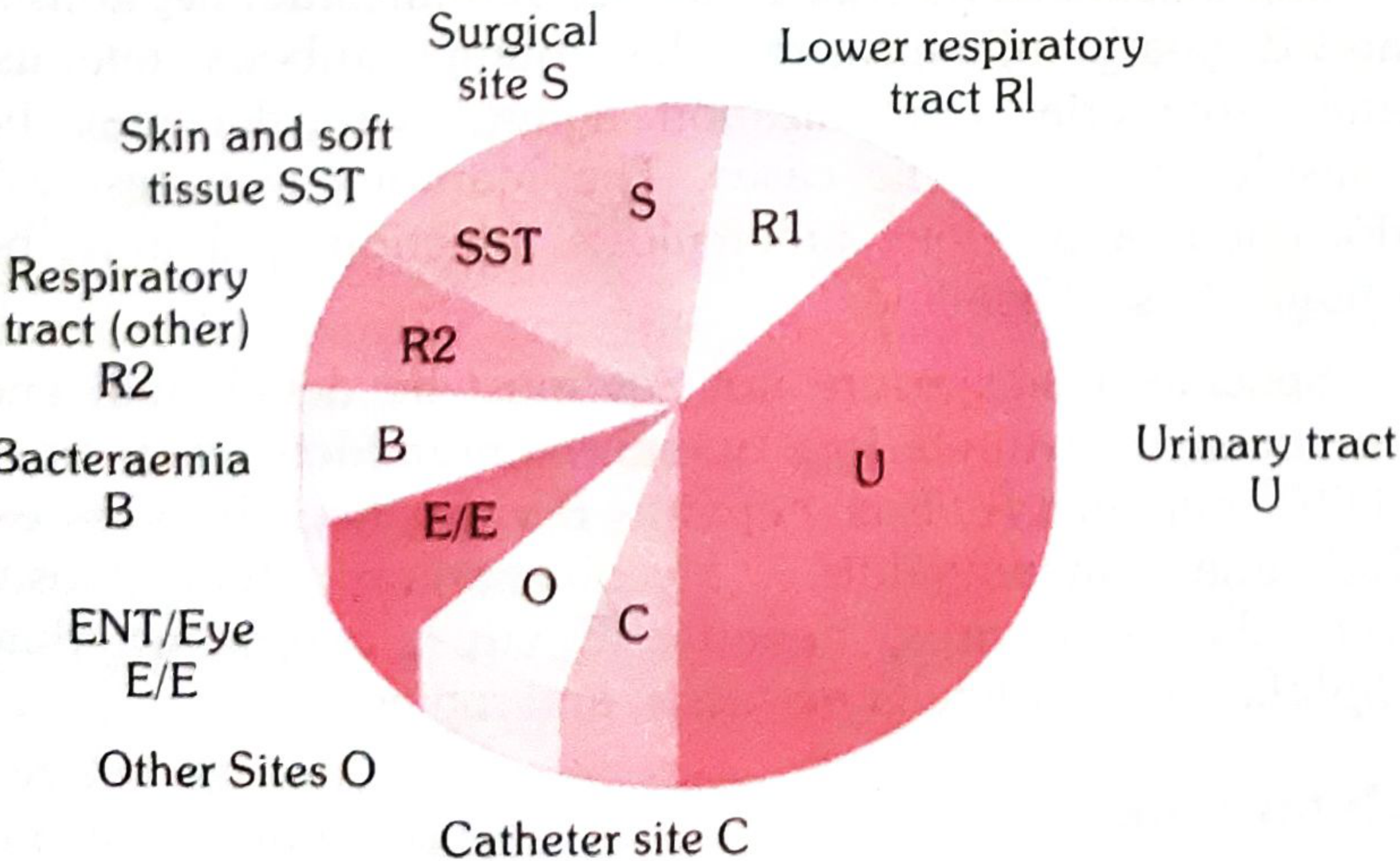
| Site | Common Pathogens |
|---|---|
| Urinary tract (most common) | E. coli, Enterococcus, Candida |
| Lower respiratory tract | Pseudomonas, Klebsiella, S. aureus |
| Surgical site | S. aureus, MRSA, coagulase-negative Staph |
| Skin and soft tissue | S. aureus, Streptococcus |
| Bloodstream / Bacteremia | CoNS, S. aureus, Gram-negatives |
| Catheter site | CoNS, S. aureus |
| ENT / Eye | Various |
The "Big 5" HAI Categories Tracked by CDC/NHSN
1. CAUTI - Catheter-Associated Urinary Tract Infection
- Most common nosocomial infection globally
- Simplified diagnostic criterion: Positive urine culture (≥10⁵ bacteria/mL, 1-2 species), with or without symptoms
- 2025 ISID-endorsed interventions (PMID 41059852): avoid unnecessary catheterization, use smallest effective catheter, maintain closed drainage system, remove catheter at earliest opportunity, maintain unobstructed urine flow, consider antimicrobial-impregnated catheters in high-risk patients
- 2025 IDSA guideline on complicated UTI recommends tailoring empiric antibiotics using local antibiograms for septic presentations
2. CLABSI - Central Line-Associated Bloodstream Infection
- ISID 2024 Position Paper (PMID 39505252): evidence-based prevention bundle includes:
- Maximal sterile barrier precautions during insertion
- Chlorhexidine gluconate (CHG) skin antisepsis
- Subclavian vein as preferred insertion site (over femoral/jugular)
- Daily review of catheter necessity and prompt removal
- CHG-impregnated dressings and catheter-locking solutions
- Antimicrobial-coated catheters when institutional rates remain high
3. VAP - Ventilator-Associated Pneumonia
- ISID 2024 Position Paper (PMID 39551087): key VAP prevention bundle:
- Head-of-bed elevation 30-45° - a 2024 meta-analysis (PMID 39300424) confirmed this reduces VAP (though very high elevation increases pressure ulcer risk - optimal ~30-35°)
- Oral decontamination with CHG
- Subglottic secretion drainage
- Daily sedation interruption and weaning assessment
- Avoid unnecessary endotracheal tube changes
- Early mobilization where feasible
4. SSI - Surgical Site Infection
- Simplified surveillance criterion: Any purulent discharge, abscess, or spreading cellulitis at surgical site within 1 month of operation
- Prevention: pre-op antibiotic prophylaxis (within 60 min of incision), hair removal only with clippers (not razors), normothermia maintenance, glycemic control, CHG bathing
5. C. difficile (CDI) - Hospital-onset
- ESCMID 2024 guidelines (PMID 39154859): pre-operative decolonization in MDR-colonized patients
- A 2025 Cochrane review (PMID 40931979) supports probiotics for primary CDI prevention in adults and children in antibiotic-exposed settings
- Contact precautions, sporicidal disinfectants (bleach-based), and antimicrobial stewardship remain cornerstones
