Acute pancreatitis
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND management
Reading File
Reading File
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND treatment
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile a complete, well-structured answer.
Acute Pancreatitis
A sudden inflammatory disease of the pancreas, acute pancreatitis (AP) ranges from a mild, self-limiting illness to a life-threatening emergency with multi-organ failure and mortality approaching 30% in severe cases.
Definition and Diagnosis
The diagnosis requires at least 2 of the following 3 criteria (Revised Atlanta Classification):
- Abdominal pain characteristic of acute pancreatitis
- Serum amylase and/or lipase ≥3x the upper limit of normal
- Characteristic findings on imaging (CT, MRI, or ultrasound)
- Grainger & Allison's Diagnostic Radiology, p. 677
- Textbook of Family Medicine 9e, p. 1136
Etiology
| Cause | Approximate Frequency |
|---|---|
| Gallstones / biliary sludge / microlithiasis | >50% of cases |
| Alcohol | ~30% |
| Hypertriglyceridemia (TG >1000 mg/dL) | <5% |
| Trauma (often blunt abdominal) | <5% |
| Post-ERCP | ~3-5% |
| Medications | <5% (valproate, L-asparaginase, 6-MP, corticosteroids, thiazides) |
| Infections (mumps, CMV, Coxsackievirus, EBV) | Rare |
| Metabolic (hypercalcemia) | Rare |
| Anatomic (pancreas divisum) | Rare |
| Idiopathic (no identifiable cause) | ~5% |
| Pancreatic neoplasm | Consider in any patient >40 years |
Gallstones and alcohol together account for ~80% of all cases. When triglycerides are >1000 mg/dL with no evidence of gallstones or alcohol use, hypertriglyceridemia should be considered the etiology.
- Textbook of Family Medicine 9e, p. 1136-1137
Pathophysiology
The central mechanism involves premature activation of pancreatic enzymes (particularly trypsinogen → trypsin) within acinar cells. This triggers a cascade of autodigestion:
- In interstitial oedematous pancreatitis (70-80% of cases): proteolytic enzymes injure acinar cells causing edema and swelling, but the inflammatory response is not strong enough to cause necrosis. The gland remains perfused.
- In necrotising pancreatitis: inflammation is sufficient to cause cell apoptosis and fat necrosis, which spreads to the parenchyma. Necrosis is the major determinant of morbidity and mortality.
Systemic effects arise from massive cytokine release (TNF-α, IL-1, IL-6), leading to SIRS, capillary leak, third-spacing of fluids, hypovolemia, and ultimately multi-organ failure (respiratory, renal, cardiovascular).
- Grainger & Allison's Diagnostic Radiology, p. 681
Clinical Features
Symptoms:
- Sudden-onset, severe, constant epigastric pain - classically described as "boring through to the back" or left scapular region
- Nausea, vomiting, anorexia, fever
- Patients are more comfortable sitting forward/leaning
Signs:
- Tachycardia, tachypnea (reflecting SIRS)
- Epigastric tenderness, guarding; hypoactive bowel sounds
- Cool, cyanotic extremities (underperfusion)
- Grey-Turner sign: flank ecchymosis (retroperitoneal hemorrhage)
- Cullen sign: periumbilical ecchymosis
- (Both signs indicate hemorrhagic necrosis and predict severe disease)
Lab findings:
-
WBC 12,000-20,000/mm³
-
Elevated serum amylase (rises within hours, clears faster) and lipase (more specific, persists longer)
-
Serum lipase is superior to amylase alone - relying on amylase alone is error-prone
-
Elevated bilirubin, transaminases, ALP suggest a biliary cause
-
Hemoconcentration (high hematocrit), elevated BUN/creatinine from third-spacing
-
Hypocalcemia, hyperglycemia in severe disease
-
Elevated CRP is a useful marker of pancreatic necrosis
-
Sleisenger & Fordtran's GI and Liver Disease, p. 174
-
Textbook of Family Medicine 9e, p. 1137
Imaging
Ultrasound
First-line for identifying gallstones as a cause. Sensitivity for pancreatitis itself is 62-95% (poor due to bowel gas obscuring the pancreas in up to 30% of cases). When the pancreas is visible, findings include diffuse enlargement, reduced reflectivity, and peripancreatic fluid.
