analyse_media
Reading File
Finding Sources
Finding Sources
Searching PubMed
"lung adenocarcinoma"[MeSH Terms] AND "EBUS-TBNA" AND diagnosis
Reading File
Finding Sources
Searching PubMed
"lung adenocarcinoma"[MeSH Terms] AND "molecular testing" AND treatment
Reading File
Reading File
Searching PubMed
"NSCLC" AND "adenocarcinoma" AND ("EGFR" OR "ALK") AND treatment
Loading Image
Finding Sources
I now have comprehensive information to provide a thorough explanation of this report. Here is a full, clinically structured breakdown:
FNAC Report Explained: Metastatic NSCLC, Adenocarcinoma
What This Report Says
This is a Fine Needle Aspiration Cytology (FNAC) report from AIIMS Bhubaneswar for a 50-year-old woman who presented with cough and hemoptysis for 3 months, with a right hilar mass on imaging.
The sample was obtained via EBUS-TBNA (Endobronchial Ultrasound-guided Transbronchial Needle Aspiration) from station 11R - this means a needle was passed through the bronchial wall under ultrasound guidance to sample the right lower paratracheal/interlobar lymph node (station 11R), which is a standard technique for sampling mediastinal and hilar lymph nodes.
Microscopic Findings - What the Pathologist Saw
The report describes the following cellular features:
| Feature | Significance |
|---|---|
| Highly cellular smears | Abundant malignant cells - confirms active tumor |
| Malignant epithelial cells in tight 3D clusters, papillaroid fragments, acini | Classic pattern of adenocarcinoma - gland-forming tumor |
| Cells round to polygonal with scant-to-moderate basophilic, vacuolated cytoplasm | Vacuoles suggest mucin production - typical of adenocarcinoma |
| Enlarged, moderately pleomorphic nucleus | Irregular nuclear size - hallmark of malignancy |
| Coarse chromatin and prominent nucleoli | Aggressive nuclear features |
| Few multinucleated giant cells | Seen in aggressive/reactive tumors |
| Hemorrhagic background | Common in EBUS-TBNA samples and in vascular tumors |
Diagnosis (Impression)
Metastatic non-small cell lung carcinoma (NSCLC), morphologically adenocarcinoma
This means:
- The primary tumor is in the lung (most likely), and has spread to the hilar lymph node (station 11R)
- It is classified as NSCLC (as opposed to small cell lung cancer)
- The subtype is adenocarcinoma - the most common subtype of lung cancer, especially in women and non-smokers
Cancer Category: POS (Positive) - Diagnostic for malignancy.
Why "Metastatic"?
Station 11R is the interlobar lymph node on the right side. When a lung tumor spreads to hilar lymph nodes, it is classified as at least Stage IIIA (if only regional nodes) or Stage IV (if distant metastasis). The right hilar mass plus positive lymph node sampling indicates regional nodal spread at minimum.
What Happens Next - Mandatory Steps
According to current guidelines (Murray & Nadel's Textbook of Respiratory Medicine; Harrison's Principles of Internal Medicine 22E), all patients with metastatic adenocarcinoma must undergo:
1. Molecular/Biomarker Testing (MANDATORY)
"It is imperative that metastatic adenocarcinoma, large cell carcinoma, and NSCLC not otherwise specified undergo molecular testing, preferably with next-generation sequencing." - Murray & Nadel's Textbook of Respiratory Medicine