Also tracked: MRSA bloodstream events
Sources of HAIs
The textbook framework identifies three sources (Park's Textbook, p. 409):
- Patients - Active infections (TB, influenza, wound infections, UTIs, viral infections)
- Staff - Carriers of S. aureus (nasal/skin), Haemolytic streptococci (throat), Salmonella (gut)
- Environment - Hospital dust, linen, bedclothes, sinks, door handles, air
Routes of Transmission
- Direct contact (hands of healthcare workers - the most common route)
- Droplet infection
- Airborne particles
- Hospital dust
- Invasive procedures: catheterization, IV lines, dressings, endoscopy
Risk Factors for High Susceptibility
- Immunocompromised states (malignancy, chemotherapy, organ transplant, HIV)
- Extremes of age (neonates, elderly)
- Severe critical illness (ICU patients)
- Corticosteroid therapy
- Prolonged hospitalization
- Invasive devices in situ
- Urological, geriatric, and neonatal wards are highest-risk settings
Prevention - Core Strategies
Standard Precautions (ALL patients)
| Measure | Detail |
|---|---|
| Hand hygiene | Most important single intervention - WHO 5 Moments (before patient contact, before aseptic procedure, after body fluid exposure, after patient contact, after contact with patient surroundings) |
| PPE | Gloves for blood/body fluid contact; mask/gown/eye protection for splash risk |
| No-touch technique | Where possible for procedures |
| Sharps safety | Proper handling and disposal |
| Environmental decontamination | Prompt spill management, terminal cleaning |
| Linen management | Machine wash or boiling for contaminated linen |
Isolation Precautions
- Contact precautions: MRSA, VRE, C. difficile, MDR organisms
- Droplet precautions: Influenza, Meningococcal disease
- Airborne precautions: TB, Measles, Varicella (negative pressure rooms)
Antimicrobial Stewardship
The ESCMID 2024 stewardship guidelines for emergency departments emphasize:
- Shortest effective antibiotic duration
- De-escalation based on culture results
- Antibiogram-guided empiric therapy
- IV-to-oral switching at earliest opportunity
Staff Health Programme (Prevention in Healthcare Workers)
Park's Textbook, p. 411
- Pre-employment health review including immunization history and tuberculin (Mantoux) testing
- Vaccinations recommended for HCWs: Hepatitis A and B, annual influenza, MMR, Td, Varicella (if seronegative)
- Staff with active infections (skin disease, sore throat, diarrhea) should be excluded from patient contact until recovered
- Post-exposure protocols for: HIV, HBV, HCV, TB, Meningococcus, VZV, Pertussis, Rabies
Surveillance and Governance
- NHSN definitions are the global standard for HAI surveillance
- Hospitals must report CLABSIs, CAUTIs, VAEs, SSIs, MRSA bacteremia, and CDI to NHSN (mandatory in the US)
- CMS financial penalty programs (since 2015) incentivize HAI prevention
