Jaundice
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the content needed for a thorough response. Let me compile a comprehensive answer.
Jaundice
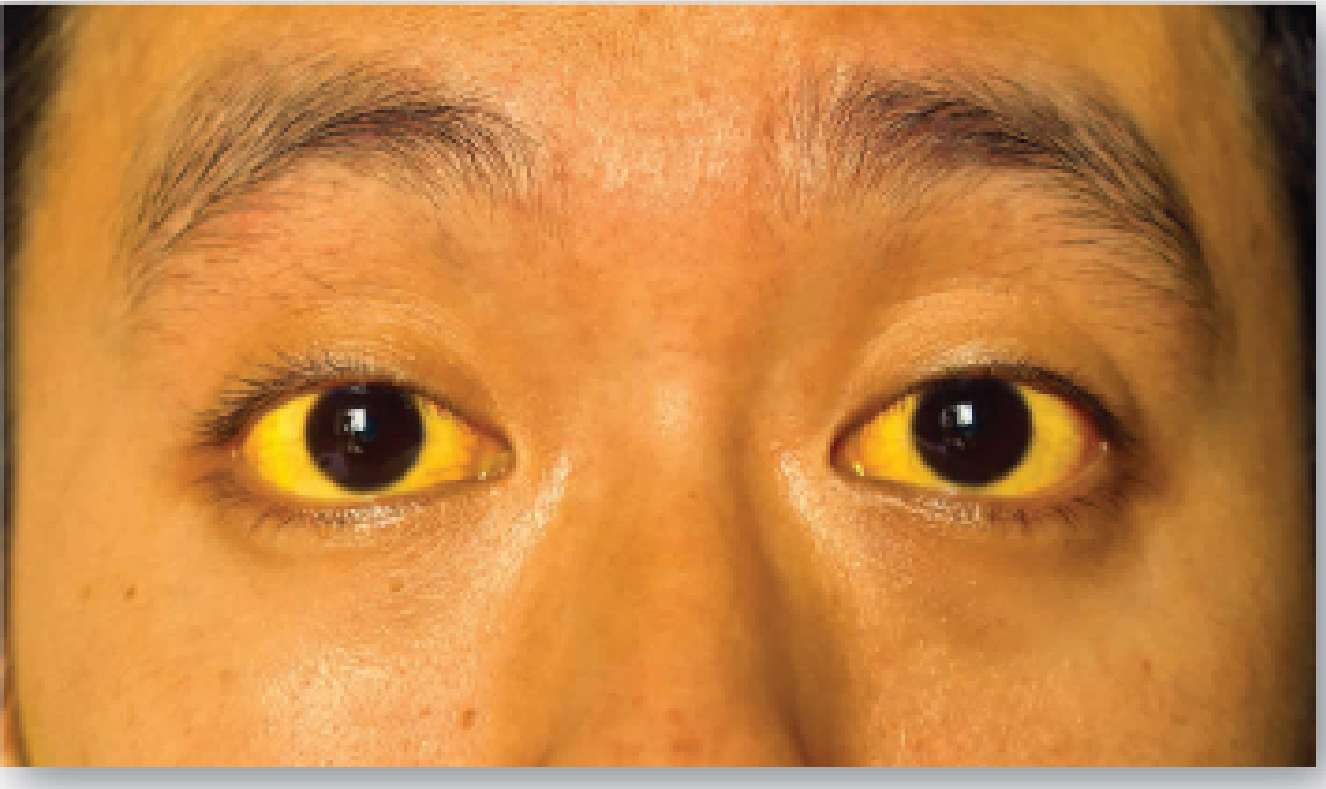
Jaundice (icterus) is the yellowish discoloration of the skin, sclera, and mucous membranes caused by excess bilirubin in the blood. It becomes clinically detectable when serum bilirubin rises above 2.5-3 mg/dL.
