Fatty liver disease
Reading File
Finding Sources
Searching PubMed
"fatty liver disease" AND "MASLD" treatment
Searching the Web
fatty liver disease MASLD NAFLD 2024 2025 guidelines treatment
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information to deliver a detailed, well-sourced answer. Let me compile it.
Fatty Liver Disease (MASLD / NAFLD)
Nomenclature Update
The terminology has shifted. The umbrella term is now steatotic liver disease (SLD), with:
- MASLD (metabolic dysfunction-associated steatotic liver disease) replacing NAFLD
- MASH (metabolic dysfunction-associated steatohepatitis) replacing NASH
This rename reflects ~98% overlap with the old NAFLD/NASH population and more precisely ties the disease to its metabolic drivers. Patients who drink socially (up to 20-50 g/day in women, 30-60 g/day in men) can still be classified as MASLD provided metabolic risk factors are present. - Harrison's Principles of Internal Medicine 22E, p. 2745
Definition & Diagnostic Criteria
MASLD is defined as hepatic steatosis (fat in ≥5% of hepatocytes) in individuals who:
- Drink little to no alcohol, AND
- Have at least one of five cardiometabolic risk factors (central obesity, hypertriglyceridemia, low HDL, hypertension, or prediabetes/T2DM), AND
- Have no secondary cause of hepatic injury (viral hepatitis, Wilson disease, medications, etc.)
Normal liver enzymes do NOT exclude MASLD. The true upper normal for ALT is 29-33 U/L in men and 19-25 U/L in women - lower than most labs report. - Harrison's 22E, p. 2746
Epidemiology
- Global prevalence: ~25% of adults; projected to exceed 30% in the U.S. by 2030
- Highest prevalence in Hispanic and South Asian-Indian populations (~50%), intermediate in whites (~30%), lowest in African Americans (~25%)
- Now a leading indication for liver transplantation in the United States
- MASLD-related HCC is growing fastest among all liver cancer etiologies - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 786; Harrison's 22E, p. 2745
Disease Spectrum & Progression
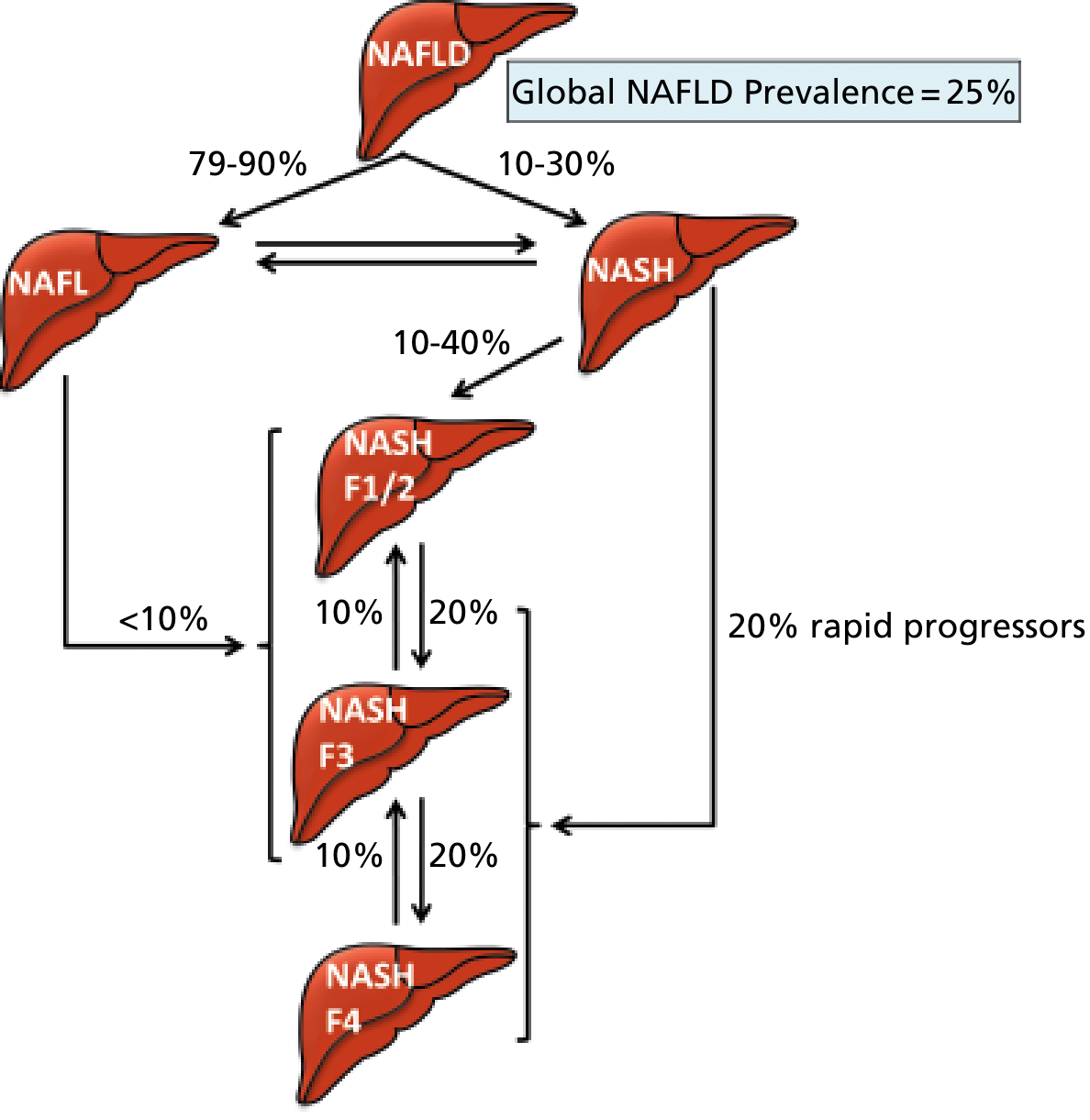
Figure: Global NAFLD prevalence is ~25%. Of these, 79-90% have simple steatosis (NAFL) and 10-30% have NASH. About 20% are "rapid progressors" who can jump directly to advanced fibrosis (F3-F4). Fibrosis stage is the key determinant of clinical outcomes.
The spectrum from benign to severe:
| Stage | Features |
|---|---|
| Isolated steatosis (MASL) | Fat accumulation, no injury - most clinically benign |
| MASH (steatohepatitis) | Steatosis + ballooned hepatocytes + lobular inflammation |
| Fibrosis (F1-F3) | Progressive scarring; F3 = bridging fibrosis |
| Cirrhosis (F4) | End-stage; risk of HCC, hepatic decompensation |
Fibrosis stage - not inflammation - is the single most important predictor of clinical outcomes, morbidity, and mortality. - Yamada's Textbook of Gastroenterology 7e
Pathogenesis
The central driver is insulin resistance acting through several converging mechanisms:
