
IMG20260616103034.jpg
Interpretation of this report with DD and approach
Reading File
Searching the Web
myeloid erythroid ratio 15:1 elevated bone marrow interpretation leukemoid reaction
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
leukemoid reaction neutrophilia differential diagnosis CML
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is the complete interpretation:
Case Interpretation - 54y/M, Peripheral Blood + Bone Marrow
Transcription of Findings
| Parameter | Finding |
|---|---|
| Age/Sex | 54-year-old Male |
| RBC (PBS) | Mild to moderate anisocytosis; predominantly MCHC (microcytic/hypochromic) with few NCNC (normochromic normocytic) cells |
| WBC (PBS) | TLC ~45,000/µL; >90% neutrophils; toxic granulation present |
| Platelets (PBS) | Adequate |
| Imp (PBS) | Neutrophilic leukocytosis |
| BM Cellularity | Hypercellular for age; particulate adequate |
| TLH | Present |
| Erythropoiesis (BM) | Maturation up to late normoblasts; predominantly micronormoblastic; dyserythropoiesis in the form of nuclear budding/karyorrhexis |
| Myelopoiesis (BM) | Maturation up to neutrophil stage |
| Megakaryocytes | Both immature and mature forms seen |
| M:E Ratio | 15.67:1 (markedly elevated; normal ~2-4:1) |
| BM Differential | Ery 6%, N 70%, Myelocyte 20%, (remaining ~4% other) |
Interpretation
This is a case of marked reactive myeloid hyperplasia (leukemoid reaction pattern) with a secondary/ineffective erythropoiesis - most likely representing a severe systemic illness (infection/sepsis/malignancy) driving a leukemoid response.
Key Observations Analyzed:
1. M:E Ratio of 15.67:1 - The Pivotal Finding
- Normal M:E = 2:1 to 4:1
- This extreme elevation (nearly 4x upper limit) reflects a massive myeloid expansion with relative erythroid suppression
- In CML, M:E is typically ≥10:1 with a classic "myelocyte bulge"
- In this case, myelocytes account for ~20% of BM cells with maturation proceeding to mature neutrophils - this is characteristic of reactive myeloid hyperplasia
2. Toxic Granulation in PBS
- Toxic granulation = coarse dark azurophilic granules in neutrophils due to retained primary granules
- This is a REACTIVE feature - seen in severe infection, sepsis, burns, inflammatory states
- In true CML, toxic granulation is typically absent
3. Dyserythropoiesis
- Nuclear budding and karyorrhexis in erythroid precursors
- The erythropoiesis is micronormoblastic, suggesting underlying iron deficiency or chronic disease limiting effective erythropoiesis
- Only 6% erythroid cells in BM (severely reduced)
4. Megakaryocytes - Both Immature and Mature
- Presence of both forms indicates active but reactive megakaryopoiesis
- In CML, megakaryocytes are classically small and hypolobated ("dwarf" megakaryocytes)
