drugs for htn
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "antihypertensive" AND "treatment"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete, organized overview of antihypertensive drugs:
Drugs for Hypertension
Definition: HTN = SBP >130 mmHg or DBP >80 mmHg on at least two occasions. BP goal for most patients is <130/80 mmHg.
First-line choices (most guidelines): Thiazide diuretics, ACE inhibitors, ARBs, Calcium Channel Blockers (CCBs). Beta-blockers are used when there is a compelling indication (e.g. heart failure, post-MI, angina).
1. Diuretics
All diuretics initially lower BP by reducing blood volume (Na+ and water excretion), which decreases cardiac output. With long-term use, a reduction in peripheral vascular resistance also contributes.
A. Thiazide diuretics (First-line)
| Drug | Brand |
|---|---|
| Hydrochlorothiazide | Microzide |
| Chlorthalidone | (generic) |
| Indapamide | (generic) |
| Metolazone | Zaroxolyn |
- Mechanism: Inhibit Na+/Cl- cotransporter in distal convoluted tubule
- Advantage: Useful in combination with beta-blockers, ACEi, ARBs, K+-sparing diuretics
- Caution: NOT effective if GFR <30 mL/min/m² (except metolazone)
- Side effects: Hypokalemia, hyperuricemia (gout), hyperglycemia
B. Loop diuretics
| Drug | Brand |
|---|---|
| Furosemide | Lasix |
| Bumetanide | Bumex |
| Torsemide | Demadex |
| Ethacrynic acid | Edecrin |
- Use: When thiazides are ineffective (CKD, GFR <30), or in heart failure with fluid overload
- Side effects: Hypokalemia, ototoxicity (especially ethacrynic acid)
C. Potassium-sparing diuretics
| Drug | Brand |
|---|---|
| Spironolactone | Aldactone |
| Eplerenone | Inspra |
| Amiloride | Midamor |
| Triamterene | Dyrenium |
- Spironolactone/Eplerenone = aldosterone receptor antagonists; used in resistant HTN, heart failure, post-MI
- Side effects: Hyperkalemia; spironolactone causes gynecomastia (eplerenone is more selective, less so)
2. ACE Inhibitors (ACEi)
| Drug | Brand |
|---|---|
| Lisinopril | Prinivil, Zestril |
| Enalapril | Vasotec |
| Ramipril | Altace |
| Benazepril | Lotensin |
| Captopril | Capoten |
| Fosinopril | Monopril |
| Quinapril | Accupril |
- Mechanism: Block conversion of Ang I → Ang II; reduce aldosterone → reduced Na+ retention and vasoconstriction. Also increase bradykinin levels.
- Compelling indications: Diabetes (nephroprotective), CKD with proteinuria, heart failure, post-MI, recurrent stroke prevention
