Is ulcerative colitis curable
Reading File
Searching PubMed
"ulcerative colitis" AND cure OR remission
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have all the information needed for a thorough answer.
Is Ulcerative Colitis Curable?
The short answer: Yes, but only by surgery. Medical therapy cannot cure UC - it manages and suppresses the disease. Surgical removal of the colon and rectum is considered curative.
Medical Treatment - Controls but Does Not Cure
The goal of all drug therapy is to induce and maintain remission while healing the mucosa - not to eliminate the disease permanently. Once medications are stopped, UC can relapse. The main drug categories are:
| Category | Examples | Role |
|---|---|---|
| 5-Aminosalicylates (5-ASA) | Mesalamine, sulfasalazine, balsalazide | Mild-moderate disease; remission maintenance |
| Corticosteroids | Prednisone, budesonide, IV methylprednisolone | Flare control only; NOT for long-term use |
| Immunomodulators | Azathioprine, mercaptopurine, ozanimod | Moderate-severe disease; steroid-sparing |
| JAK inhibitors | Tofacitinib, upadacitinib | Moderate-severe disease |
| Biologics | Infliximab, adalimumab, vedolizumab, ustekinumab, golimumab | Moderate-severe or biologic-eligible disease |
A 2024 AGA network meta-analysis (PMID 39425738) compared the comparative efficacy of all advanced therapies, confirming that biologics and JAK inhibitors are the most effective at inducing remission in moderate-severe UC - but again, remission is not the same as cure.
Surgery - The Only Cure
As stated directly in Goldman-Cecil Medicine: "For ulcerative colitis, colectomy is a curative procedure."
- About 10% of patients will require surgery within 10 years (down significantly from historical rates due to better biological therapies - roughly 3% at 1 year, 7% at 5 years, 10% at 10 years)
- Indications for surgery include: toxic megacolon, severe fulminant attack unresponsive to medical therapy, medically refractory disease, uncontrolled hemorrhage, perforation, or colorectal cancer risk
- The standard procedure is total proctocolectomy (removal of the entire colon and rectum), which eliminates UC permanently since the disease is confined to the colon
Two main surgical options:
- Proctocolectomy + Brooke (end) ileostomy - permanent ileostomy through the abdominal wall; definitive and curative
- Restorative proctocolectomy with ileal pouch-anal anastomosis (IPAA / J-pouch) - the distal 30 cm of ileum is fashioned into a pouch and pulled through the anal canal, preserving continence and avoiding a permanent stoma. This is the preferred option for most patients who are good surgical candidates
A known complication of IPAA is pouchitis (inflammation of the ileal pouch), occurring in some patients after surgery, treated with antibiotics (metronidazole or ciprofloxacin).
Key Contrast with Crohn's Disease
This is a clinically important distinction:
- UC: colectomy IS curative - the disease cannot recur once the colon is removed (it is confined entirely to the colon)
- Crohn's disease: surgery is NOT curative - recurrence after resection is common (~25% need repeat surgery within 10 years), because Crohn's can affect any part of the GI tract from mouth to anus
Bottom Line
| Approach | Outcome |
|---|---|
| Medical therapy alone | Remission possible, but disease persists; relapse common if therapy stopped |
| Surgery (proctocolectomy) | Curative - eliminates UC permanently |
The decision to proceed with surgery is individualized and requires specialist consultation, but for appropriate patients - particularly those with refractory disease or high cancer risk - surgery offers a definitive cure.