- Infection Control Committee should review rates, conduct root cause analyses of outbreaks, and audit compliance with bundles
Summary Table: Diagnostic Criteria & Prevention Bundles
| HAI Type | Key Diagnostic Criterion | Core Prevention Bundle |
|---|---|---|
| CAUTI | ≥10⁵ CFU/mL urine + catheter in situ | Avoid/remove catheter early, closed drainage |
| CLABSI | Bacteremia with no other source, CVC in situ | Sterile insertion, CHG antisepsis, daily necessity review |
| VAP | New infiltrate + ≥2 clinical signs after 48h MV | HOB 30-45°, oral CHG, subglottic drainage |
| SSI | Purulent discharge/abscess within 30 days | Prophylactic antibiotics, glycemic control, normothermia |
| CDI | Positive C. diff toxin + ≥3 loose stools/day | Contact precautions, sporicidal cleaning, stewardship |
| MRSA BSI | MRSA in blood culture | Decolonization, CHG bathing, barrier precautions |
Key Recent Guidelines (2023-2025):
- ISID 2024: VAP Prevention (PMID 39551087) and CLABSI Prevention (PMID 39505252) - updated position papers
- ESCMID 2024: Decolonization before surgery in MDR carriers (PMID 39154859)
- ESCMID 2024: Antimicrobial stewardship in emergency departments (PMID 39029872)
- Cochrane 2025: Probiotics for CDI prevention (PMID 40931979)
- CDC 2024 HAI Progress Report: third straight year of declines, data from >38,000 facilities
Prepare ppt , flash cards
Reading File
Reading File
Running Command
Writing File
Running Command
Writing File
Running Command
Running Command
Both files are ready. Here's a summary of what was created:
Downloads
| File | Download |
|---|---|
| PowerPoint Presentation (10 slides) | HAI Hospital Acquired Infections Presentation · PPTX |
| Flashcards PDF (16 cards) | HAI Flashcards PDF Document · PDF |
What's Inside
PowerPoint (10 Slides) - Navy/Teal medical theme
| Slide | Topic |
|---|---|
| 1 | Title slide |
| 2 | Definition & Epidemiology (CDC 2024 stats) |
| 3 | Common Sites of Infection (with pathogen distribution) |
| 4 | Sources & Routes of Transmission |
| 5 | The "Big 5" HAIs - criteria & prevention at a glance |
| 6 | Prevention Bundles (CLABSI, VAP, CAUTI, SSI) |
| 7 | Standard Precautions & Isolation Types |
| 8 | Antimicrobial Stewardship + Staff Health Programme |
| 9 | Recent Guidelines 2023-2025 (ISID, ESCMID, Cochrane, CDC) |
| 10 | Key Takeaways (dark closing slide) |
Flashcards (16 Cards, 2 per A4 page)
- Definition & Criteria
- 3 Sources of HAI
- 5 Routes of transmission
- Big 5 diagnostic criteria
- CLABSI, VAP, CAUTI, SSI prevention bundles
- WHO 5 Moments for Hand Hygiene
- Isolation precaution types
- Risk factors for HAI
- HCW vaccination schedule
- Antimicrobial stewardship principles
- CDC 2024 data highlights
- CDI prevention strategy
- Simplified surveillance criteria
This is a shared conversation. Sign in to Orris to start your own chat.