- Free fatty acid (FFA) flux - Insulin resistance causes overactivity of lipoprotein lipase in adipocytes, flooding the liver with FFAs that are stored as triglycerides
- Reduced adiponectin - Dysfunctional adipocytes produce less adiponectin, impairing FFA oxidation in skeletal muscle and increasing hepatocyte FFA uptake
- Lipotoxicity - Accumulated lipids (especially saturated FFAs like palmitate and lysophosphatidylcholine) activate ER stress, mitochondrial dysfunction, and hepatocyte apoptosis
- Innate immune activation - Injured hepatocytes trigger Kupffer cell activation, releasing TNF-α and TGF-β, which activate hepatic stellate cells → collagen deposition → fibrosis
- Inflammasome activation - IL-1 release further amplifies inflammation
- Gut microbiome - Dysbiosis and increased gut-derived endotoxin (LPS) drive hepatic inflammation
- Genetic factors - PNPLA3 rs738409 (C>G) polymorphism significantly increases MASLD severity and HCC risk; first-degree relatives of MASH cirrhosis patients have a 12-fold higher risk of advanced fibrosis
- Robbins, Cotran & Kumar, p. 786-787; Harrison's 22E, p. 2745
Clinical Features
- Most patients are asymptomatic - discovered incidentally via elevated transaminases or hepatic echogenicity on ultrasound
- Some report fatigue, malaise, or right upper quadrant discomfort
- AST:ALT ratio typically < 1 (contrast with alcohol-related disease where ratio > 2)
- Elevated risk of cardiovascular disease (the leading cause of death in MASLD overall)
- In those with MASH/advanced fibrosis, liver-related mortality exceeds cardiovascular mortality
- Complications include decompensated cirrhosis, variceal bleeding, encephalopathy, and HCC - Robbins Basic Pathology 10e, p. 1922
Diagnosis
Non-invasive workup:
- Ultrasound: first-line; sensitive for moderate-severe steatosis but poor for fibrosis staging
- Transient elastography (FibroScan / VCTE): assesses liver stiffness as surrogate for fibrosis; controlled attenuation parameter (CAP) can quantify steatosis simultaneously
- MR elastography (MRE): more accurate than VCTE for fibrosis staging
- Serum scores: NAFLD Fibrosis Score, FIB-4 index, ELF score - used to risk-stratify and identify who needs biopsy
- FLI (Fatty Liver Index): uses BMI, waist circumference, triglycerides, GGT - predicts steatosis
Liver biopsy remains the gold standard to:
- Diagnose MASH definitively (requires steatosis + ballooning + lobular inflammation)
- Stage fibrosis accurately
- Guide treatment decisions
Biopsy is NOT required for all patients - it is reserved for those with intermediate/high non-invasive fibrosis scores or when the diagnosis is uncertain. - Sleisenger & Fordtran's GI and Liver Disease; Harrison's 22E
Differential diagnosis of hepatic steatosis includes: alcoholic liver disease, hepatitis C (genotype 3), medications (amiodarone, methotrexate, tamoxifen, valproate), Wilson's disease, lipodystrophy, parenteral nutrition, inborn errors of metabolism.
