Liver Lobed Septas Relations Clinical aspects Refer- bd chaurasya Diagrams -15 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the material needed for a comprehensive 15-mark answer. Let me compile the full response.
THE LIVER - Anatomy (15 Marks)
Reference: Gray's Anatomy for Students | Color Atlas of Human Anatomy Vol. 2 (BD Chaurasia equivalent level)
1. INTRODUCTION & POSITION
The liver is the largest visceral organ in the body. It is primarily situated in the right hypochondrium and epigastric region, extending into the left hypochondrium. It lies below the right dome of the diaphragm; its inferior border is nearly flush with the right costal margin, running diagonally to the left through the epigastric region.
Fig. 4.102 - Position of the Liver in the Abdomen:
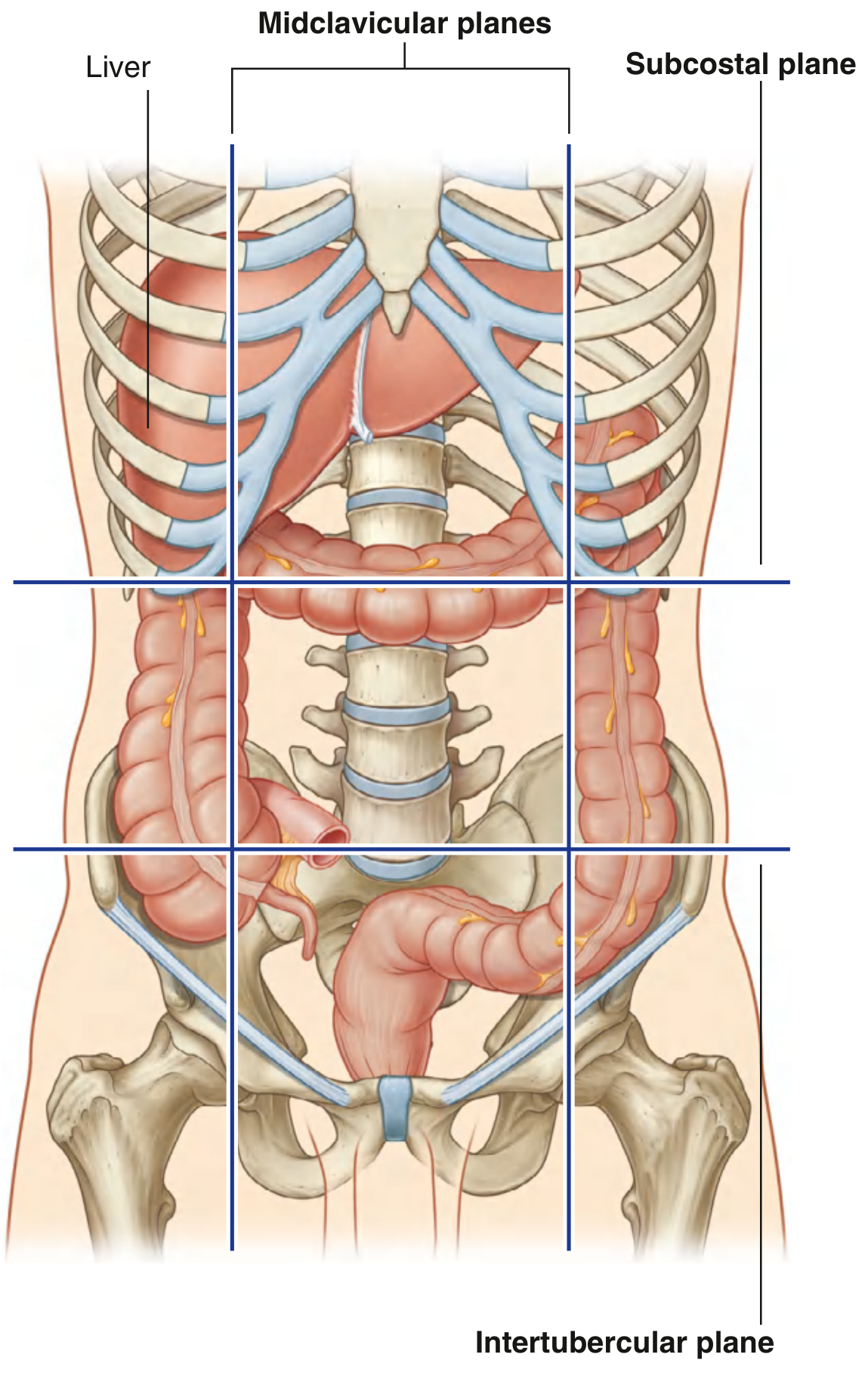
The liver is an intraperitoneal organ. Except for the triangular bare area, it is completely covered by visceral peritoneum, giving it a smooth, glistening appearance.