- Normal/mixed morphology favors reactive etiology
Differential Diagnosis
| Condition | Favoring This Case | Against This Case |
|---|---|---|
| Leukemoid Reaction (reactive neutrophilia) ✅ MOST LIKELY | Toxic granulation, mature neutrophils dominate, TLC 45K (not extreme), reactive megakaryocytes | Need to rule out CML |
| CML (Chronic Myeloid Leukemia) ⚠️ MUST RULE OUT | M:E ≥10:1, hypercellular BM, high M:E ratio | Toxic granulation present (seen in LR, not CML), no basophilia mentioned, megakaryocytes not described as dwarf/hypolobated |
| Chronic Neutrophilic Leukemia (CNL) | Mature neutrophilia >90% | Requires CSF3R mutation; TLC typically >25,000 with specific criteria |
| MDS/MPN with neutrophilia (atypical CML) | Dyspoiesis present | Atypical CML typically shows more dysplasia across lineages |
| Severe sepsis/infection (e.g., TB, C. diff, fungal) | Toxic granulation, leukemoid WBC | BM shows myeloid hyperplasia without leukemic features |
| Solid tumor-associated leukemoid reaction | Can mimic CML in BM | Need tumor markers, imaging |
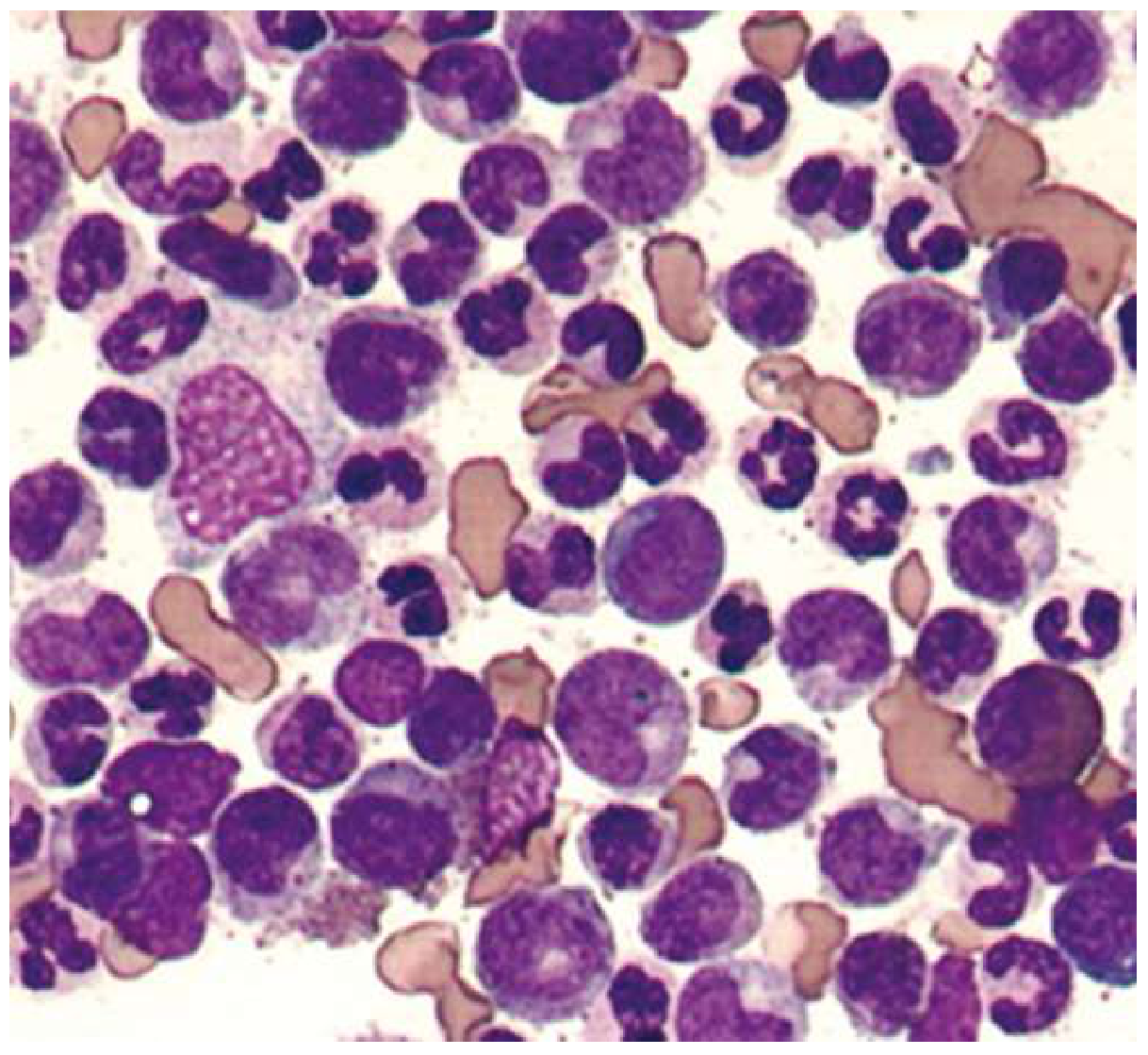
The Critical Distinguishing Test: BCR-ABL1 (Philadelphia chromosome)
As shown in the Goldman-Cecil textbook image (leukemoid reaction PBS below), morphology alone cannot distinguish leukemoid reaction from CML:
Diagnostic Approach
Urgent / Step 1 - Molecular Testing:
- BCR-ABL1 FISH / RT-PCR on peripheral blood - the single most important test
- Positive = CML (chronic phase)
- Negative = reactive/leukemoid reaction - look for cause
Step 2 - LAP Score (Leukocyte Alkaline Phosphatase):
- Leukemoid reaction: LAP score elevated (>120)
- CML: LAP score low (0-15)
- Quick, inexpensive, though less definitive than BCR-ABL
Step 3 - If BCR-ABL negative, look for underlying cause:
- Infection workup: Blood cultures, CXR/CT chest (TB, fungal), urine cultures, serology
- Inflammatory markers: CRP, ESR, procalcitonin
- Malignancy screen: CT chest/abdomen/pelvis, tumor markers (CEA, CA-125, PSA)
- Bone marrow biopsy (trephine): For reticulin fibrosis, infiltration
Step 4 - Address the anemia component:
- Serum ferritin, iron, TIBC (micronormoblastic picture suggests iron deficiency or ACD)
- Serum B12, folate (for any macrocytic contribution)
- Peripheral film for specific RBC morphology
Step 5 - If CML confirmed:
- Cytogenetics (karyotype), blast count
- Stage (chronic/accelerated/blast phase)
- Tyrosine kinase inhibitor (imatinib first-line, or nilotinib/dasatinib)
Summary Statement
This 54-year-old male has a hypercellular bone marrow with markedly elevated M:E ratio (15.67:1), myeloid hyperplasia with full maturation to neutrophils, dyserythropoiesis, and toxic granulation - a picture that fits either:
