Ctev management algorithm
Reading File
Finding Sources
Finding Sources
Searching PubMed
"clubfoot" AND "Ponseti" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from Campbell's Operative Orthopaedics 15th Ed 2026 and Miller's Review of Orthopaedics. Let me compile the full management algorithm.
CTEV (Congenital Talipes Equinovarus) - Management Algorithm
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Miller's Review of Orthopaedics 9th Ed
Pathoanatomy - The 4 Deformities (CAVE)
| Component | Description |
|---|---|
| C - Cavus | High arch; forefoot in plantarflexion relative to hindfoot |
| A - Adductus | Forefoot adduction at midfoot |
| V - Varus | Hindfoot inversion |
| E - Equinus | Hindfoot plantarflexion |
The talar neck is deviated medially and plantarward; the navicular and cuboid are displaced medially. Muscles shortened include: intrinsics, Achilles tendon, tibialis posterior, FHL, FDL, joint capsules, and ligaments.
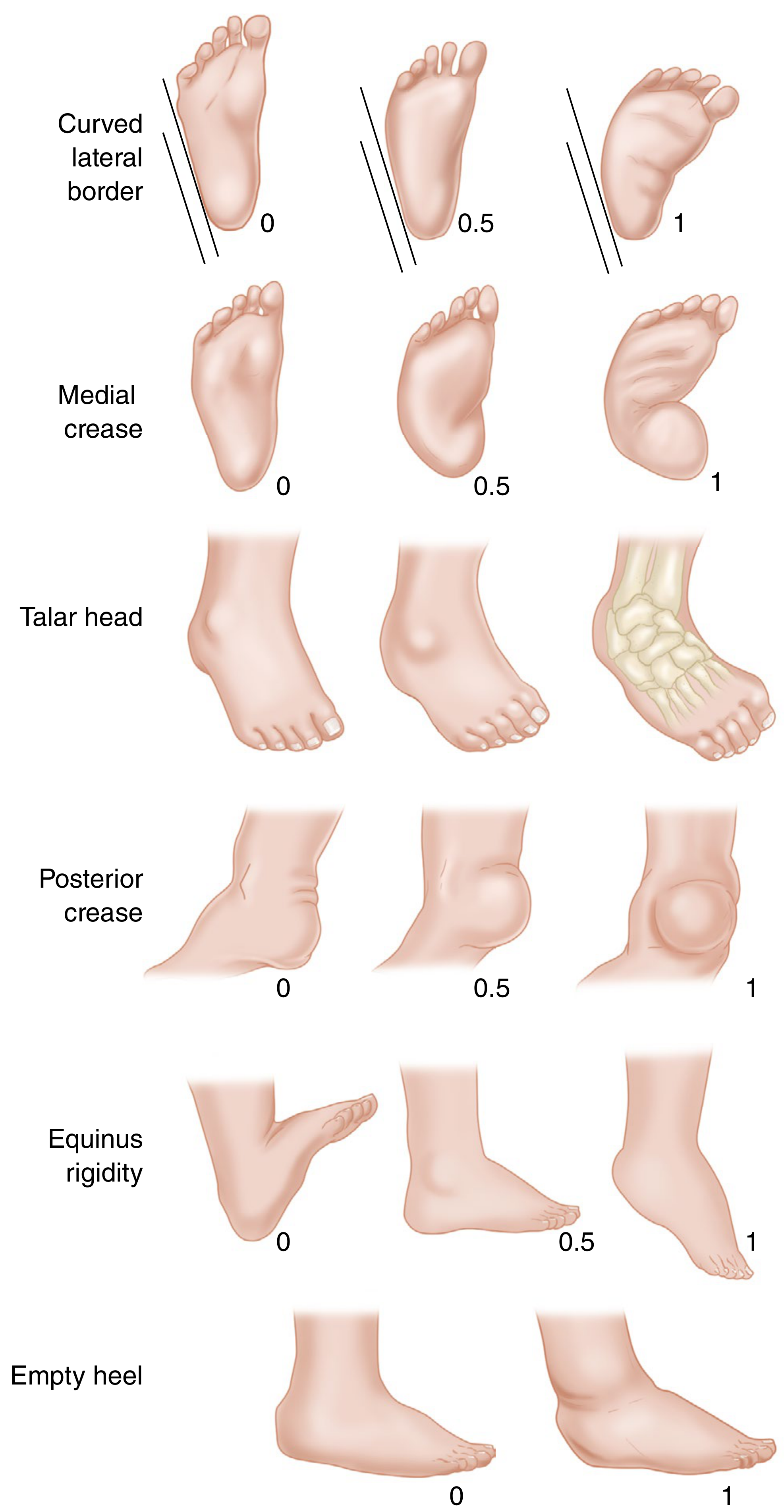
Severity Scoring - Pirani Score
Each of 6 signs scored 0 / 0.5 / 1:
Midfoot signs (0-3):
- Curved lateral border (0 = straight; 0.5 = deviation at metatarsals; 1 = deviation at calcaneocuboid joint)
- Medial crease (0 = fine creases; 0.5 = 2-3 mild; 1 = 1 deep crease)
- Lateral head of talus coverage (0 = mobile; 0.5 = partially; 1 = fixed)
Hindfoot signs (0-3):
4. Posterior crease (0 = fine creases; 0.5 = 2-3 mild; 1 = 1 deep crease)
5. Rigid equinus (0 = dorsiflexion possible; 0.5 = to neutral only; 1 = rigid)
6. Empty heel (0 = calcaneus easily palpable; 0.5 = deep; 1 = not palpable)
Total: 0 (normal) to 6 (severe)
Management Algorithm
Newborn/Infant with CTEV
|
v
ASSESS severity (Pirani score, clinical exam)
Distinguish: Idiopathic vs Syndromic/Neurogenic
|
v
FIRST LINE: PONSETI METHOD (>90% success in idiopathic CTEV)
|
+--> STEP 1: Serial Manipulation + Long-leg Plaster Casting
| - Weekly casts
| - Correct in sequence: C → A → V → E (CAVE order)
| - Cast 1: Correct CAVUS (supinate forefoot, dorsiflex 1st ray)
| - Casts 2-5: Correct ADDUCTUS + VARUS
| (lateral pressure on distal talar head as fulcrum)
| - Average 5-7 casts total
|
+--> STEP 2: Percutaneous Achilles Tenotomy (~90% of patients)
| - To address residual hindfoot EQUINUS
| - Last cast placed in 70° of abduction
| - 3-week post-tenotomy cast
|
+--> STEP 3: Foot Abduction Brace (Denis Browne type)
- Full time: 3 months (23 hrs/day)
- Nights/naps: 3 years total
- 70° abduction, 15° dorsiflexion
- MOST IMPORTANT FACTOR: Brace compliance
Radiographic Assessment
- Minimal ossification in infants; X-rays rarely used routinely
- Parallelism of talus and calcaneus on AP view
- Talocalcaneal (Kite) angle: < 20° (normal 20-40°)
- Talo-1st metatarsal angle: negative (normal 0-20°)
- Dorsiflexion lateral (Turco) view: talocalcaneal angle < 35°
Outcomes and Complications of Ponseti Method
| Complication | Notes |
|---|---|
| Recurrence / undercorrection | 10-30%; most important cause = brace non-compliance |
| Rocker-bottom deformity | Attempting to dorsiflex hindfoot before varus is corrected |
| Flat-top talus | Aggressive dorsiflexion causing talar dome flattening |
