If adenocarcinoma of stomach spreaded into periotoneum then what are the next steps procedures and prognosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
gastric cancer peritoneal metastasis treatment
Finding Sources
Finding Sources
Searching PubMed
gastric cancer peritoneal carcinomatosis HIPEC cytoreductive surgery
Reading File
Reading File
Reading Article
PMID: 39644811
Reading Article
PMID: 37906724
Reading File
Finding Sources
Reading Article
PMID: 39600651
Reading File
Finding Sources
Reading File
Searching the Web
gastric adenocarcinoma peritoneal metastasis treatment guidelines 2024 immunotherapy prognosis
Loading Image
Here is a comprehensive, evidence-based overview of gastric adenocarcinoma with peritoneal spread.
Gastric Adenocarcinoma with Peritoneal Spread — Management & Prognosis
Peritoneal spread classifies the disease as Stage IV (M1) under AJCC/TNM staging. It represents one of the most common and most lethal patterns of metastasis in gastric cancer, and systemic treatment is generally the standard of care, with surgery reserved for highly selected patients.
Step 1 — Initial Workup & Staging Laparoscopy
Before committing to any treatment strategy, peritoneal disease extent must be formally characterized:
- Staging laparoscopy is imperative to evaluate the extent of peritoneal spread. It allows calculation of the Peritoneal Cancer Index (PCI) score — a validated tool that scores 13 abdominal regions (0–3 per region, max 39).
- Biopsy confirmation of peritoneal deposits establishes histologic proof.
- Molecular profiling should be performed simultaneously:
- HER2 status (IHC/FISH) — overexpressed in 7–34% of gastric adenocarcinomas
- PD-L1 CPS (Combined Positive Score)
- MSI/MMR status
- VEGFR2 expression
- Cross-sectional imaging (CT chest/abdomen/pelvis) to rule out other distant metastases.
Step 2 — Treatment Decision Based on Disease Volume
A. Limited Peritoneal Disease (PCI ≤ 7) — Aggressive Multimodal Approach
Highly selected patients with low-volume peritoneal carcinomatosis (PCI ≤ 7) may be candidates for:
Cytoreductive Surgery (CRS) + HIPEC:
- CRS involves gastrectomy with D2 lymphadenectomy + resection of all visible peritoneal deposits (omentectomy, peritonectomy of involved surfaces).
- The goal is complete cytoreduction (CC-0) — no visible residual disease.
- HIPEC (Hyperthermic Intraperitoneal Chemotherapy) is administered intraoperatively at 42°C for 60–90 minutes. The rationale is that systemic chemotherapy has poor peritoneal penetration, while heated IP drug delivery achieves high local concentrations.
- HIPEC regimens (from a 2024 Bayesian network meta-analysis of 11 RCTs, n=1,092): cisplatin alone showed the best overall survival benefit (HR 0.52, 95%CI 0.38–0.73); cisplatin + fluorouracil and oxaliplatin + 5-FU also showed benefit. Cisplatin + mitomycin C was used in the GASTRIPEC-I trial (15 mg/m² MMC + 75 mg/m² cisplatin, 60 min at 42°C). [PMID 39600651]
⚠ Critical note: The Phase III GASTRIPEC-I trial (JCO 2024, PMID 37906724) — 105 patients, CRS+HIPEC vs. CRS alone — found no OS difference (median OS 14.9 months in both arms), though PFS (7.1 vs. 3.5 months, p=0.047) and distant MFS favored CRS+HIPEC. The trial stopped early due to slow recruitment, limiting conclusions. A 2025 meta-analysis of 53 studies (n=2,446) confirmed that combined IP + systemic chemotherapy confers a survival benefit over systemic therapy alone (HR 0.57, 95%CI 0.48–0.67, p<0.001). [PMID 39644811]
These patients should be referred to high-volume centers with multidisciplinary gastric cancer teams.