Ultrasound in oedematous pancreatitis:
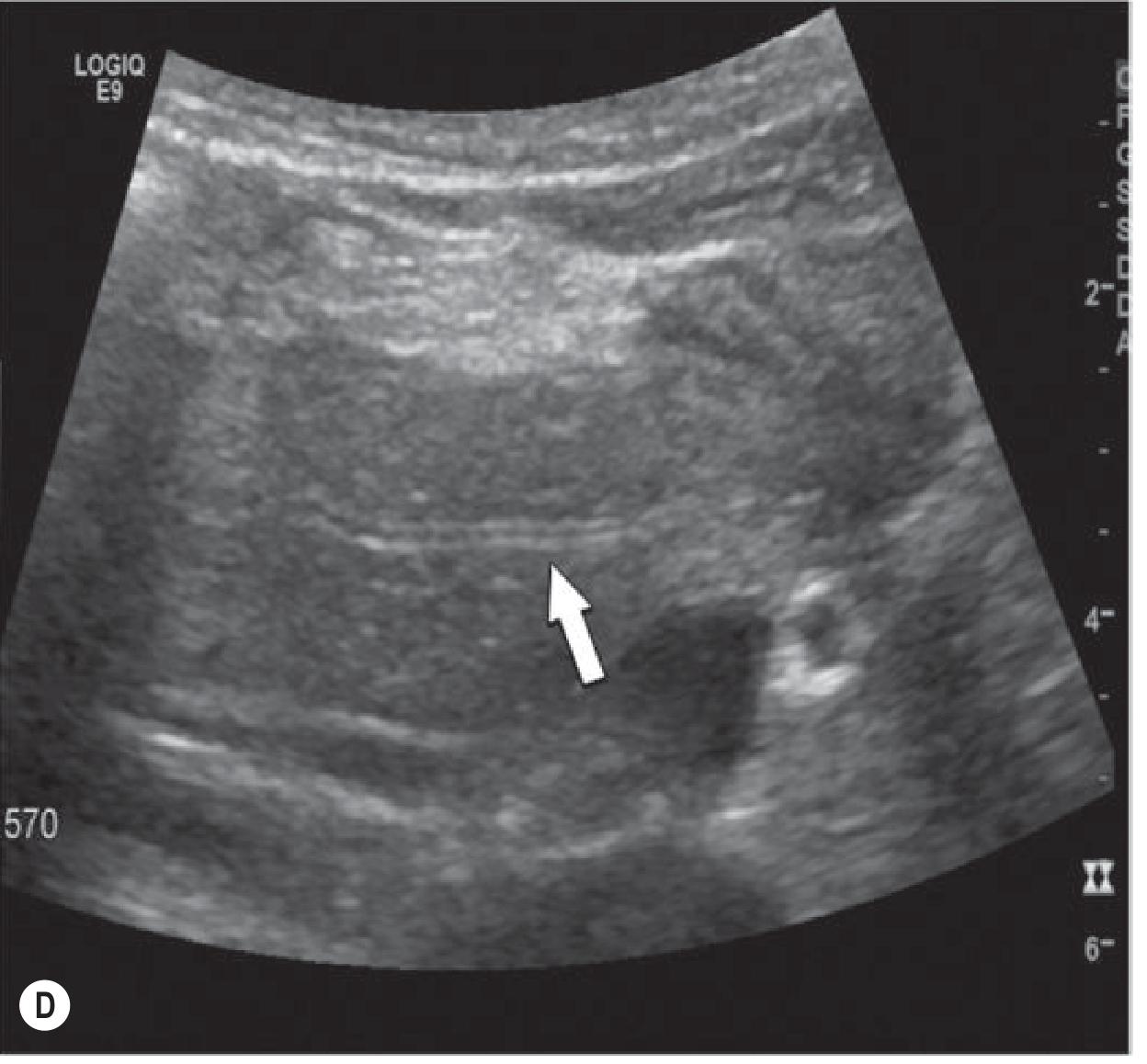 Ultrasound shows diffuse swelling of the gland with reduced reflectivity and a small rim of peripancreatic fluid (arrow). - Grainger & Allison's Diagnostic Radiology
Ultrasound shows diffuse swelling of the gland with reduced reflectivity and a small rim of peripancreatic fluid (arrow). - Grainger & Allison's Diagnostic Radiology
Contrast-Enhanced CT (CECT)
The gold standard for staging and assessing complications. Indications include:
- Diagnostic uncertainty
- Failure to improve clinically within 48-72 hours
- Suspected complications (necrosis, abscess, vascular injury)
Important caveat: CT performed in the first 24 hours may underestimate the degree of necrosis, which can take 2-3 days to fully develop.