2. SURFACES
The liver has two main surfaces:
A. Diaphragmatic Surface
- Smooth and domed; lies against the inferior surface of the diaphragm
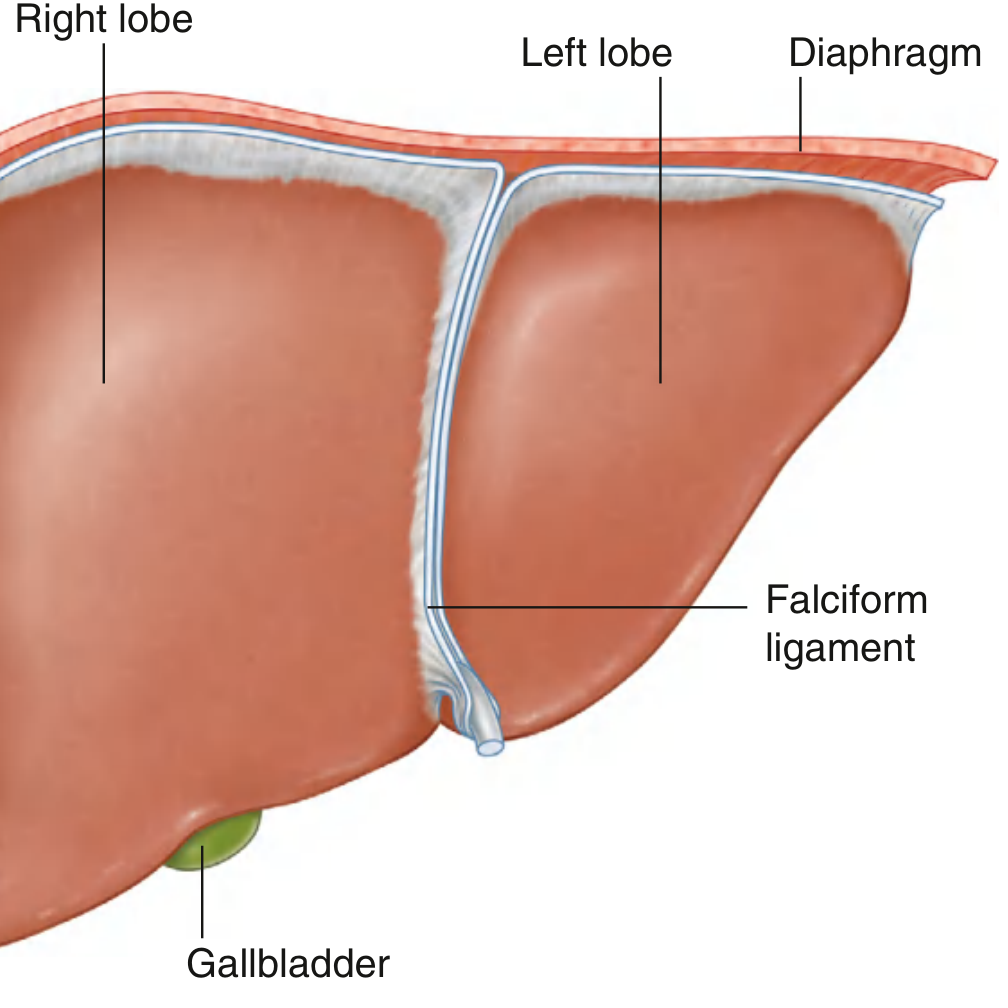
- Subphrenic recess: separates the diaphragmatic surface from the diaphragm, divided by the falciform ligament into right and left portions
- Hepatorenal recess (Morison's pouch): on the right side, between the liver and the right kidney/suprarenal gland - the most dependent peritoneal recess in the supine patient; fluid collects here first
- The anterior surface is divided by the falciform ligament into right lobe and left lobe
B. Visceral Surface
- Slightly concave; covered by visceral peritoneum except at the gallbladder fossa and porta hepatis
- Subdivided by H-shaped grooves (see lobes below)
- The porta hepatis forms the horizontal crossbar of the H and is the gateway to the liver
Fig. 4.105 - Visceral Surface of the Liver (showing all 4 lobes, porta hepatis, ligaments, impressions):
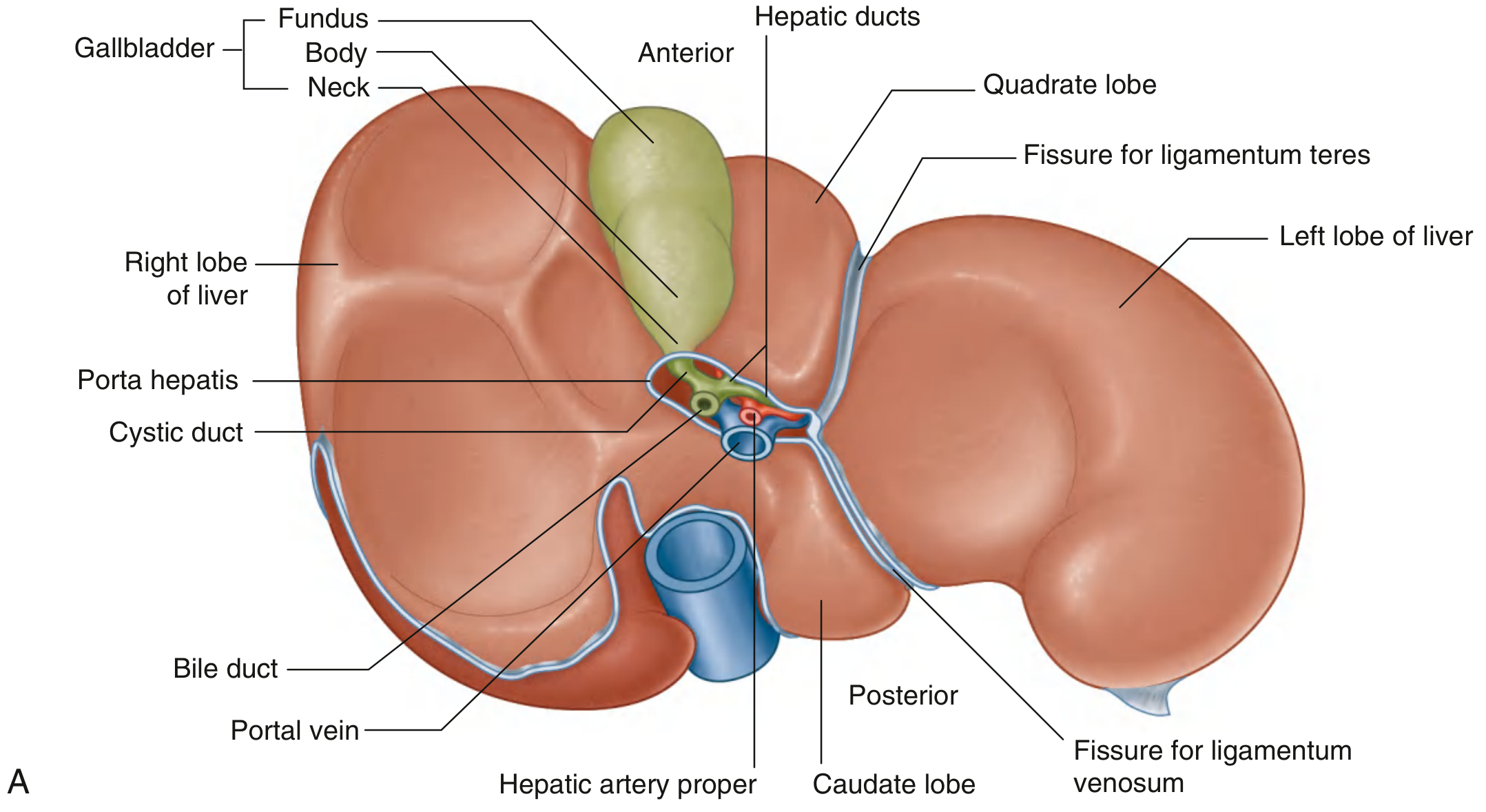
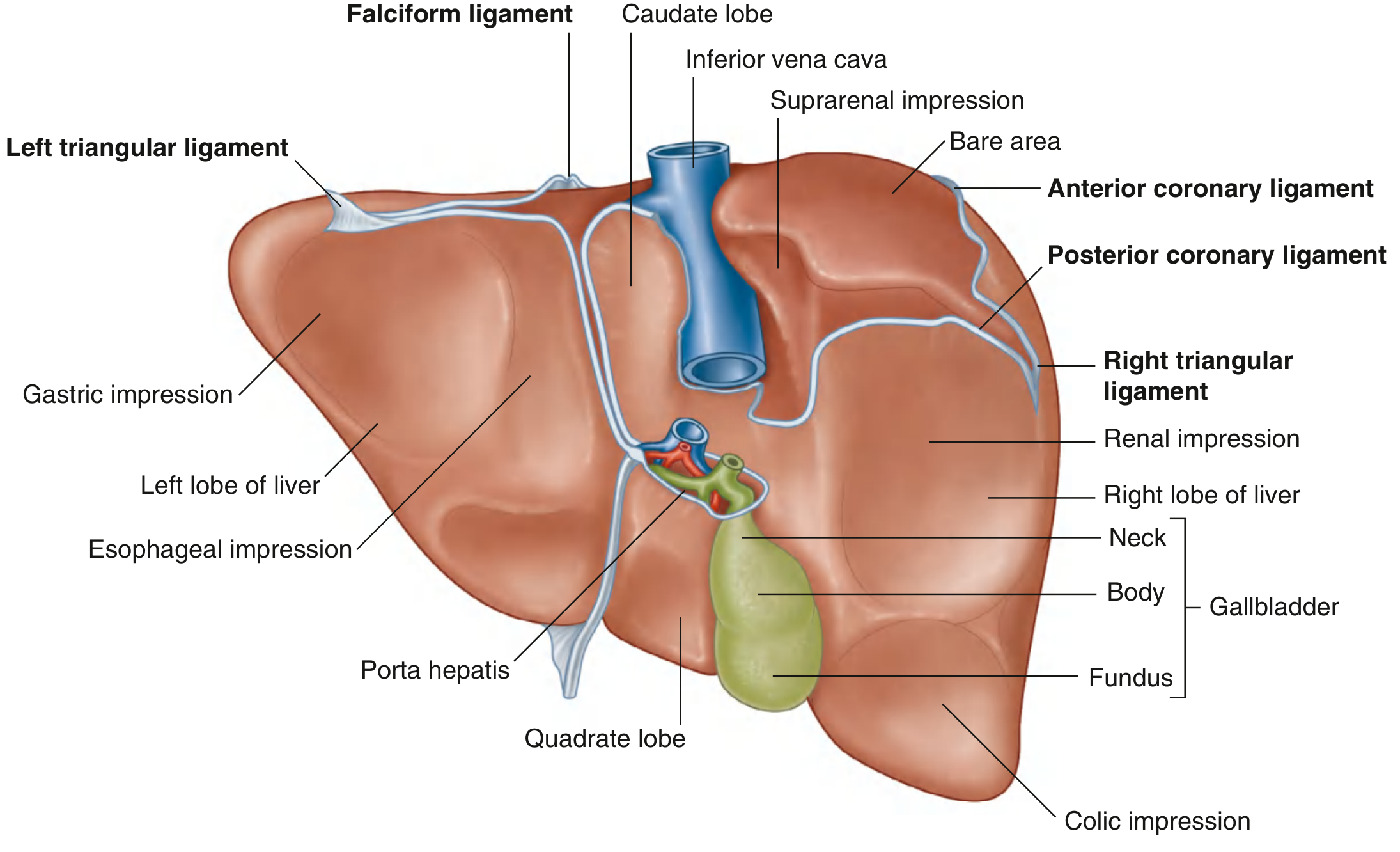
Fig. 4.106 - Posterior View (Bare Area, Ligaments, and Visceral Impressions):
3. LOBES OF THE LIVER
The liver is divided into 4 anatomical lobes. The H-shaped grooves on the visceral surface are the key landmarks:
| Lobe | Boundaries | Functional Relationship |
|---|---|---|
