Uterus mbbs nots 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
I have all the content I need for a thorough 10-mark MBBS answer. Let me now compile the complete notes.
Uterus - MBBS Notes (10 Marks)
1. Introduction
The uterus is a thick-walled, hollow, pear-shaped muscular organ situated in the midline of the female pelvis, between the urinary bladder anteriorly and the rectum posteriorly.
Size (non-pregnant adult): ~7.5 cm long, 5 cm wide, 2.5 cm thick
Weight: ~60-80 g
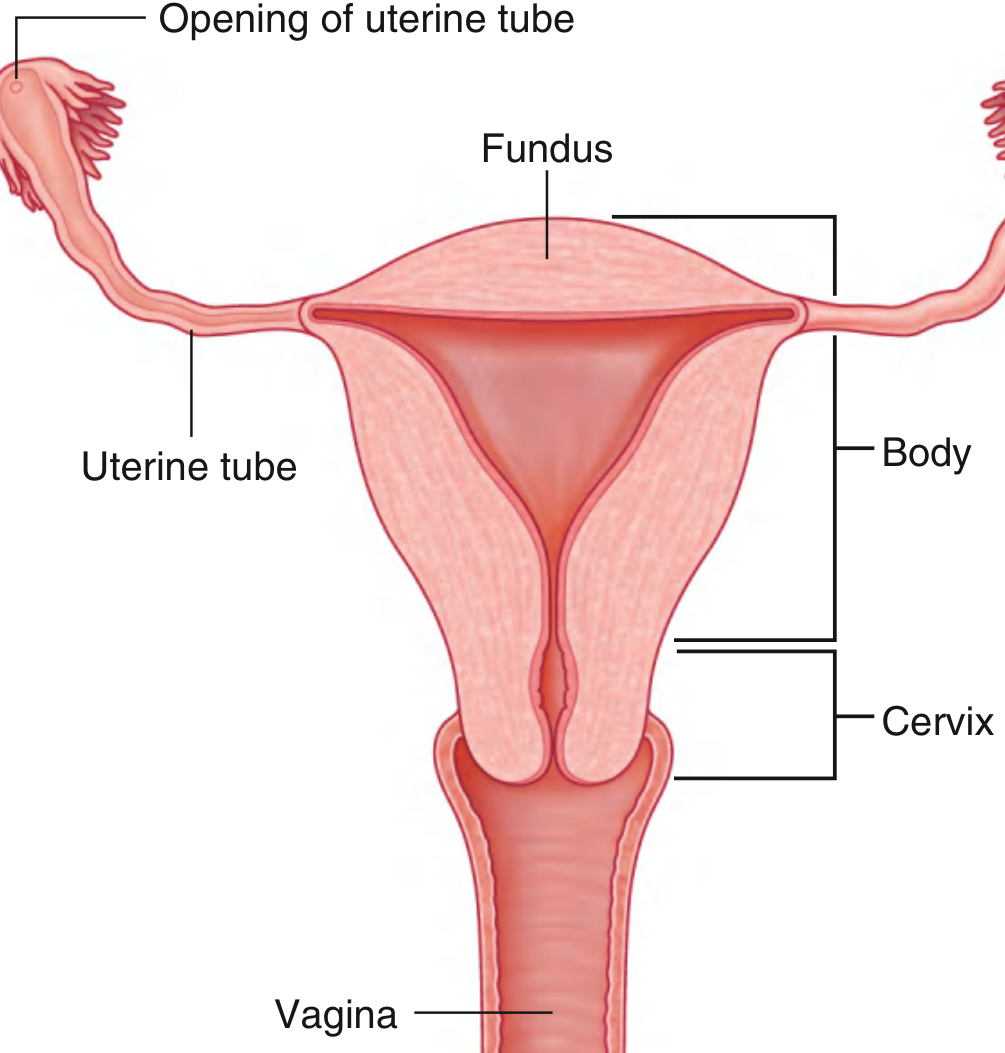
2. Parts of the Uterus
| Part | Description |
|---|---|
| Fundus | Rounded, dome-shaped superior part; above the level of uterine tube openings |
| Body (Corpus) | Main bulk; flattened anteroposteriorly; cavity is triangular when viewed from front |
| Isthmus | Constricted junction between body and cervix (~1 cm); becomes the lower uterine segment in pregnancy |
| Cervix | Cylindrical lower portion, 2.5 cm long; projects into vagina as the portio |
The cervical canal has two openings:
- Internal os - opens into isthmus
- External os - opens into vagina (round in nulliparous, transverse slit after vaginal delivery)
3. Position
- Normally in anteversion + anteflexion
- Anteversion: the uterus as a whole is tilted forward relative to the vagina
- Anteflexion: the body is bent forward on the cervix (angle ~125°)
- Position changes with bladder and rectal fullness
4. Relations
| Surface/Direction | Relation |
|---|---|
| Anterior | Vesicouterine pouch and urinary bladder |
| Posterior | Rectouterine pouch (Pouch of Douglas) and rectum |
| Lateral (broad ligament) | Ureter, uterine artery, ovary |
| Inferior | Vagina |
Important clinical point: During hysterectomy or ligation of uterine artery, the ureter passes close beneath the uterine artery at the base of the broad ligament ("water under the bridge") - risk of ureteric injury.