B. Extensive Peritoneal Disease (PCI > 7) or Poor Performance Status — Palliative Systemic Chemotherapy
This is the standard for most patients. Systemic chemotherapy improves both survival and quality of life compared to best supportive care alone. — Sleisenger & Fordtran's, p. 979
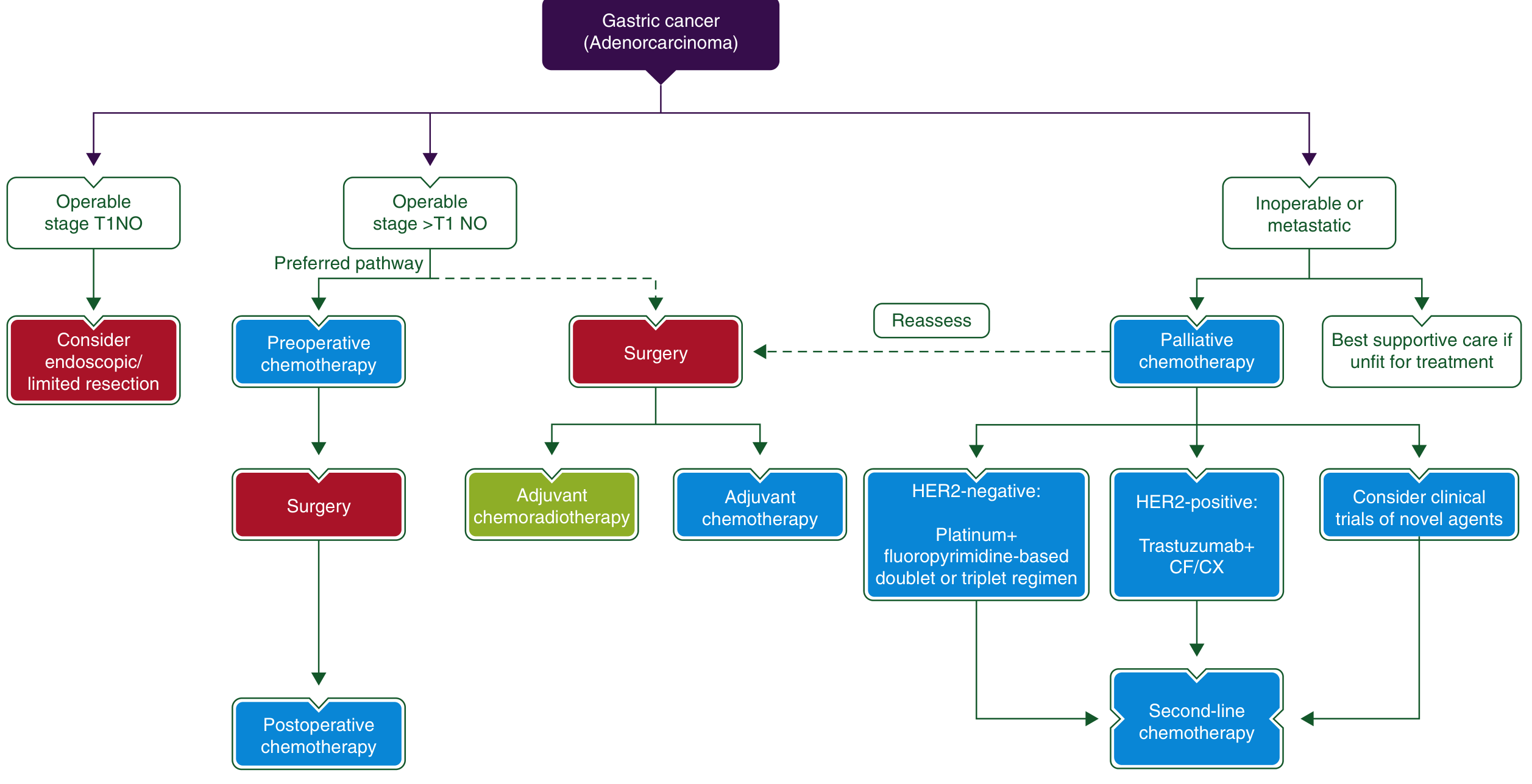
First-line regimens:
| Scenario | Regimen | Evidence |
|---|---|---|
| HER2-negative | Platinum + fluoropyrimidine doublet (FOLFOX, CAPOX) ± docetaxel | Phase III trials |
| HER2-positive | Trastuzumab + cisplatin/capecitabine or 5-FU | ToGA trial: mOS 13.8 vs. 11.1 months |
| PD-L1 CPS ≥ 5 | Nivolumab + chemotherapy (CheckMate 649) | Approved 1st line |
| MSI-H / dMMR | Pembrolizumab ± chemotherapy | High response rates |
| All | EOX (epirubicin + oxaliplatin + capecitabine): median OS 11.2 months, non-inferior to cisplatin-based regimens | Phase III |
FLOT regimen (docetaxel + oxaliplatin + fluorouracil/leucovorin) is the preferred perioperative regimen when surgery is anticipated (FLOT4-A10 trial).