| Right lobe | Largest lobe; to the right of the falciform ligament (anterior) and fissure for ligamentum teres (visceral) | Right hepatic artery and right portal vein |
| Left lobe | Smaller; to the left of the falciform ligament | Left hepatic artery and left portal vein |
| Quadrate lobe | Bounded on the left by the fissure for ligamentum teres and on the right by the gallbladder fossa; anterior part of visceral surface | Functionally related to the left lobe |
| Caudate lobe | Bounded on the left by the fissure for ligamentum venosum and on the right by the groove for the IVC; posterior visceral surface | Functionally separate from both right and left lobes; has independent portal and hepatic venous drainage |
Fissures forming the H-shape:
- Left limb of H: Fissure for the round ligament (ligamentum teres, a remnant of the umbilical vein) anteriorly + Fissure for the ligamentum venosum (remnant of ductus venosus / duct of Arantius) posteriorly
- Right limb of H: Fossa for the gallbladder anteriorly + Groove for the IVC posteriorly
- Horizontal crossbar: Porta hepatis
Diaphragmatic surface - Right and Left Lobes with Falciform Ligament:
4. PORTA HEPATIS
The porta hepatis (gateway of the liver) is the transverse fissure on the visceral surface where:
- Entering: Portal vein (posterior), hepatic artery proper branches (anterior-left), nerves
- Leaving: Right and left hepatic ducts, lymphatic vessels