- Side effects: Dry cough (bradykinin), angioedema (contraindication), hyperkalemia, teratogenic (avoid in pregnancy)
3. Angiotensin II Receptor Blockers (ARBs)
| Drug | Brand |
|---|---|
| Losartan | Cozaar |
| Valsartan | Diovan |
| Candesartan | Atacand |
| Irbesartan | Avapro |
| Telmisartan | Micardis |
| Olmesartan | Benicar |
| Azilsartan | Edarbi |
- Mechanism: Block AT1 receptor directly - same benefits as ACEi but do NOT raise bradykinin
- Advantage over ACEi: No dry cough; still avoid in pregnancy (teratogenic)
- Key use: Substitute when ACEi causes cough or angioedema; diabetic nephropathy
4. Calcium Channel Blockers (CCBs)
A. Dihydropyridines (DHP) - Vascular selective
| Drug | Brand |
|---|---|
| Amlodipine | Norvasc |
| Nifedipine | Procardia, Adalat |
| Felodipine | Plendil |
| Nicardipine | Cardene |
- Block L-type Ca²+ channels in vascular smooth muscle → vasodilation → ↓ peripheral resistance
- Advantage: Antihypertensive effect is independent of dietary sodium intake and NSAIDs
- Side effects: Peripheral edema, reflex tachycardia, flushing
B. Non-dihydropyridines (Non-DHP) - Cardiac selective
| Drug | Brand |
|---|---|
| Verapamil | Calan, Isoptin |
| Diltiazem | Cardizem, Dilacor |
- Block Ca²+ channels in myocardium AND vessels → reduce HR and contractility in addition to vasodilation
- Contraindicated in heart failure with reduced EF (HFrEF)
- Use: HTN + angina or atrial arrhythmias
5. Beta-Blockers (β-Blockers)
| Drug | Brand | Selectivity |
|---|---|---|
| Metoprolol | Lopressor, Toprol-XL | β1-selective |
| Atenolol | Tenormin | β1-selective |
| Bisoprolol | (generic) | β1-selective |
| Carvedilol | Coreg | Non-selective + α1 blockade |
| Labetalol | Normodyne | Non-selective + α1 blockade |
| Propranolol | Inderal | Non-selective |
| Acebutolol | (generic) | β1-selective |
| Esmolol | Brevibloc | β1-selective (IV, short-acting) |
- Mechanism: Reduce cardiac output by blocking β1 receptors; also reduce renin release
- Compelling indications: Heart failure (carvedilol, metoprolol), post-MI, angina, tachyarrhythmias
- Side effects: Bradycardia, fatigue, masking of hypoglycemia symptoms, bronchospasm (non-selective agents in asthmatics), erectile dysfunction
- Labetalol/carvedilol (combined α+β blockade) are preferred in HTN emergencies and pheochromocytoma
6. Centrally Acting Agents (α2 Agonists)
| Drug | Notes |
|---|---|
| Clonidine | Oral or transdermal patch; used in resistant HTN; does not reduce renal blood flow |