The following must be tested:
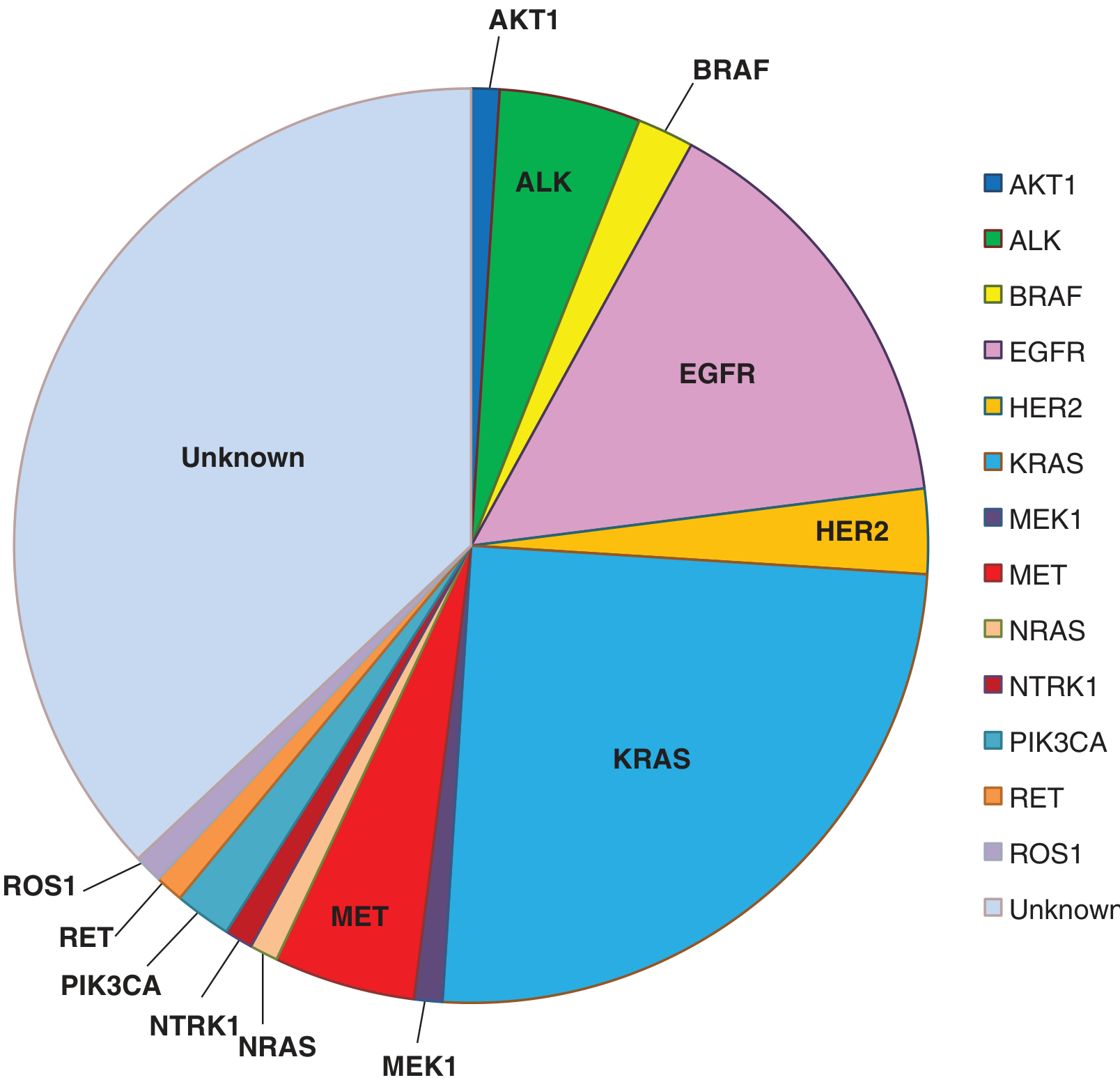
| Gene/Target | Frequency in Adenocarcinoma | Targeted Drug Available |
|---|---|---|
| EGFR mutation | 10-35% | Osimertinib, Erlotinib, Gefitinib, Afatinib |
| ALK fusion | ~8% | Alectinib, Crizotinib, Lorlatinib |
| ROS1 rearrangement | ~2% | Entrectinib, Crizotinib |
| KRAS G12C | ~25% (most common) | Sotorasib, Adagrasib |
| BRAF V600E | ~2% | Dabrafenib + Trametinib |
| HER2 (ERBB2) | ~2-3% | Trastuzumab deruxtecan |
| MET amplification | ~1-5% | Tepotinib, Capmatinib |
| RET fusion | ~1-2% | Selpercatinib, Pralsetinib |
| NTRK fusion | rare | Larotrectinib, Entrectinib |
The chart below shows the distribution of driver mutations in lung adenocarcinoma:
2. PD-L1 Expression Testing
- Required to determine eligibility for immunotherapy (pembrolizumab, atezolizumab, nivolumab)
- If PD-L1 ≥ 50% and no targetable driver, pembrolizumab monotherapy is first-line
3. Full Staging Workup
- CT chest/abdomen/pelvis with contrast
- PET-CT scan (whole body) to detect distant metastases
- Brain MRI (adenocarcinoma has high propensity for brain metastases)
- Bone scan or PET if bone pain
4. IHC (Immunohistochemistry) on the Cell Block
The report notes IHC as "NA" currently. IHC with TTF-1, Napsin-A (positive in lung adenocarcinoma) and p40/CK5/6 (negative, to exclude squamous cell carcinoma) should be performed on the cell block. This also helps confirm the primary origin.
Treatment Overview (Stage Dependent)
| Stage | Treatment Approach |
|---|---|
| If actionable mutation found (EGFR, ALK, etc.) | Targeted oral therapy - best outcomes |
| If PD-L1 high, no driver mutation | Immunotherapy (pembrolizumab) |
| If no driver, PD-L1 intermediate/low | Platinum-based chemotherapy + immunotherapy |
| Stage III unresectable | Concurrent chemoradiotherapy + Durvalumab consolidation |
| Stage IV with driver mutation | Targeted TKI therapy |
With EGFR-targeted therapy (TKIs), the 5-year survival in metastatic adenocarcinoma improved from ~4% (pre-TKI era) to 14.6% - a significant improvement. - Murray & Nadel's Textbook of Respiratory Medicine
Key Summary for the Patient/Family
- A cancer diagnosis has been confirmed in the right hilar lymph node
- The cancer is lung adenocarcinoma (a type of non-small cell lung cancer)
- This is NOT a final/complete workup - the report itself says "correlation with clinical, radiological and other investigations is mandatory"
- Molecular testing is the most important next step - it can identify treatable gene mutations and open the door to targeted oral therapies with much better outcomes
- This should be managed by a multidisciplinary team including a pulmonologist, medical oncologist, radiation oncologist, and thoracic surgeon
- The case should be discussed in a tumor board before treatment decisions are made
Important: This explanation is for educational/informational purposes. All clinical decisions must be made by the treating oncology team based on the full clinical picture, complete staging, and molecular test results.
This is a shared conversation. Sign in to Orris to start your own chat.