The bile duct, hepatic artery proper, and portal vein travel in the hepatoduodenal ligament (free margin of the lesser omentum) to reach the porta hepatis.
5. ASSOCIATED LIGAMENTS
| Ligament | Connection | Notes |
|---|---|---|
| Falciform ligament | Liver to anterior abdominal wall | Contains the round ligament of the liver (ligamentum teres); derived from the ventral mesentery |
| Hepatogastric ligament | Liver to lesser curvature of stomach | Part of lesser omentum |
| Hepatoduodenal ligament | Liver to duodenum | Contains portal triad: bile duct (right), hepatic artery (left), portal vein (posterior) |
| Right triangular ligament | Joins coronary ligaments on right | |
| Left triangular ligament | Joins coronary ligaments on left | Terminates in fibrous appendix of liver |
| Anterior coronary ligament | Anterior boundary of bare area | |
| Posterior coronary ligament | Posterior boundary of bare area |
Bare area: Region on the diaphragmatic surface with no intervening peritoneum between liver and diaphragm. Bounded anteriorly by the anterior coronary ligament and posteriorly by the posterior coronary ligament.
6. SEGMENTS (COUINAUD'S SEGMENTAL ANATOMY)
The traditional anatomical lobes differ from functional (surgical) segments. The principal plane (Cantlie's line) divides the liver into right and left halves of approximately equal size - this imaginary line passes from the gallbladder fossa to the IVC and contains the middle hepatic vein.