5. Supports (Ligaments)
The uterus is supported by pelvic floor muscles + ligaments:
Primary/Main Supports:
| Ligament | Origin → Insertion | Key Feature |
|---|---|---|
| Transverse cervical (Mackenrodt's/Cardinal) ligament | Cervix & vaginal vault → lateral pelvic wall | Most important; prevents uterine prolapse |
| Uterosacral ligament | Posterior cervix → sacrum (S2-S4) | Keeps cervix backward and upward; contains autonomic nerves |
| Pubocervical ligament | Cervix → pubis | Prevents forward displacement |
Secondary/Peritoneal Ligaments:
| Ligament | Description |
|---|---|
| Broad ligament | Double peritoneal fold from lateral uterus to lateral pelvic wall; contains mesometrium, mesosalpinx, mesovarium; NOT a true ligament |
| Round ligament | From uterine horn → inguinal canal → labium majus; maintains anteversion; has smooth muscle |
| Infundibulopelvic (suspensory) ligament of ovary | Ovary to pelvic wall; transmits ovarian vessels |
6. Walls (Microscopic Structure)
The uterine wall has 3 layers:
A. Perimetrium (Serosa)
- Outermost layer; peritoneal covering
- Adventitial (no serosa) on anterior and lateral aspects of lower uterus
- Continuous with broad ligament laterally
B. Myometrium
- Thickest layer; composed of interlacing bundles of smooth muscle
- Three indistinct layers (outer longitudinal, middle circular, inner longitudinal)
- Middle circular layer contains large blood vessels
- During pregnancy: undergoes hyperplasia + hypertrophy; contracts forcefully during parturition
- After pregnancy: cells shrink, many undergo apoptosis
C. Endometrium (Mucosa)
- Simple columnar epithelium (ciliated + secretory cells)
- Contains tubular uterine glands penetrating full thickness
- Two zones:
- Basal layer (stratum basalis): Adjacent to myometrium; NOT shed during menstruation; regenerates the functional layer; supplied by straight arteries
- Functional layer (stratum functionalis): Superficial; undergoes cyclic changes; shed during menstruation; supplied by spiral (coiled) arteries
7. Menstrual Cycle - Endometrial Changes
| Phase | Days | Hormone | Endometrial Change |
|---|---|---|---|
| Proliferative (follicular) | 5-14 | Estrogen (from developing follicle) | Glands enlarge & lengthen; stroma proliferates; spiral arteries grow |
| Secretory (luteal) | 15-28 | Progesterone + estrogen (corpus luteum) | Glands become coiled, tortuous, sacculated; stroma becomes edematous; spiral arteries become tortuous |
| Menstrual | 1-4 | Progesterone withdrawal | Vasoconstriction of spiral arteries → ischemia → necrosis → shedding of functional layer |
The basal layer is supplied by straight arteries (not affected by progesterone withdrawal) and is always retained.
8. Blood Supply
| Vessel | Source | Course |
|---|---|---|
| Uterine artery (main) | Internal iliac artery | Runs in broad ligament; crosses over the ureter at the level of the internal os; ascends along lateral uterine wall in a tortuous course; at fundus anastomoses with ovarian artery |
| Ovarian artery | Abdominal aorta (L2) | Supplies fundus via anastomosis with uterine artery |
Venous drainage: Uterine venous plexus (valveless) → uterine veins → internal iliac veins
9. Lymphatic Drainage
| Region | Drains To |
|---|---|
| Fundus & body | Para-aortic nodes (along aorta, via infundibulopelvic ligament) |
| Body | Superficial inguinal nodes (via round ligament) |
| Body (also) | External/internal iliac nodes (via broad ligament) |
| Cervix | Internal iliac + obturator nodes; also sacral nodes |
10. Nerve Supply
- Sympathetic: T12-L1 via hypogastric plexus (→ vasoconstriction, uterine contraction)
- Parasympathetic: S2-S4 via pelvic splanchnic nerves
- Both form the uterovaginal plexus (Frankenhäuser ganglion) lateral to the cervix
- Pain from body/fundus: T11-T12 (referred to lower abdomen)
- Pain from cervix: S2-S4 (referred to back/thighs)
11. Clinical Notes
- Hysterectomy: Removal of uterus; care must be taken to ligate uterine arteries without injuring the ureter beneath them
- Lower uterine segment: Formed from the isthmus during pregnancy; site of lower segment caesarean section (LSCS) - less vascular, heals better
- Implantation: Blastocyst normally implants in the body of the uterus
- Uterine prolapse: Weakening of cardinal and uterosacral ligaments + levator ani; uterus descends into vagina
- Endometriosis: Ectopic endometrial tissue; most common in pouch of Douglas
- Retroversion: ~20% of women; uterus tilted backward; can cause dysmenorrhoea and dyspareunia
Quick Summary Box
UTERUS
├── Parts: Fundus → Body → Isthmus → Cervix
├── Position: Anteverted + Anteflexed (normal)
├── Relations: Bladder (ant.) | Rectum (post.) | Ureter (lat.)
├── Supports: Cardinal lig. (most important) + Uterosacral + Round + Broad
├── Layers: Perimetrium → Myometrium → Endometrium
├── Endometrium: Basalis (retained) + Functionalis (shed)
├── Blood: Uterine a. (from int. iliac) crosses OVER ureter
├── Lymph: Body → Para-aortic; Cervix → Internal iliac/sacral
└── Nerves: Frankenhäuser ganglion (uterovaginal plexus)
Sources: Gray's Anatomy for Students, p. 555 | Color Atlas of Human Anatomy Vol. 2 Internal Organs, pp. 454-460 | Junqueira's Basic Histology 17e, pp. 1129-1134
This is a shared conversation. Sign in to Orris to start your own chat.