| Dynamic supination | 15-20% of treated patients; overpull of tibialis anterior |
Recurrences: Treat with repeat casting first (with or without repeat Achilles tenotomy). Anterior tibial tendon transfer (to lateral cuneiform) for dynamic supination.
Operative Treatment (Only ~5% of Idiopathic Clubfeet)
Reserved for resistant or refractory clubfeet (failed conservative treatment).
Indications by Age
| Age Group | Procedure |
|---|---|
| < 1 year (resistant) | Posteromedial release (PMR) |
| 1-4 years | PMR with/without lateral column lengthening |
| 3-10 years (residual adductus) | Medial opening-wedge OR lateral column-shortening osteotomy OR cuboid decancellation |
| Older children / late presentation | Triple arthrodesis |
| Neglected / adolescent | Modified Ponseti + Ilizarov frame if needed |
Posteromedial Release (PMR)
- Tendon lengthening (Achilles, tibialis posterior, FHL, FDL)
- Subtalar, tibiotalar, and talonavicular capsular release
- Realignment and Kirschner wire fixation
- Key: Posterior tibial artery must be carefully protected (dorsalis pedis is often insufficient)
- Incision: Cincinnati (transverse circumferential) approach
Triple Arthrodesis
- For late-presenting, uncorrected, or severely rigid feet
- Contraindicated in insensate feet (risk of pressure ulceration from rigidity)
Surgical Complications
| Complication | Treatment |
|---|---|
| Dorsal bunion | Capsulotomy + FHL lengthening + transfer FHB to MTP extensor |
| Dynamic supination | Tibialis anterior transfer laterally |
| Recurrent equinus | Anterior distal tibial epiphysiodesis (if growth remaining) |
Special Situations
| Situation | Approach |
|---|---|
| Syndromic clubfoot (arthrogryposis, myelomeningocele) | Higher recurrence; still attempt Ponseti first; often needs more casts and surgery |
| Neurogenic CTEV (stroke, CP) | Tendon rebalancing; split anterior tibial tendon transfer (SPLATT); triple sectioning Achilles |
| Neglected / older child | Modified Ponseti; Ilizarov distraction if stiff |
| Bilateral | Treat simultaneously; severity and response correlated between both feet |
Key Points for Exams
- CAVE = order of deformity components; correction order = C → A → V → E
- Ponseti success rate: >90% in idiopathic CTEV < 2 years
- Achilles tenotomy needed in ~90%; done percutaneously
- Brace worn full-time 3 months, then nights/naps for 3 years
- Brace non-compliance = #1 cause of recurrence
- Surgery only needed in ~5% of idiopathic cases
- Parallelism of talus-calcaneus is the hallmark radiographic finding
- PITX1-TBX4 transcriptional pathway implicated in genetic cases
Recent Evidence (2025-2026): A 2025 systematic review (PMID 41272751) confirmed Ponseti method effectiveness even in neurogenic clubfoot. A 2026 meta-analysis (PMID 41549019) found accelerated Ponseti (casting every 5 days vs. weekly) is similarly effective to standard. A 2026 systematic review (PMID 42210224) found global relapse rates post-Ponseti range 10-37%, with non-bracing being the dominant predictor.
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 1307-1393
- Miller's Review of Orthopaedics 9th Ed, p. 382
This is a shared conversation. Sign in to Orris to start your own chat.