Couinaud's 8 Segments (numbered clockwise from caudate lobe):
| Segment | Name |
|---|---|
| I | Caudate lobe (posterior) |
| II | Lateral superior area (left lateral) |
| III | Left anterior lateral (lateral inferior area) |
| IV (IVa/IVb) | Medial segment (corresponds to quadrate lobe inferiorly) |
| V | Anterior medial - inferior area |
| VI | Right anterior lateral - posterior inferior area |
| VII | Posterior lateral - posterior superior area |
| VIII | Posterior medial - anterior superior area |
Fig. 4.17 - Couinaud's Segments (anterior and posterior views):
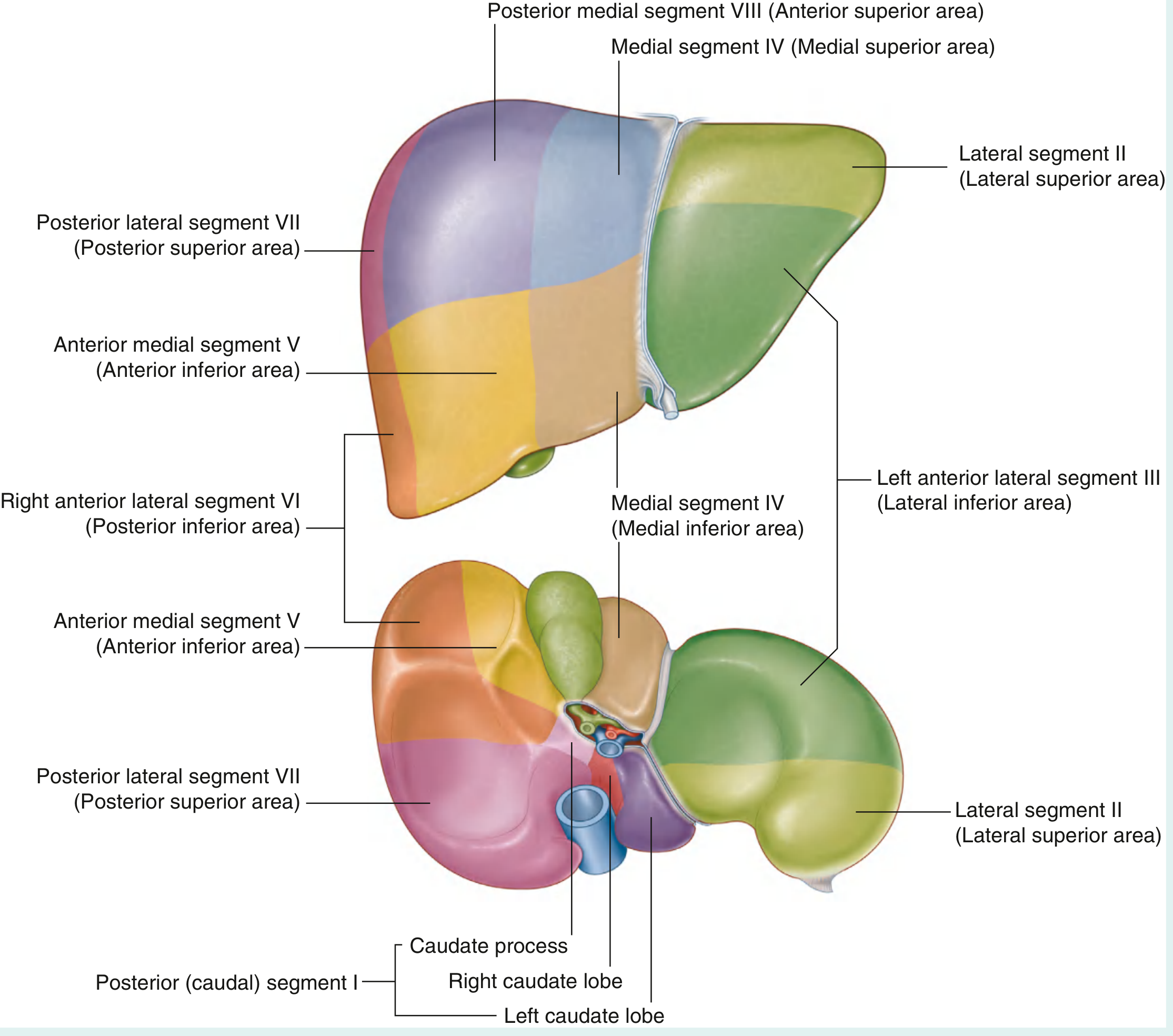
Right hepatectomy = removes segments V, VI, VII, VIII. Left hepatectomy = removes segments II, III, IV.
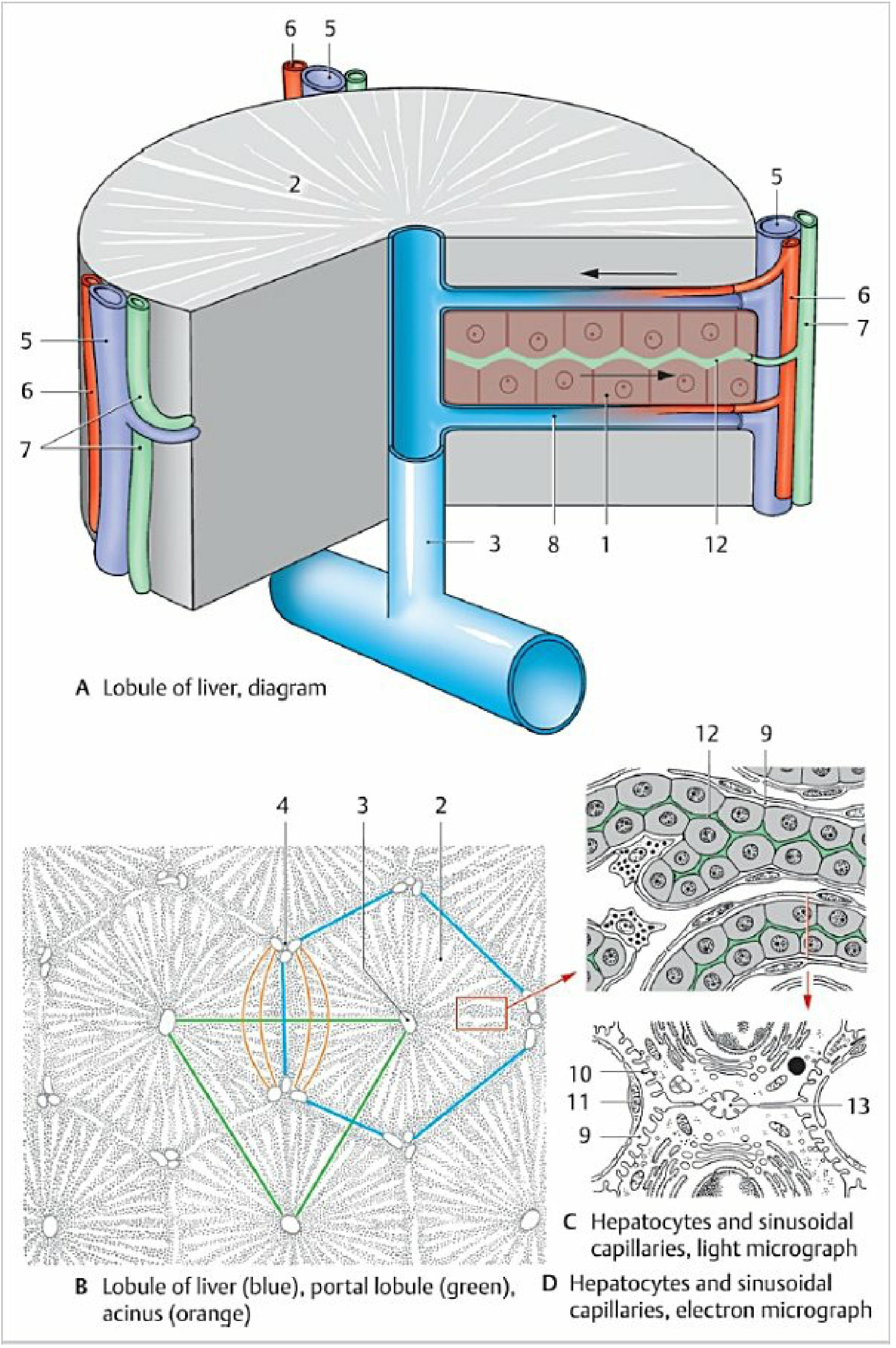
7. MICROSCOPIC ANATOMY / LOBULES (SEPTA)
The liver is enclosed in the visceral peritoneum and the Glisson's capsule (perivascular fibrous capsule), which sends septa into the liver substance forming a supporting connective tissue framework.
Three Lobule Models:
A. Classical (Hepatic) Lobule:
- Functional unit centered on a central vein (terminal hepatic venule)
- Polygonal shape; surrounded by connective tissue septa at the corners = portal areas / portal triads
- Each portal triad contains:
- Interlobular vein (branch of portal vein)
- Interlobular artery (branch of hepatic artery)
- Interlobular bile duct
- All enclosed in the connective tissue of the Glisson capsule
- Hepatocytes radiate from center toward periphery in cell plates separated by sinusoidal capillaries
- Blood flows: Portal triad → sinusoids → central vein → hepatic vein → IVC
- Space of Disse (perisinusoidal space): Between sinusoid wall and hepatocyte surface; contains microvilli, Ito cells (fat-storing), and filtered plasma
- Sinusoidal endothelium is discontinuous (fenestrated, no basement membrane)
- Kupffer cells: Hepatic macrophages on the luminal surface of the sinusoidal endothelium