- Goldman-Cecil Medicine, 26th Edition, Chapter 127 (Inflammatory Bowel Disease)
- Schwartz's Principles of Surgery, 11th Edition
Fecal calprotectin increased in which condition above 150
Finding Sources
Searching PubMed
"fecal calprotectin" AND "150" AND inflammatory bowel disease
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
The diagnostic algorithm image perfectly answers the question. Here is the complete answer:
Fecal Calprotectin >150 µg/g: Organic Disease (IBD / Colorectal Cancer)
The 150 µg/g threshold is a key decision point in the fecal calprotectin diagnostic algorithm. Here is the full interpretation:
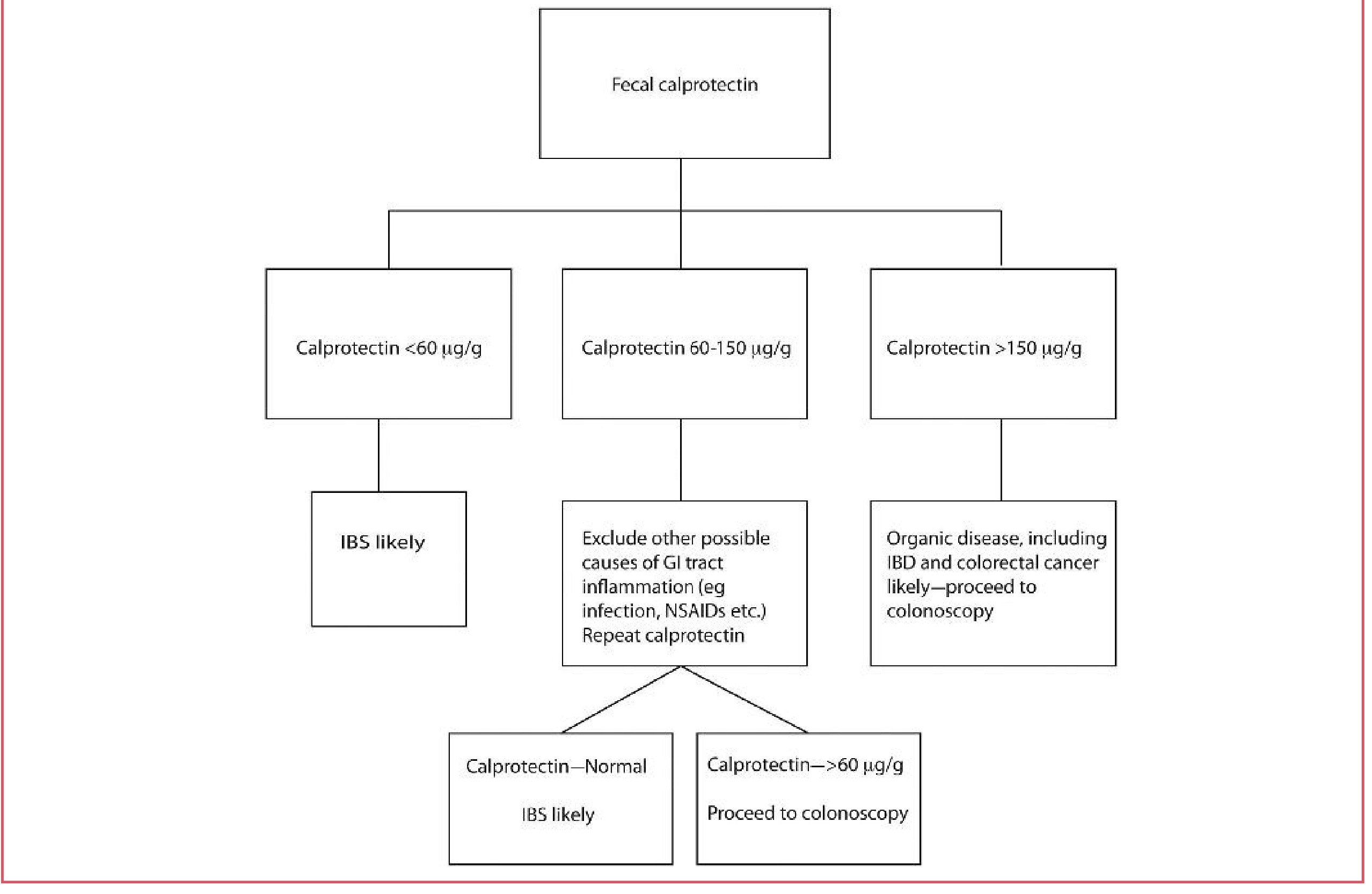
Source: Tietz Textbook of Laboratory Medicine, 7th Edition
The Three Zones
| Level | Interpretation | Action |
|---|---|---|
| < 60 µg/g | IBS likely | No further workup needed |
| 60 - 150 µg/g | Indeterminate - exclude other GI inflammation causes (infection, NSAIDs) | Repeat calprotectin |
| > 150 µg/g | Organic disease likely - IBD or colorectal cancer | Proceed to colonoscopy |
Conditions Causing Fecal Calprotectin >150 µg/g
The main conditions are:
-
Inflammatory Bowel Disease (IBD)
- Ulcerative Colitis - active mucosal inflammation
- Crohn's Disease - active luminal inflammation
-
Colorectal Cancer - mucosal disruption triggers neutrophil influx
-
Other causes that can raise calprotectin in this range:
- GI infections (bacterial, parasitic)
- NSAID-induced enteropathy
- Colorectal polyps
- Microscopic colitis
Clinical Utility
-
Calprotectin <50 µg/g rules out moderate-to-severe intestinal inflammation with >95% accuracy
-
Sensitivity is optimized at a threshold of 50 µg/g; specificity for confirming active inflammation peaks at ~250 µg/g
-
At <50 µg/g, a patient has only a 1-4% chance of having IBD
-
It is most useful for distinguishing IBD from IBS - calprotectin is typically normal in IBS (a functional, non-inflammatory disorder)
-
In active UC, calprotectin also correlates with endoscopic findings and degree of mucosal healing, making it useful for monitoring treatment response
-
Tietz Textbook of Laboratory Medicine, 7th Edition
-
Yamada's Textbook of Gastroenterology, 7th Edition
-
Mulholland and Greenfield's Surgery, 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.