Fracture neck of femur examination documentation
Reading File
Finding Sources
Finding Sources
Searching the Web
fracture neck of femur clinical examination findings documentation OSCE
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the material needed for a thorough, well-structured answer. Here is the complete clinical examination documentation for fracture neck of femur:
Fracture Neck of Femur - Clinical Examination Documentation
History
- Mechanism: Typically a low-energy fall in an elderly (often osteoporotic) female; high-energy trauma in younger patients
- Chief complaint: Severe pain in the hip/groin after a fall
- Key history point: Was the patient able to get up after the fall?
- Yes = suggests impacted fracture (some weight-bearing may still be possible)
- No, unable to move the leg = suggests unimpacted/displaced fracture
- Ask about: pre-existing osteoporosis, prior hip surgery, comorbidities (especially cardiac, renal, diabetic status for surgical risk)
A. Inspection
1. Attitude (the most diagnostically telling sign)
An elderly patient lying helplessly on the bed with the affected limb in external rotation strongly suggests fracture neck of femur.

Typical attitude of external rotation due to fracture of the femoral neck - S Das, Manual on Clinical Surgery
Differential by attitude:
| Condition | Attitude |
|---|---|
| Fracture neck of femur | Externally rotated limb, lying helpless |
| Anterior dislocation of hip | Externally rotated + abducted + slightly flexed |
| Posterior dislocation of hip | Flexed + adducted + internally rotated |
| Subtrochanteric fracture | Externally rotated, but greater trochanter immobile on rotation |