B. Portal Lobule:
- Places the portal area at the center; emphasizes bile flow direction
- Triangular shape with central veins at the corners
- Bile flows from central vein region → interlobular ducts
C. Hepatic Acinus (of Rappaport):
- Rhombic shape; best correlates with metabolic zonation
- Zone 1 (periportal): closest to blood supply; first affected by toxins, first to regenerate
- Zone 2 (midzonal)
- Zone 3 (centrilobular / perivenular): most susceptible to ischemia and hypoxic damage
Fig. 4.37 - Liver Lobule Diagrams (Classical, Portal, and Acinus models + electron micrograph):
8. RELATIONS
Diaphragmatic Surface Relations:
- Above: Diaphragm (separates it from pleura and base of right lung; on the left, separates it from pericardium/heart)
- Anterior: Anterior abdominal wall
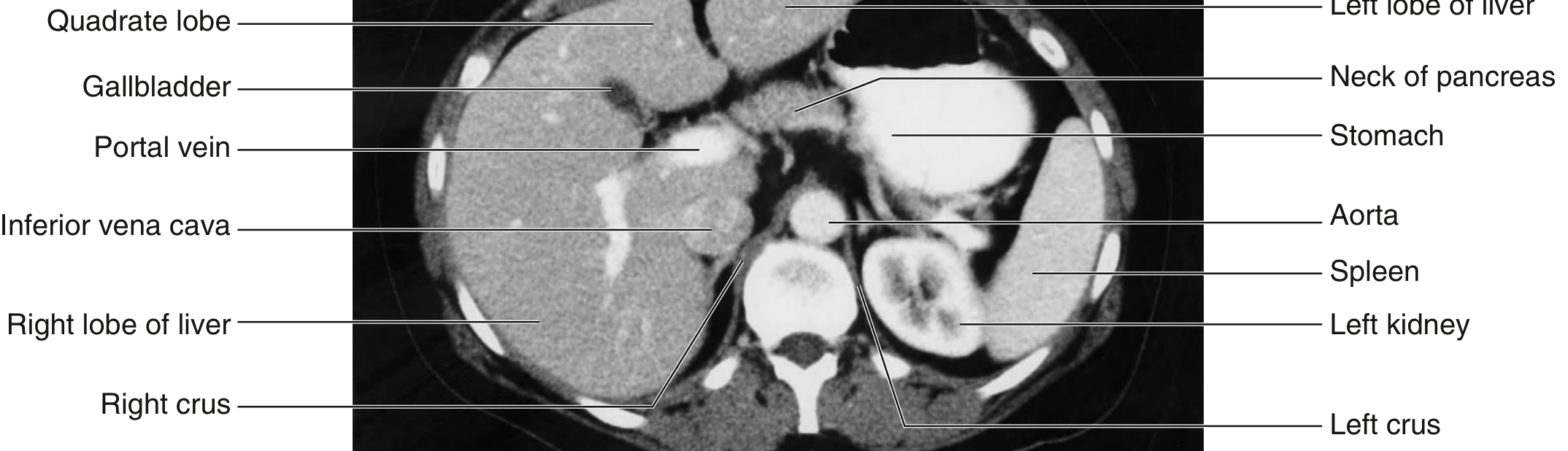
Visceral Surface Relations (impressions):
| Structure | Lobe/Region |
|---|---|
| Esophagus | Left lobe (esophageal impression) |
| Anterior surface of stomach | Left lobe (gastric impression) |
| Superior part of duodenum | Right lobe/quadrate lobe |
| Lesser omentum | Between left lobe and stomach/duodenum |
| Gallbladder | Right and quadrate lobes (gallbladder fossa) |
| Right colic flexure | Right lobe (colic impression) |
| Right transverse colon | Right lobe |
| Right kidney | Right lobe (renal impression) |
| Right suprarenal gland | Right lobe (suprarenal impression) |
| IVC | Groove on posterior diaphragmatic surface |
CT Axial Section - Liver Relations (labeled):
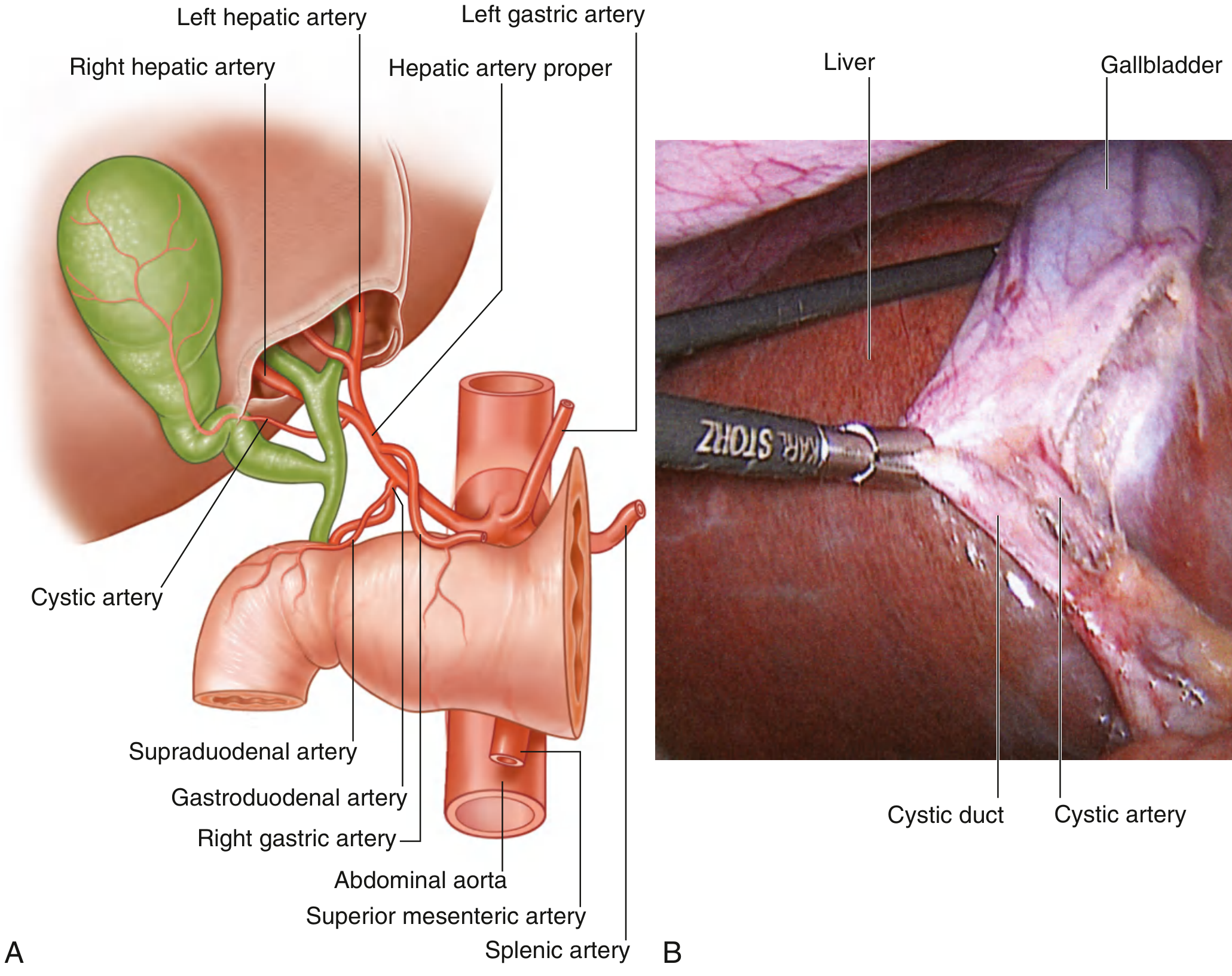
9. BLOOD SUPPLY, VENOUS DRAINAGE & NERVE SUPPLY
Arterial Supply:
- Right hepatic artery and Left hepatic artery - both from the hepatic artery proper (branch of common hepatic artery from the celiac trunk)
- The cystic artery to the gallbladder typically arises from the right hepatic artery
Portal Venous Supply:
- Portal vein (5-8 cm long): formed behind the head of the pancreas by the union of the superior mesenteric vein and splenic vein