| Methyldopa | Drug of choice for HTN in pregnancy; multiple daily doses required |
- Mechanism: Stimulate α2 receptors in the CNS → reduce sympathetic outflow → lower BP and HR
- Side effects (clonidine): Sedation, dry mouth (xerostomia), constipation, hypotension
- Important: Abrupt withdrawal of clonidine causes rebound hypertension; taper dose when stopping
7. Direct Vasodilators
| Drug | Notes |
|---|---|
| Hydralazine | Arterial vasodilator; used in resistant HTN and HTN in pregnancy (IV form) |
| Minoxidil | Reserved for severe resistant HTN; causes significant reflex tachycardia and fluid retention |
| Sodium nitroprusside | IV only; used in hypertensive emergencies |
| Nitroglycerine | IV; primarily venous dilation; used in HTN with acute coronary syndromes |
- Side effects of hydralazine: Reflex tachycardia, fluid retention, drug-induced lupus with long-term use
- Both hydralazine and minoxidil typically need co-administration of a beta-blocker (to blunt reflex tachycardia) and a diuretic (to prevent fluid retention)
8. Renin Inhibitor
| Drug | Brand |
|---|---|
| Aliskiren | Tekturna |
- Direct renin inhibitor; rarely used alone; contraindicated with ACEi or ARBs in diabetics or those with CKD (risk of hyperkalemia, acute kidney injury)
Drug Selection by Comorbidity
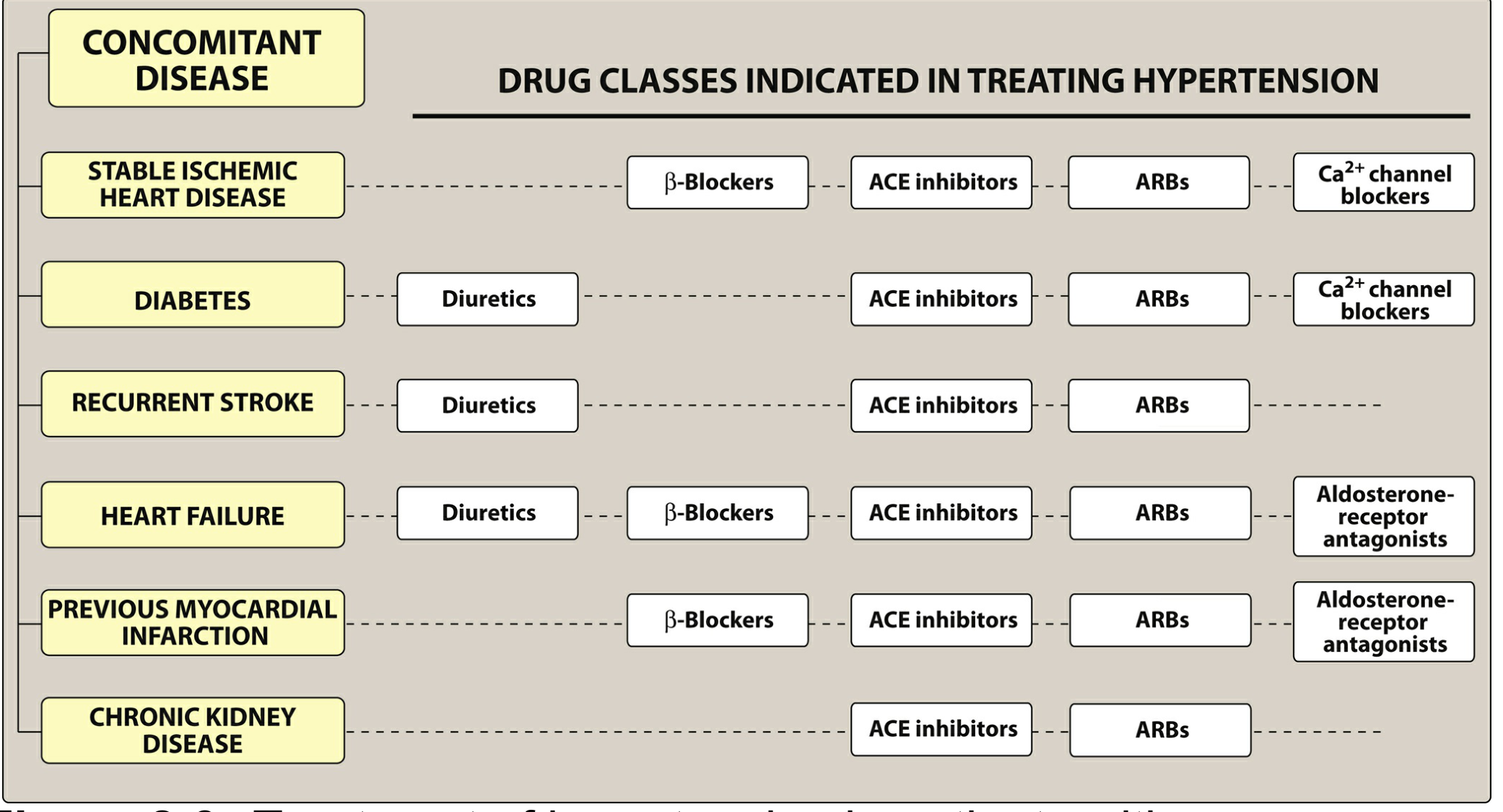
| Comorbidity | Preferred Drug(s) |
|---|---|
| Diabetes | Thiazide, ACEi, ARB, CCB |
| CKD / Proteinuria | ACEi or ARB (first choice) |
| Heart failure (HFrEF) | Diuretic, β-blocker, ACEi/ARB, aldosterone antagonist |
| Post-MI | β-blocker, ACEi/ARB, aldosterone antagonist |
| Stable ischemic heart disease | β-blocker, ACEi/ARB, CCB |
| Recurrent stroke prevention | Diuretic, ACEi/ARB |
| Pregnancy | Methyldopa, labetalol, nifedipine (avoid ACEi/ARBs) |
| Pheochromocytoma | Labetalol or phentolamine (never β-blocker alone) |
| Resistant HTN | Add spironolactone, clonidine, or direct vasodilator |
Recent Evidence: A 2025 Lancet meta-analysis (PMID 40885583) confirmed that drug combinations are significantly more effective than monotherapy. The 2024 ESC Guidelines (PMID 39210715) recommend initiating therapy with a RAAS blocker (ACEi/ARB) + CCB combination in most patients, reserving thiazide diuretics as a third agent.
- Lippincott Illustrated Reviews: Pharmacology, Ch. 8 | Goodman & Gilman's Pharmacological Basis of Therapeutics, Ch. 49
This is a shared conversation. Sign in to Orris to start your own chat.