- A leukemoid reaction secondary to severe infection/inflammation/malignancy (favored by toxic granulation, mature neutrophil dominance, mixed megakaryocyte morphology), or
- CML chronic phase (cannot be excluded by morphology alone)
The BCR-ABL1 molecular test is mandatory and should be sent immediately. A low LAP score in the interim would heighten suspicion for CML. If negative, aggressive search for an underlying systemic cause (sepsis, TB, occult malignancy) is the next priority.
- Harrison's Principles of Internal Medicine 22E - "Persistent neutrophilia with cell counts ≥30,000-50,000/µL is called a leukemoid reaction... In a leukemoid reaction, the circulating neutrophils are usually mature and not clonally derived."
- Goldman-Cecil Medicine - "From this smear, it would be impossible to distinguish a leukemoid reaction from CML. Distinction would depend on determination of the presence or absence of BCR-ABL fusion."
- Quick Compendium of Clinical Pathology 5th ed. - "In CML, the LAP score is typically low, between 0 and 15... Leukemoid reaction (reactive neutrophilia) is associated with an elevated LAP score."
Approach to Erythrocytosis in PS
Reading File
Finding Sources
Finding Sources
Searching the Web
erythrocytosis approach diagnosis JAK2 EPO polycythemia vera secondary 2024 guidelines
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
I now have comprehensive textbook data to construct a detailed answer. Here it is:
Approach to Erythrocytosis on Peripheral Smear (PS)
Definition
Erythrocytosis = an increase in red cell mass beyond normal, reflected on peripheral smear as packed/crowded red cells with reduced plasma background, or confirmed biochemically as:
- Hb >16.5 g/dL in men / >16.0 g/dL in women
- Hct >49% in men / >48% in women
- Or red cell mass >25% above mean normal predicted value
"Unless the hemoglobin level is ≥20 g/dL (Hct ≥60%), it is not possible to distinguish true erythrocytosis from disorders causing plasma volume contraction."
- Harrison's Principles of Internal Medicine 22E
Step 1 - The Primary Classification: Relative vs. Absolute
ERYTHROCYTOSIS ON PS
│
▼
Is the RBC mass truly elevated?
│
┌────┴────┐
▼ ▼
RELATIVE ABSOLUTE
Relative (Spurious/Apparent) Erythrocytosis
- RBC mass is NORMAL - only plasma volume is reduced
- Also called Gaisböck's syndrome / stress erythrocytosis / pseudopolycythemia
- Causes:
- Acute: dehydration (vomiting, diarrhea, burns, diuretics)
- Chronic: hypertension, tobacco, ethanol abuse, obesity, androgens
Henry's Clinical Diagnosis - "Relative polycythemia refers to an increase in Hct or red cell count as a result of decreased plasma volume; total red cell mass is not increased."