- Carries nutrient-rich blood from the GI tract
- Divides into right and left branches at the porta hepatis
- Tributaries of splenic vein: left gastro-omental, short gastric, inferior mesenteric vein
- Tributaries of superior mesenteric vein: jejunal/ileal veins, right gastro-omental, ileocolic, right colic
Fig. 4.107 - Arterial Supply to the Liver and Gallbladder:
Venous Drainage:
- Several short hepatic veins drain into the IVC
- Three main hepatic veins (right, middle, left)
Nerve Supply:
- Hepatic plexus - autonomic nerves; a continuation of the celiac plexus
Lymphatics:
- Drain to hepatic nodes along the porta hepatis → superior diaphragmatic nodes → parasternal nodes
10. CLINICAL ASPECTS
A. Portal Hypertension
When portal vein flow through the liver to the heart is impeded (most commonly by cirrhosis), blood pressure in the portal vein rises - portal hypertension. Portal-caval anastomoses open up at sites where portal and systemic venous systems communicate:
| Site | Portal | Systemic | Clinical result |
|---|---|---|---|
| Lower esophagus | Left gastric vein | Esophageal veins (azygos) | Esophageal varices - most dangerous; 60% mortality per bleed |
| Umbilicus | Paraumbilical veins | Superficial epigastric veins | Caput medusae |
| Lower rectum/anal canal | Superior rectal vein | Middle/inferior rectal veins | Rectal varices |
| Retroperitoneum (Retzius veins) | Colic/intestinal veins | Lumbar/renal veins | Internal varices |
B. Hepatorenal Recess (Morison's Pouch) - Clinical Significance
This is the most dependent part of the peritoneal cavity in the supine patient. In haemoperitoneum or peritonitis, fluid collects here first - critical for FAST (Focused Assessment with Sonography in Trauma) examination.
C. Liver Biopsy
- Percutaneous (standard): Patient lies over the biopsy site; weight of liver compresses the puncture to stem bleeding