Bilirubin Metabolism - The Foundation
Normal bilirubin metabolism proceeds in three phases:
1. Bilirubin Formation (Prehepatic)
- ~80% of bilirubin comes from RBC breakdown; the rest from myoglobin and cytochromes
- Heme is catabolized by heme oxygenase in macrophages (MPS) → biliverdin (green) → bilirubin (red-orange)
- This unconjugated bilirubin (UCB) is water-insoluble, so it binds albumin for transport to the liver
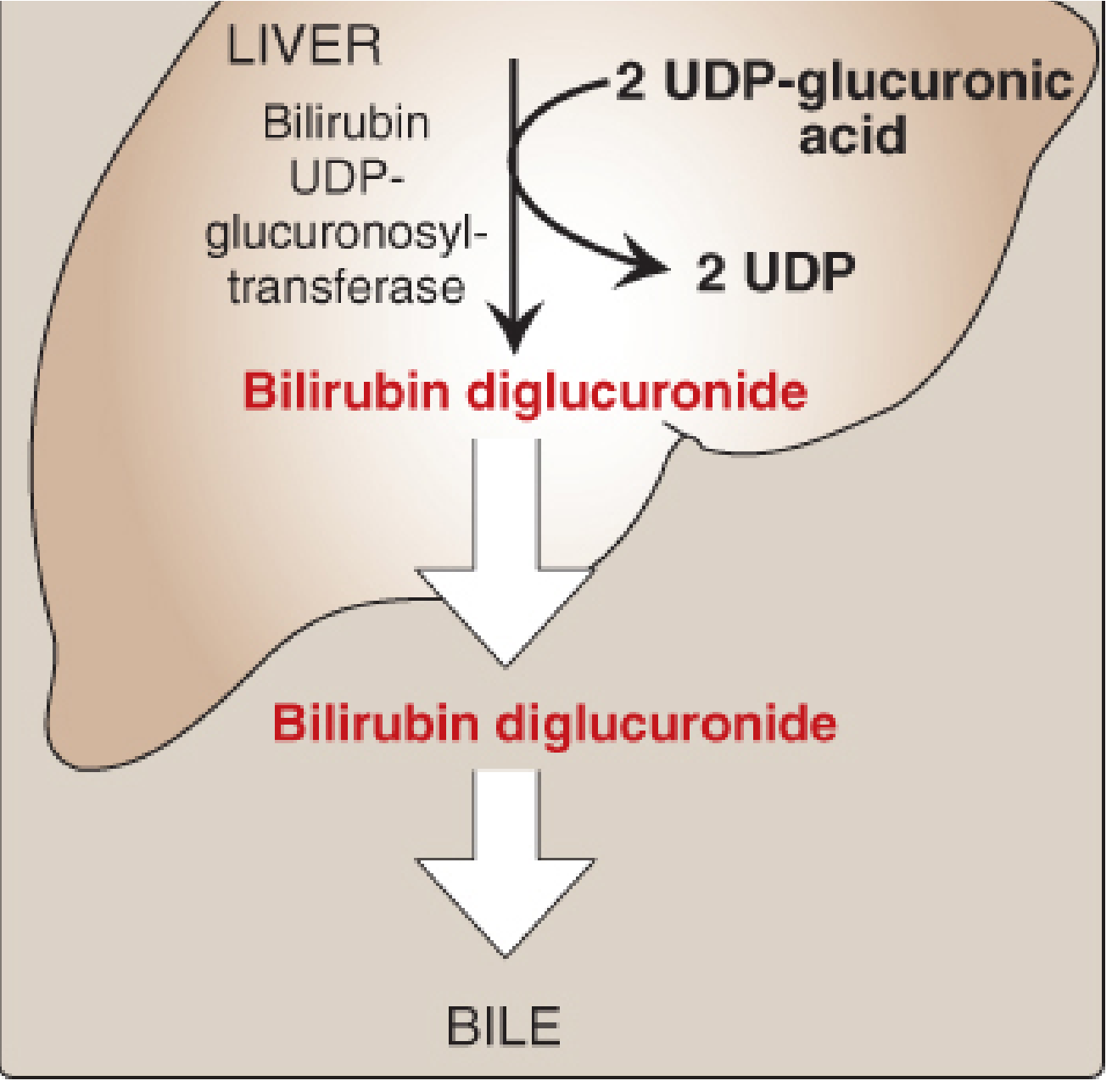
2. Hepatic Conjugation (Intrahepatic)
- UCB enters hepatocytes via facilitated diffusion, binds ligandin
- The enzyme bilirubin UDP-glucuronosyltransferase (bilirubin UGT) conjugates bilirubin with 2 glucuronic acid molecules → bilirubin diglucuronide (conjugated bilirubin, CB)
- CB is water-soluble and actively transported into bile canaliculi
3. Excretion (Posthepatic)
- CB is secreted into bile → intestine → converted to urobilinogen by gut bacteria
- Most urobilinogen is excreted in stool as stercobilin (gives stool its brown color)
- A small fraction is reabsorbed (enterohepatic circulation), reaches the kidney, and is excreted as urobilin (gives urine its pale yellow color)
Classification of Jaundice
Jaundice is classified by the site of bilirubin metabolism dysfunction:
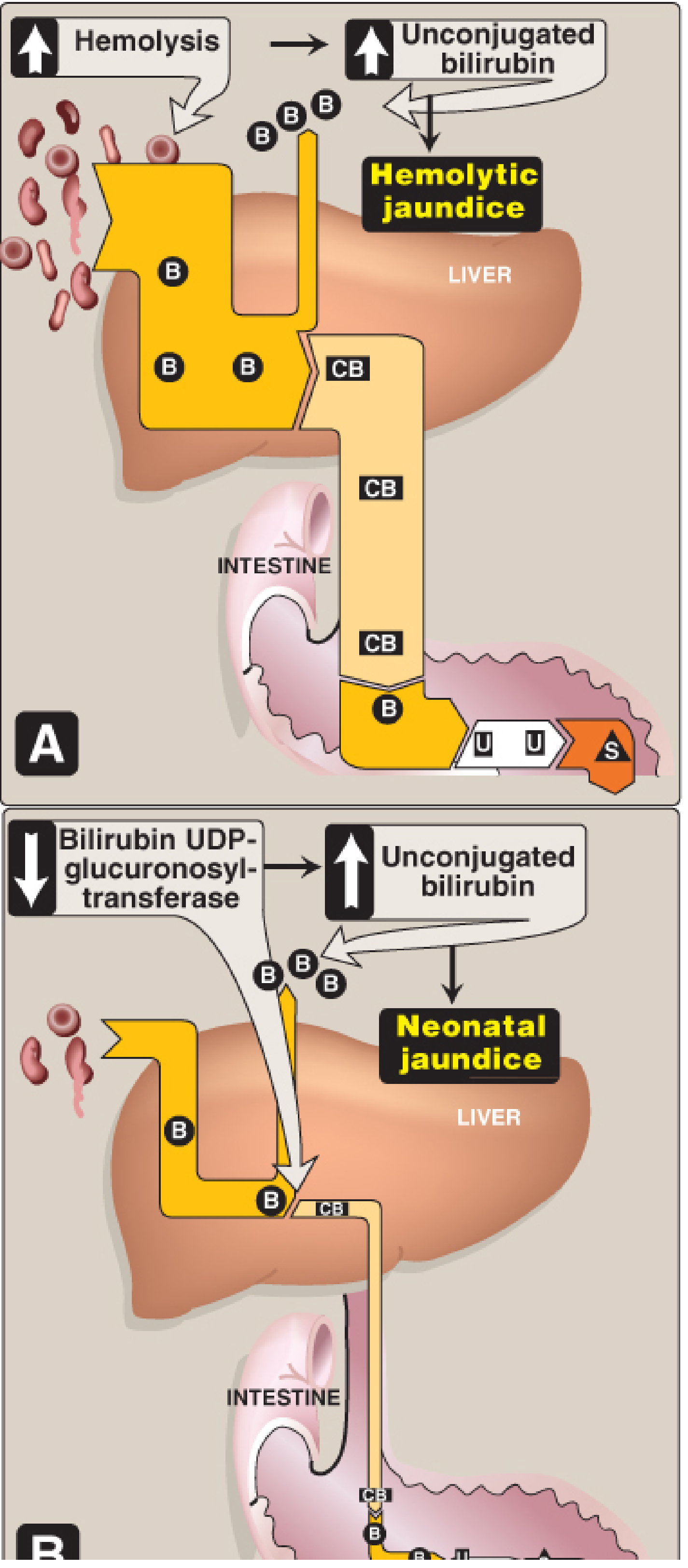
1. Prehepatic (Hemolytic) Jaundice
- Cause: Excessive RBC destruction overwhelms the liver's conjugation capacity
- Bilirubin type: Unconjugated hyperbilirubinemia (UCB elevated)
- Mechanism: Hemolysis produces bilirubin faster than it can be conjugated
- Examples: Sickle cell anemia, G6PD deficiency, pyruvate kinase deficiency, immune hemolysis (Coombs+), microangiopathic hemolytic anemia, mechanical hemolysis (prosthetic heart valves)
- Urine findings: Urobilinogen increased; NO bilirubin in urine (UCB is not filtered by kidneys)
- Stool: Normal color (stercobilin normal or increased)
2. Hepatocellular (Intrahepatic) Jaundice
- Cause: Liver cell damage impairs both conjugation and excretion
- Bilirubin type: Mixed (both UCB and CB elevated)
- Examples: Viral hepatitis, cirrhosis, alcoholic liver disease, ischemic hepatitis, drug toxicity