Key point: In PV specifically, plasma volume is paradoxically EXPANDED, which can actually mask the elevated red cell mass - making red cell mass + plasma volume determinations important in borderline cases.
Step 2 - If Absolute Erythrocytosis: Primary vs. Secondary
ABSOLUTE ERYTHROCYTOSIS
│
┌─────┴──────┐
▼ ▼
PRIMARY SECONDARY
(EPO- (EPO-
independent) driven)
│ │
PV + ┌───┴────┐
congenital ▼ ▼
APPRO- INAPPROP-
PRIATE RIATE
(hypoxia) (ectopic)
A. Primary Erythrocytosis (EPO-independent)
| Condition | Mechanism | Marker |
|---|---|---|
| Polycythemia Vera (PV) | Clonal HSC - constitutive JAK2 activation | JAK2 V617F (>95%) or JAK2 exon 12 (<5%) |
| Familial erythrocytosis | EPO receptor mutations (EPOR) | Family history, low EPO |
| LNK mutations | JAK2 signaling amplifier | Rare, JAK2 wild-type |
B. Secondary Erythrocytosis - Appropriate (Hypoxia-driven, EPO elevated)
| Cause | Notes |
|---|---|
| Chronic pulmonary disease (COPD, ILD) | SaO2 <92% |
| High altitude | Physiologic adaptation |
| Right-to-left cardiac/vascular shunts | Congenital heart disease |
| Sleep apnea syndrome | Nocturnal desaturations |
| Carbon monoxide poisoning / heavy smoking | CO-Hb displaces O2 |
| High-oxygen-affinity hemoglobin variants | Normal SaO2, but O2 not released to tissues |
| Hepatopulmonary syndrome |
C. Secondary Erythrocytosis - Inappropriate (EPO ectopic/non-hypoxic)
| Cause | Notes |
|---|---|
| Renal cell carcinoma | ~3% cause erythrocytosis |
| Hepatocellular carcinoma | ~10% |
| Cerebellar hemangioblastoma | ~15% |
| Uterine myoma, adrenal tumors, meningioma, pheochromocytoma | Rare |
| Renal artery stenosis, renal cysts, Bartter's syndrome | Local renal ischemia → EPO |
| Post-renal transplant | ~10-15% of transplants |
| Drugs - Androgens, exogenous EPO, SGLT2 inhibitors, testosterone | Always take drug history |
D. Congenital/Familial (EPO pathway mutations)
| Gene | Mechanism |
|---|---|
| VHL (Chuvash polycythemia) | Loss of HIF-1α degradation → excess EPO |
| PHD2 (EGLN1) | Same pathway as VHL |
| HIF-2α (EPAS1) | Constitutive HIF activation |
| 2,3-BPG mutase | Altered O2 dissociation curve |
Step 3 - The Diagnostic Algorithm
Initial Assessment
- Repeat CBC - confirm persistent elevation (exclude lab error)
- Clinical history - smoking, altitude, drugs (androgens, EPO, SGLT2i), renal disease, family history
- Examination - splenomegaly? aquagenic pruritus? plethora? erythromelalgia? thrombosis history?
Step 4 - Two Pivotal Tests (run simultaneously)
┌─────────────────────┐
│ Serum EPO + JAK2 │
│ V617F mutation │
└──────────┬──────────┘
│
┌───────────┼───────────┐
▼ ▼ ▼
EPO low EPO normal EPO high
JAK2 +ve JAK2 -ve JAK2 -ve
│ │ │
▼ ▼ ▼
PV Check O2 Secondary
(see WHO Sat + check cause
criteria) congenital (hypoxia
mutations or ectopic)
Important caveat from Harrison's 22E:
"A normal serum erythropoietin level does not exclude the presence of PV, but an elevated erythropoietin level is most consistent with a secondary cause."
"Not everyone expressing a low JAK2 V617F quantitative mutation allele burden (VAF ≤5%) actually has a blood disease."