Treatment
1. Lifestyle Modification (Cornerstone)
| Weight Loss Goal | Histologic Benefit |
|---|---|
| ≥5% body weight | Improves steatosis, ballooning, inflammation |
| ≥7% body weight | Improves NAFLD Activity Score (NAS) |
| ≥10% body weight | Resolves MASH histologically; fibrosis stabilizes or improves |
- Diet: Moderate caloric restriction (500-750 kcal/day deficit); Mediterranean diet preferred; avoid high-fructose corn syrup and saturated fats; reduce simple carbohydrates
- Exercise: Aerobic + resistance training 3-4x/week (~400 kcal expenditure per session); best results when weight loss is achieved
- Coffee: 2-3 cups/day associated with decreased fibrosis risk
- Sustained weight loss is achievable in only a minority of patients long-term - Sleisenger & Fordtran's, Table 87.3
2. Pharmacotherapy
Currently FDA-approved (as of 2024-2025):
- Resmetirom (Rezdiffra) - selective thyroid hormone receptor-beta (THR-β) agonist; the first FDA-approved drug specifically for MASH with liver fibrosis (F2-F3). A 2024 systematic review and meta-analysis (PMID: 39187533) confirmed its efficacy and safety in MASLD/MASH.
Other agents used in practice (off-label or supported by evidence):
- Pioglitazone (TZD): improves insulin sensitivity; reduces steatosis, inflammation, and ballooning; may reduce fibrosis; used in MASH with T2DM and even in non-diabetics
- Vitamin E (800 IU/day): antioxidant; reduces steatosis and inflammation in non-diabetic adults with biopsy-proven MASH; a 2024 Cochrane review (PMID: 39412049) evaluated the evidence
- GLP-1 receptor agonists (semaglutide, liraglutide): significant weight loss + direct hepatic effects; a 2025 meta-analysis (PMID: 40489581) confirmed GLP-1-based therapies improve MASLD/MASH histologically
- Statins: safe in MASLD/MASH; reduce cardiovascular risk (primary mortality driver); do not significantly improve liver histology
- SGLT2 inhibitors, metformin: improve metabolic parameters but less robust liver-specific evidence
3. Bariatric/Metabolic Surgery
Indicated in eligible patients (BMI ≥35 or ≥30 with metabolic comorbidities). A meta-analysis of 32 studies (3,093 biopsies) showed:
- Steatosis resolution: 66%
- Inflammation resolution: 50%
- Ballooning degeneration resolution: 76%
- Fibrosis resolution: 40%
RYGB (Roux-en-Y gastric bypass) produces greater liver improvement than purely restrictive procedures (sleeve gastrectomy). - Current Surgical Therapy 14e
Complications
| Complication | Notes |
|---|---|
| Cirrhosis | Risk increases with fibrosis stage; F4 is compensated/decompensated cirrhosis |
| HCC | Can arise even in non-cirrhotic MASLD; NAFLD now the fastest-growing cause of HCC in the U.S. |
| Cardiovascular disease | Leading cause of death in MASLD overall; must be actively managed |
| Liver transplant | MASLD is a top indication; recurrence can occur post-transplant if metabolic factors uncontrolled |
Pediatric MASLD
A growing problem due to epidemic childhood obesity. Children show a different histologic pattern compared to adults:
- Inflammation and scarring are more prominent in portal tracts and periportal regions
- Mononuclear infiltrates predominate (vs. neutrophilic in adults)
- Robbins Basic Pathology 10e, p. 1926
Key recent evidence updates (2024-2025):
- Resmetirom received FDA approval for MASH with fibrosis - first drug approved for this indication [PMID 39187533]
- GLP-1 receptor agonists (especially semaglutide) are showing strong histologic benefit in MASH clinical trials [PMID 40489581]
- Cochrane review (2024) on Vitamin E for NAFLD provides updated evidence base [PMID 39412049]
This is a shared conversation. Sign in to Orris to start your own chat.