Why external rotation occurs: When the femoral neck is disrupted, the psoas major (which inserts on the lesser trochanter) loses its fulcrum at the femoral head. Its unopposed action pulls the femur proximally and into external rotation. Adductor muscle spasm further exacerbates this rotation. - Gray's Anatomy for Students, p. 784
2. Swelling and Bruising
- Haematoma may be visible over the lateral hip/thigh
- Bruising may track to the groin or lateral thigh
- Document site, extent, and colour of bruising
3. Limb Length
- The affected limb appears shortened (true shortening due to proximal displacement of the femoral shaft)
- Note: shortening is present in nearly all fractures and dislocations, except the obturator type of anterior dislocation which may show slight lengthening
B. Palpation
1. Greater Trochanter
- The greater trochanter and its relation to bony points are the keystones for diagnosis around the hip
- In fracture neck of femur: the greater trochanter is displaced upward (proximal displacement of the shaft)
- In posterior dislocation: trochanter moves toward the ASIS (due to internal rotation)
- In anterior dislocation or NOF fracture: trochanter recedes from the ASIS (due to external rotation)
Key distinguishing test - Transmitted movement:
- In fracture neck of femur: rotating the leg causes the greater trochanter to move with it (transmitted movement present)
- In subtrochanteric fracture: the greater trochanter remains immobile while the shaft of the femur is rotated (no transmitted movement)
2. Head of the Femur
- In NOF fracture: head remains in the acetabulum (it is the neck that is fractured)