Second-line chemotherapy: Docetaxel or irinotecan monotherapy is superior to best supportive care. Ramucirumab (anti-VEGFR2) ± paclitaxel is a validated second-line option.
C. Intraperitoneal Chemotherapy Without Surgery
For patients not candidates for CRS, catheter-based normothermic IP chemotherapy or PIPAC (Pressurized Intraperitoneal Aerosol Chemotherapy) are investigational options administered via repeat laparoscopy. In the 2025 meta-analysis, ~27% of patients achieved complete peritoneal disease regression with IP chemotherapy alone. [PMID 39644811]
D. Best Supportive Care
For patients with poor ECOG performance status (≥3), significant comorbidities, or patient preference — aggressive chemotherapy offers limited benefit and best supportive care (nutritional support, analgesics, management of ascites) is appropriate.
Step 3 — Complications Requiring Management
Peritoneal spread frequently causes:
- Malignant ascites — therapeutic paracentesis; bevacizumab (off-label) may reduce re-accumulation
- Bowel obstruction — stenting vs. palliative bypass vs. venting gastrostomy
- Nutritional failure — parenteral nutrition or jejunal feeding tube
- Pain — WHO analgesic ladder; consider celiac plexus block
Prognosis
| Scenario | Median Overall Survival |
|---|---|
| Stage IV metastatic (all comers) | ~8–13 months with combination chemotherapy |
| Peritoneal metastasis + systemic chemo alone | ~6–8 months |
| CRS + HIPEC (selected patients, complete cytoreduction) | ~14.9 months (GASTRIPEC-I) |
| CRS + HIPEC phase II (PCI ≤ 7, complete resection) | ~25 months (2.1 years) |
| HER2+ receiving trastuzumab | ~13.8 months |
| MSI-H receiving immunotherapy | Better outcomes; data maturing |
| Best supportive care only | ~3–5 months |
Key prognostic factors: completeness of cytoreduction (CC-0 vs CC-1/2), PCI score, performance status, HER2/PD-L1/MSI status, number of involved peritoneal regions, response to induction chemotherapy.
Summary Algorithm
- Staging laparoscopy + molecular profiling → calculate PCI
- PCI ≤ 7, good PS, respond to induction chemo → consider CRS + HIPEC at specialized center (within clinical trial if possible)
- PCI > 7 or unresectable → palliative systemic chemotherapy guided by HER2/PD-L1/MSI status
- HER2+ → add trastuzumab; PD-L1 CPS ≥ 5 → add nivolumab; MSI-H → immunotherapy
- Progression on 1st line → 2nd-line chemotherapy (ramucirumab ± paclitaxel, docetaxel, irinotecan)
- Enroll in clinical trials at every step
Sources:
- Current Surgical Therapy 14e, pp. 145–150
- Sleisenger and Fordtran's GI and Liver Disease, pp. 979–980
- GASTRIPEC-I Phase III RCT — PMID 37906724 (JCO 2024)
- Boshier et al. Meta-analysis of IP chemotherapy — PMID 39644811 (EJSO 2025)
- Wang et al. HIPEC regimens Bayesian meta-analysis — PMID 39600651 (Front Oncol 2024)
This is a shared conversation. Sign in to Orris to start your own chat.