CT: Appropriate timing of imaging - early vs. day 3:
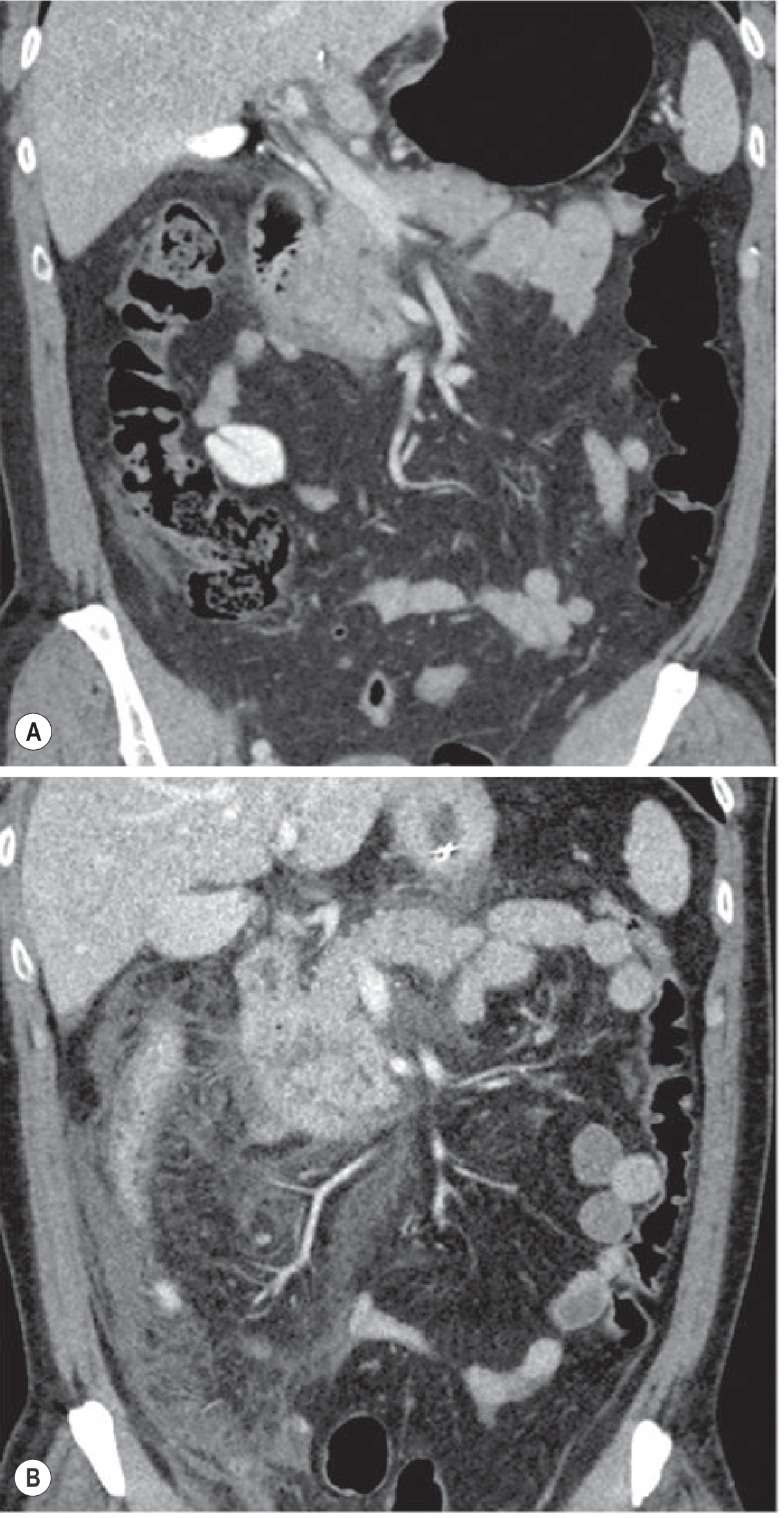 (A) CT performed 12 hours after onset shows only minimal signs. (B) Follow-up CT on day 3 (prompted by clinical deterioration) reveals extensive inflammation. - Grainger & Allison's Diagnostic Radiology
(A) CT performed 12 hours after onset shows only minimal signs. (B) Follow-up CT on day 3 (prompted by clinical