- Palpate for the femoral artery at the femoral triangle - normally well-supported from behind by the femoral head. In posterior dislocation, the artery is less easily palpable
3. Tenderness
- In trochanteric fractures: bony tenderness is obvious and easily elicited
- In transcervical and subcapital fractures: tenderness is only elicited when the shaft of the femur is rotated (i.e., axial compression or rotation reproduces groin/hip pain)
- Document exact point of tenderness (groin/anterior hip region for intracapsular fractures)
C. Measurements
These are the classic clinical measurements used to document proximal femur displacement:
1. Bryant's Triangle
Patient lies supine. Three lines are drawn:
- A vertical line downward from the ASIS
- A line from the tip of the ASIS to the tip of the greater trochanter
- A horizontal line from the tip of the greater trochanter to the first vertical line
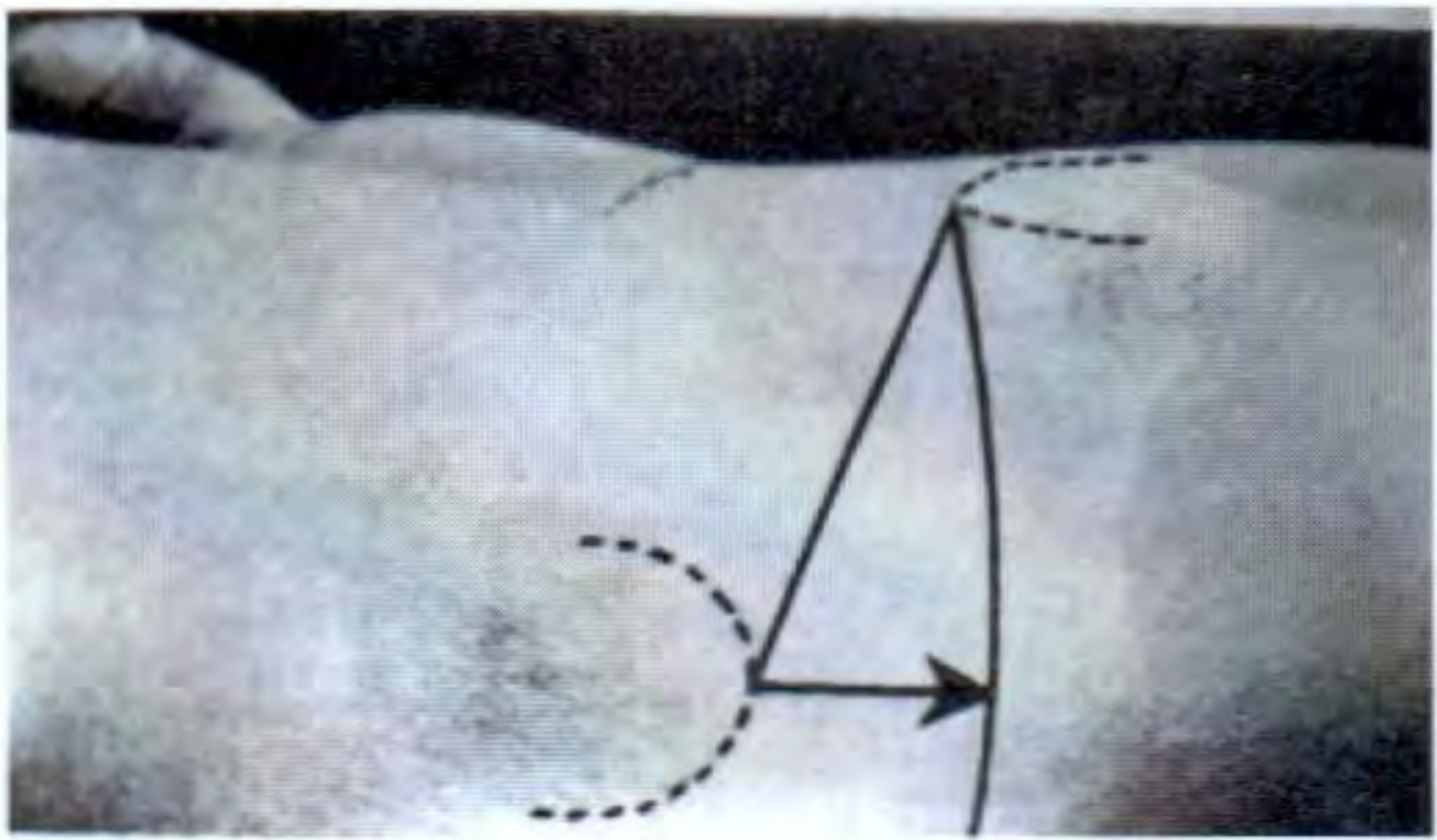
Bryant's triangle - the horizontal line is compared bilaterally - S Das, Manual on Clinical Surgery
- Shortened horizontal line = upward elevation of greater trochanter = fracture neck of femur (transcervical/subcapital) or separation of upper femoral epiphysis
- Compare both sides
2. Nelaton's Line
- Patient lies on the sound side
- A line (or tape) is placed from the most prominent part of the ischial tuberosity to the tip of the ASIS
- Normally this line touches the tip of the greater trochanter
- If the trochanter lies above this line = upward displacement (fracture NOF or hip dislocation)
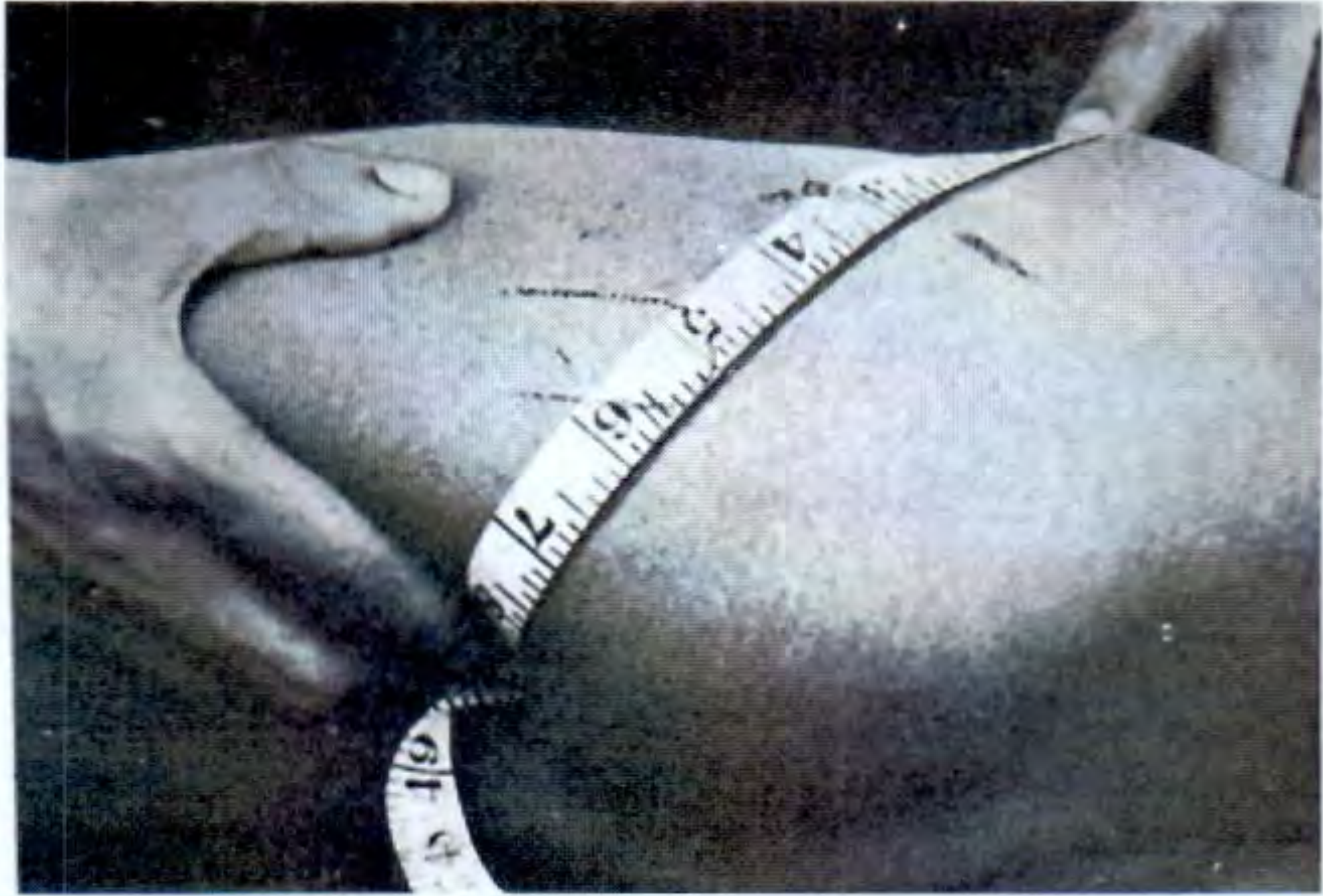
Nelaton's line measurement technique - S Das, Manual on Clinical Surgery
Advantage over Bryant's triangle: No need to compare with the other side; an absolute measurement.