- Inherited enzyme disorders:
- Gilbert's syndrome - diminished bilirubin UGT activity; affects 4-7% of the population; benign, causes mild transient UCB elevation during fasting/stress/illness
- Crigler-Najjar syndrome (I & II) - more severe deficiency of bilirubin UGT; neonates at risk of kernicterus
- Dubin-Johnson syndrome - defect in CB transport out of hepatocyte; CB accumulates in blood
- Rotor's syndrome - similar to Dubin-Johnson, disrupts CB secretion
- Urine: Dark (urobilinogen increased - less reabsorbed by damaged liver, more reaches urine; plus urinary bilirubin present)
- Stool: Pale/clay-colored (less stercobilin)
3. Posthepatic (Obstructive/Cholestatic) Jaundice
- Cause: Blockage of the common bile duct preventing CB from reaching the intestine
- Bilirubin type: Conjugated hyperbilirubinemia (CB elevated)
- Examples:
- Intraluminal: choledocholithiasis (gallstones), biliary sludge
- Mural: cholangiocarcinoma, biliary strictures (post-operative, PSC)
- Extramural: pancreatic head cancer, periampullary tumors, lymph node compression
- Urine: Dark (CB filtered by kidneys - "bilirubinuria"); urinary urobilinogen ABSENT
- Stool: Pale, clay-colored (no bile reaching intestine)
- Symptoms: Pruritus (bile salt deposition in skin), right upper quadrant pain, nausea
Comparison Table
| Feature | Prehepatic | Hepatocellular | Posthepatic |
|---|---|---|---|
| Bilirubin type | UCB ↑ | Mixed (UCB + CB) | CB ↑ |
| Urine color | Normal | Dark | Dark ("Coca-Cola") |
| Urine bilirubin | Absent | Present | Present |
| Urine urobilinogen | Increased | Increased | Absent |
| Stool color | Normal/dark | Pale | Pale/clay |
| ALP | Normal | Mildly ↑ | Markedly ↑ |
| ALT/AST | Normal | Markedly ↑ | Mildly ↑ |
| van den Bergh reaction | Indirect +ve | Both +ve | Direct +ve |
Special Topic: Neonatal Jaundice
- Occurs in ~60% of full-term and ~80% of preterm neonates in the first postnatal week
- Cause: Low bilirubin UGT activity at birth (reaches adult levels at ~4 weeks) → physiologic UCB accumulation
- Danger: UCB >20-25 mg/dL can cross the blood-brain barrier → deposits in basal ganglia → kernicterus (bilirubin encephalopathy)