Arterial Blood Gas / Pulse Oximetry
- SaO2 <92% → hypoxic secondary erythrocytosis
- If SaO2 normal but EPO elevated → check for high-affinity Hb variants (P50), ectopic EPO sources
Step 4 - WHO 2016 Diagnostic Criteria for PV (if suspected)
Diagnosis requires: All 3 Major, OR Major 1+2 + Minor
| Criterion | |
|---|---|
| Major 1 | Hb >16.5 g/dL (men) / >16.0 g/dL (women) OR Hct >49%/48% OR red cell mass >25% predicted |
| Major 2 | BM biopsy: hypercellularity for age with trilineage growth (panmyelosis) - prominent erythroid + granulocytic + megakaryocytic proliferation with pleomorphic mature megakaryocytes |
| Major 3 | JAK2 V617F or JAK2 exon 12 mutation |
| Minor | Subnormal serum EPO level |
(Washington Manual of Medical Therapeutics / Quick Compendium of Clinical Pathology)
Step 5 - Peripheral Smear Specific Findings
| PS Finding | Interpretation |
|---|---|
| Packed RBCs, reduced plasma gaps | Erythrocytosis (any cause) |
| Microcytic RBCs with erythrocytosis | β-thalassemia trait, hypoxic erythrocytosis, or PV (iron deficient) |
| Elevated RDW with erythrocytosis | Hypoxic erythrocytosis or PV (iron deficiency component) |
| Leukocytosis + thrombocytosis + erythrocytosis | PV (panmyelosis pattern) |
| Tear-drop cells + nucleated RBCs + leukoerythroblastosis | Post-PV myelofibrosis |
| Normal WBC, normal platelets, isolated erythrocytosis | Secondary cause more likely |
Harrison's 22E - "Only three situations cause microcytic erythrocytosis: β-thalassemia trait, hypoxic erythrocytosis, and PV. With β-thalassemia trait, RDW is usually normal; with hypoxic erythrocytosis or PV, RDW may be elevated due to associated iron deficiency."
Step 6 - Further Workup Based on Pathway
If PV confirmed:
- BM biopsy (panmyelosis + pleomorphic megakaryocytes)
- Risk stratification (age >60 or prior thrombosis = high risk)
- Treatment: phlebotomy (target Hct <45%), low-dose aspirin, hydroxyurea (high risk)
- JAK2 inhibitor (ruxolitinib) for refractory/symptomatic disease
If secondary (hypoxic):
- PFTs, overnight oximetry (sleep study), echo (R→L shunt)
- Treat underlying cause; phlebotomy only for symptomatic hyperviscosity
If secondary (ectopic EPO):
- CT chest/abdomen/pelvis
- Renal Doppler (renal artery stenosis)
- Liver function + AFP (HCC)
- MRI head (cerebellar hemangioblastoma)
If congenital suspected (young patient, family history, JAK2-negative):
- P50 determination (high-affinity Hb)
- VHL sequencing, PHD2, EPAS1 mutations
- Genetic counseling
Summary Flowchart
Elevated Hb/Hct on PS
↓
Is Hb ≥20 g/dL?
No → Measure red cell mass + plasma volume
(or use clinical + lab clues)
↓
Relative? → Treat cause (dehydration/drugs)
↓
Absolute confirmed
↓
Serum EPO + JAK2 V617F
↓
┌─────────────────────────────────────────┐
│ EPO low + JAK2+ → PV (confirm with WHO │
│ criteria, BM if needed│
│ EPO high + JAK2- → Secondary erythrocytosis
│ → SaO2 check:
│ Low SaO2 → Hypoxic (COPD, OSA, altitude, CHD)
│ Normal SaO2 → Ectopic EPO (renal/hepatic tumor,
│ high-affinity Hb, renal disease)
│ or congenital (VHL, PHD2, EPAS1)
│ EPO normal + JAK2-→ Borderline/congenital/relative
│ → JAK2 exon 12, LNK mutation
│ → P50, VHL sequence
└─────────────────────────────────────────┘
Sources: Harrison's Principles of Internal Medicine 22E, p. 863 | Washington Manual of Medical Therapeutics | Henry's Clinical Diagnosis and Management by Laboratory Methods | Goldman-Cecil Medicine | Textbook of Family Medicine 9e
Causes of neutrophilic leucocytosis
Finding Sources
Searching the Web
causes neutrophilic leukocytosis classification mechanisms pathophysiology hematology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the textbook data needed for a thorough, well-organized answer.