3. Schoemaker's Line
- Line from the tip of the greater trochanter to the ASIS is extended anteriorly
- Normally it reaches/crosses the midline at or above the umbilicus
- If the trochanter is elevated, the line crosses the midline below the umbilicus
4. Morris' Bitrochanteric Test
- Distance from the outer border of the greater trochanter to the symphysis pubis, measured bilaterally with calipers
- Reveals medial displacement (posterior/central dislocation) or lateral displacement (anterior dislocation)
5. Chiene's Test
- A tape joining the tips of both greater trochanters should be parallel to a line joining the two ASISs
- If a trochanter is raised, these two lines are no longer parallel
6. Limb Length Measurement
- Measure from ASIS to medial malleolus (true length)
- Ensure pelvis is not tilted: the line joining both ASISs must be perpendicular to the long axis of the body before measuring
- Thigh segment: ASIS to knee joint line
- Shortening is expected in fracture NOF (typically 1-3 cm in displaced fractures)
D. Movements
- Active straight leg raise (inability): The patient is unable to lift the leg off the bed with the knee straight. This is the hallmark - absence of this ability suggests bony injury around the hip.
- Exception: In an impacted fracture of the neck of femur, some use of the limb may still be possible - do not exclude the diagnosis based on this alone.
- All hip movements are limited and painful in displaced fractures
- Passive rotation of the hip (log-roll test): any rotation of the limb causes pain - a reliable bedside test
- Document: flexion, extension, abduction, adduction, internal rotation, external rotation - all typically restricted and painful
E. Neurovascular Assessment
- Palpate femoral, popliteal, posterior tibial, and dorsalis pedis pulses
- Check capillary refill of the toes
- Assess sciatic nerve function (motor: foot dorsiflexion/plantarflexion; sensation: dorsum/sole of foot) - sciatic nerve injury is more relevant to posterior hip dislocation and subtrochanteric fracture, but must be documented
- Examine for associated injuries: ipsilateral knee, ankle, wrist (falling on outstretched hand)
F. Special Considerations
- Rectal examination: Required if central dislocation of the hip is suspected (head of femur within the pelvis). Rotating the limb during PR examination allows the femoral head to be felt moving by the examining finger.
- In elderly patients: document skin integrity (pressure areas, bruising from the fall), cognitive state, and medication history (anticoagulants, steroids, bisphosphonates)
G. Radiological Documentation
| View | Purpose |
|---|---|
| AP pelvis (both hips for comparison) | Identify fracture, displacement, Shenton's line disruption |
| Cross-table lateral | Assess posterior tilt; predict fixation failure in Garden I/II |
| Traction internal rotation view | Improves visualization of fracture line |
| MRI pelvis | Investigation of choice for occult (radiographically invisible) fractures |
| CT (trauma series) | Degree of comminution |
Pauwel's Angle (on AP view): angle between the fracture line and the horizontal plane. More vertical = mechanically less favorable = poorer prognosis with fixation.
Garden Classification (displacement):
- Stage I: Incomplete/valgus impacted
- Stage II: Complete, undisplaced
- Stage III: Complete, partially displaced
- Stage IV: Complete, fully displaced
Summary: Classic Triad on Presentation
Severe hip/groin pain + inability to weight-bear + shortened, externally rotated limb
This triad in an elderly patient after a fall is fracture neck of femur until proven otherwise.
Sources: S Das - A Manual on Clinical Surgery 13th Ed, pp. 202-205; Gray's Anatomy for Students, p. 784; Campbell's Operative Orthopaedics 15th Ed 2026
This is a shared conversation. Sign in to Orris to start your own chat.