- Contraindicated when ascites is present (liver floats away from abdominal wall; bleeding pours freely into ascitic fluid)
- Transjugular liver biopsy: Access through right internal jugular vein → right brachiocephalic vein → SVC → IVC → right hepatic vein; biopsy taken through the hepatic vein wall - bleeding re-enters the circulation directly, avoiding haemoperitoneum risk
D. Liver Resection (Hepatectomy) for Metastases
- Couinaud's segmental anatomy is essential for surgical planning
- The principal plane (through middle hepatic vein, gallbladder fossa to IVC) divides liver into equal right and left halves for resection
- Right hepatectomy: removes segments V, VI, VII, VIII
- Segments V and VI are commonly involved in right lobe metastases
- Left lobe contains only segments II and III anatomically; the lobes do NOT correlate with hepatic volume
E. Subphrenic Abscess
- Pus collects in subphrenic and hepatorenal recesses following peritonitis or abdominal surgery
- Right subphrenic abscess (between liver and diaphragm) is more common given the position of the hepatorenal recess
- Presents with fever, right shoulder pain (referred via phrenic nerve, C3-C5)
F. Bare Area and Retroperitoneal Spread
- The bare area of the liver is in direct contact with the diaphragm
- Infections (e.g., amoebic liver abscess) can spread through the bare area into the right pleural cavity or pericardium
G. Jaundice and Biliary Obstruction
- Obstruction of the bile duct (by gallstones, pancreatic head carcinoma) causes obstructive (post-hepatic) jaundice with pale stools, dark urine, and pruritus
- The bile duct lies in the free margin of the hepatoduodenal ligament: bile duct (right) + hepatic artery (left) + portal vein (posterior)
Sources: Gray's Anatomy for Students, pp. 391-402; Color Atlas of Human Anatomy Vol. 2: Internal Organs, pp. 355-366
This is a shared conversation. Sign in to Orris to start your own chat.