Causes of Neutrophilic Leukocytosis
Definition
Neutrophilic leukocytosis (neutrophilia) = absolute neutrophil count (ANC) >7,500 cells/mm³
When WBC >50,000/µL with a marked left shift, it is termed a leukemoid reaction.
Mechanisms (Pathophysiologic Basis)
Before listing causes, it helps to understand the four mechanisms - because each cause acts through one or more of these:
| Mechanism | How | Examples |
|---|---|---|
| 1. Increased BM production | Growth factor-driven expansion of myeloid pool | Infection, chronic inflammation, G-CSF, CML |
| 2. Increased release from BM storage pool | Rapid egress of mature neutrophils from marrow reserve | Acute infection (endotoxin), glucocorticoids, thermal injury |
| 3. Decreased margination (demargination) | Shift of neutrophils from marginal pool to circulating pool | Epinephrine, exercise, stress, corticosteroids, LAD |
| 4. Decreased extravasation into tissues | Reduced exit from blood into tissue | Glucocorticoids |
Robbins & Kumar Pathologic Basis of Disease - "In acute infection there is a rapid increase in the egress of mature granulocytes from the bone marrow pool, mediated through effects of TNF and IL-1. If infection is prolonged, IL-1, TNF, and inflammatory mediators stimulate macrophages and marrow stromal cells to produce increased hematopoietic growth factors."
Henry's Clinical Diagnosis - "An increase in immature peripheral blood granulocytes is termed a 'shift to the left.' Increased WBCs with left shift and toxic features may resemble leukemia - termed a 'leukemoid reaction.'"
Causes - Organized by Category
1. INFECTIONS (Most Common Cause)
| Type | Examples |
|---|---|
| Bacterial (pyogenic) - most potent stimulus | Staphylococcus, Streptococcus, pneumococcal pneumonia, urinary tract infection, appendicitis, cholecystitis, meningitis |
| Special organisms causing leukemoid reactions | Clostridioides difficile, tuberculosis (WBC can exceed 30,000/µL in ~25%) |
| Fungal | Candida, Aspergillus (immunocompromised) |
| Parasitic | Less common; more typically cause eosinophilia |
| Viral | Generally NOT a cause of neutrophilia (cause lymphocytosis); exceptions: early viral illness |
| Overwhelming/severe infection | May paradoxically cause neutropenia (supply cannot meet demand) |
"Pyogenic bacteria especially induce neutrophilia. More virulent agents result in higher neutrophil counts; when the infection is overwhelming, toxic neutropenia with a shift to the left can occur, more commonly in the elderly." - Henry's Clinical Diagnosis
2. INFLAMMATION / TISSUE NECROSIS
| Condition | Notes |
|---|---|
| Myocardial infarction | Sterile necrosis; peaks 12-24h post-MI |
| Burns / thermal injury | Both acute release + increased production |
| Pulmonary infarction | |
| Surgical trauma / crush injury | Transient demargination then production |
| Collagen vascular diseases | RA, juvenile RA (Still's disease), SLE |
| Inflammatory bowel disease | Crohn's, ulcerative colitis |
| Granulomatous disease | Sarcoidosis, granulomatous hepatitis |
| Chronic hepatitis | |
| Adult-onset Still's disease | Classic: spiking fever + salmon rash + arthritis + neutrophilic leukocytosis |
| Hypersensitivity states | Vasculitis, serum sickness |
3. DRUGS
| Drug | Mechanism |
|---|---|
| Corticosteroids | Demargination + increased BM release + decreased tissue extravasation |
| Epinephrine / β-agonists | Demargination (shift from marginal to circulating pool) |
| G-CSF / GM-CSF (recombinant) | Direct stimulation of BM production |
| Lithium | G-CSF agonist properties → stimulates neutrophil production |
| NSAIDs | Mild demargination |
4. PHYSIOLOGIC / TRANSIENT CAUSES