- Treatment: Phototherapy with blue fluorescent light converts bilirubin to water-soluble photoisomers that can be excreted without conjugation
- Pathologic causes include: ABO/Rh incompatibility, G6PD deficiency, biliary atresia, Crigler-Najjar
Lab Investigations
| Test | Purpose |
|---|---|
| Total bilirubin | Overall bilirubin burden |
| Direct (conjugated) bilirubin | Distinguishes obstructive/hepatocellular from hemolytic |
| Indirect (unconjugated) bilirubin | Calculated: total - direct |
| ALT, AST | Hepatocellular injury markers |
| ALP, GGT | Cholestatic pattern |
| Urine bilirubin + urobilinogen | Bedside type differentiation |
| Full blood count + reticulocytes | Hemolytic workup |
| Coombs test | Immune-mediated hemolysis |
| Abdominal ultrasound | First-line imaging - dilated bile ducts? stones? |
| MRCP | Non-invasive biliary tree visualization |
| ERCP | Diagnostic + therapeutic (stone removal, stent placement) |
Note on van den Bergh reaction: UCB reacts slowly (indirect), CB reacts rapidly in aqueous solution (direct). In normal plasma, only ~4% of total bilirubin is conjugated (direct-reacting).
Key Causes by Clinical Context
| Presentation | Likely Diagnosis |
|---|---|
| Young patient, family history, episodic | Gilbert's/Crigler-Najjar |
| Acute illness + very high ALT | Viral/ischemic hepatitis |
| Painless jaundice + weight loss | Pancreatic head carcinoma ("Courvoisier's sign") |
| Colicky RUQ pain + fever + jaundice | Choledocholithiasis (Charcot's triad) |
| Jaundice + fever + hypotension + confusion | Acute cholangitis (Reynolds' pentad) |
| Jaundice in a neonate | Physiologic; rule out biliary atresia, hemolytic disease |
Sources:
- Lippincott Illustrated Reviews: Biochemistry, 8th ed, Chapter 21 (Bilirubin metabolism & jaundice classification)
- Schwartz's Principles of Surgery, 11th ed (Prehepatic/intrahepatic/posthepatic classification, workup)
- Sleisenger and Fordtran's GI and Liver Disease (Pruritus management, palliative context)
This is a shared conversation. Sign in to Orris to start your own chat.