| Cause | Mechanism |
|---|---|
| Vigorous exercise | Demargination (epinephrine surge) |
| Emotional stress / excitement | Catecholamine-mediated demargination |
| Pregnancy (especially labor) | Increased production + demargination |
| Neonatal period | Physiologically elevated at birth |
| Cigarette smoking | Neutrophilia in 25-50% chronic smokers; persists up to 5 years after cessation |
5. METABOLIC DISORDERS
| Condition | Notes |
|---|---|
| Diabetic ketoacidosis (DKA) | Even without infection; can reach 20,000-25,000/µL |
| Acute renal failure / uremia | |
| Eclampsia | |
| Acute poisoning | |
| Acute gout attack | Neutrophilia + neutrophilic synovial fluid |
| Thyroid storm |
6. HEMATOLOGIC / MARROW STIMULATION
| Condition | Notes |
|---|---|
| Hemolytic anemia | Compensatory marrow stimulation → spills neutrophils |
| Immune thrombocytopenia (ITP) | Same mechanism |
| Recovery from marrow suppression | Rebound leukocytosis post-chemotherapy, post-aplasia |
| Post-splenectomy | Loss of splenic filtration/margination; persistent mild neutrophilia |
| Acute hemorrhage | Bone marrow response + demargination |
7. MALIGNANCIES
| Type | Notes |
|---|---|
| Solid tumors secreting G-CSF/GM-CSF/IL-6 | Lung, GI, kidney, urothelial, tongue cancers - paraneoplastic neutrophilia |
| Hodgkin lymphoma | Cytokine-secreting tumor |
| Marrow metastasis (myelophthisis) | Leukoerythroblastic reaction |
| Hepatocellular carcinoma | Ectopic G-CSF production |
8. PRIMARY HEMATOLOGIC (NEOPLASTIC / CONGENITAL)
Acquired (Clonal)
| Disease | Key Feature |
|---|---|
| Chronic Myeloid Leukemia (CML) | BCR-ABL1 positive; M:E ≥10:1; myelocyte bulge; basophilia; LOW LAP score |
| Polycythemia Vera (PV) | Panmyelosis; JAK2+ ; HIGH LAP score |
| Primary Myelofibrosis | Leukoerythroblastosis; tear-drop cells |
| Chronic Neutrophilic Leukemia (CNL) | Mature neutrophilia >80%; CSF3R mutation |
| Atypical CML / MDS-MPN | BCR-ABL negative; dysplasia |
Congenital/Hereditary
| Condition | Mechanism |
|---|---|
| Leukocyte Adhesion Deficiency (LAD) 1, 2, 3 | Neutrophils cannot exit blood into tissues (CD18/CD11b defect) → marked neutrophilia with recurrent infections despite high WBC |
| Hereditary neutrophilia | Rare autosomal dominant |
| Down syndrome | Transient neonatal myeloproliferation |
| Chronic idiopathic neutrophilia | Diagnosis of exclusion |
Peripheral Smear Clues with Neutrophilia
| PS Feature | Significance |
|---|---|
| Toxic granulation | Severe reactive (infection, sepsis) - NOT CML |
| Döhle bodies | Reactive - pale blue cytoplasmic inclusions |
| Cytoplasmic vacuoles | Reactive, especially bacterial sepsis |
| Left shift (bands, metamyelocytes) | Reactive or early CML |
| Myelocyte "bulge" | CML (myelocytes > metamyelocytes in DLC) |
| Basophilia | Strongly suggests CML |
| No toxic changes, no basophilia | Favors primary/clonal cause |
| Tear-drop RBCs + nucleated RBCs | Myelophthisis / myelofibrosis |
Quick Memory Aid - "INDIA MEN"
| Letter | Category |
|---|---|
| I | Infection (bacterial, fungal) |
| N | Necrosis (MI, burns, infarction) |
| D | Drugs (steroids, G-CSF, lithium, epinephrine) |
| I | Inflammation (RA, IBD, Still's, granulomatous) |
| A | Autoimmune / connective tissue |
| M | Metabolic (DKA, renal failure, eclampsia) |
| E | Exercise / physiologic (stress, pregnancy, smoking) |
| N | Neoplasm (CML, PV, solid tumors - paraneoplastic) |
Sources: Harrison's Principles of Internal Medicine 22E, Table 67-2 | Robbins & Kumar Pathologic Basis of Disease, Tables 13.2 & 13.3 | Goldman-Cecil Medicine, Table 153-1 | Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.