deterioration) reveals extensive inflammation. - Grainger & Allison's Diagnostic Radiology
CT: Axial section showing acute pancreatitis with peripancreatic inflammation:
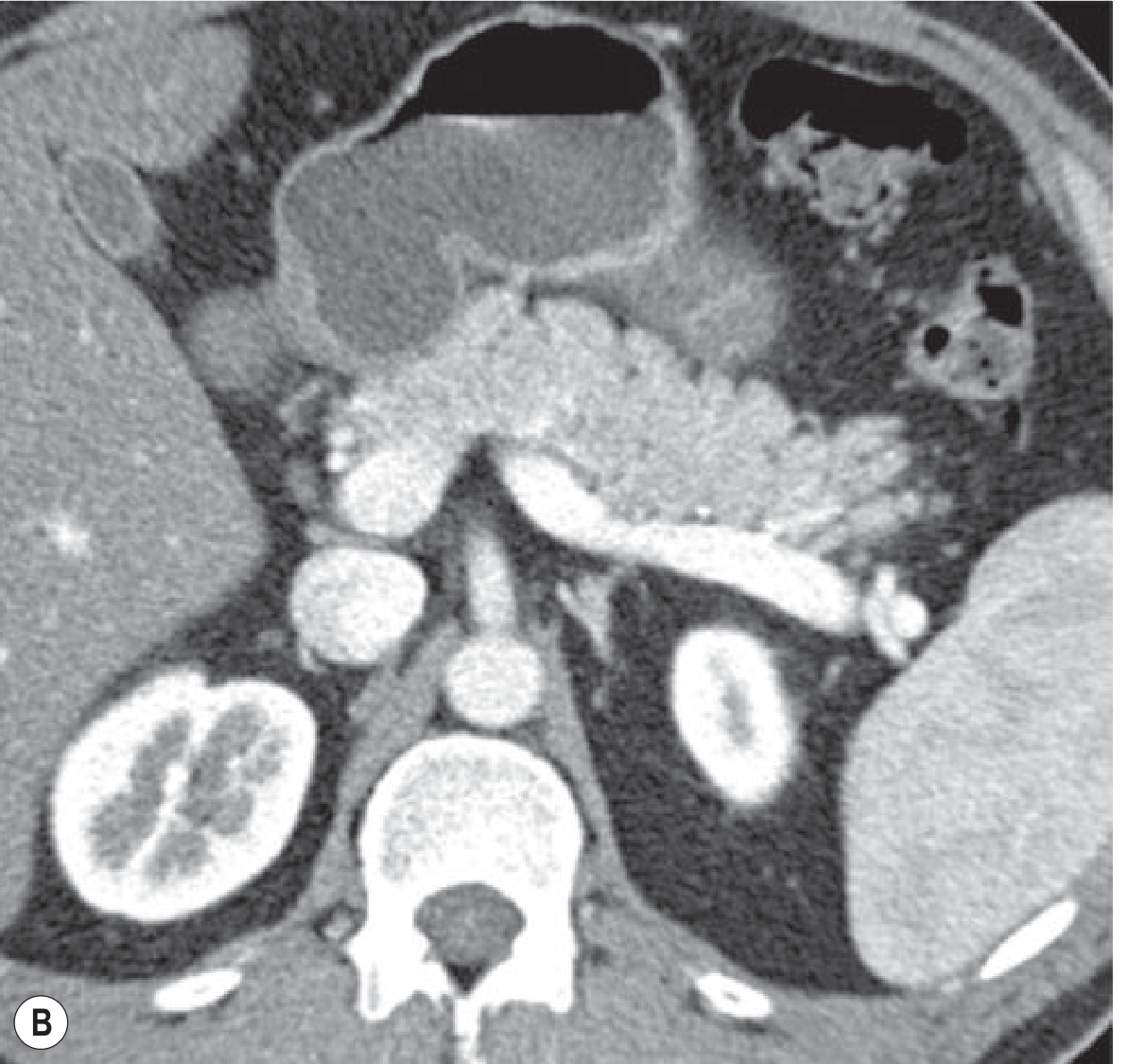 Axial CT demonstrating pancreatic body/tail with inflammatory changes. - Grainger & Allison's Diagnostic Radiology
Axial CT demonstrating pancreatic body/tail with inflammatory changes. - Grainger & Allison's Diagnostic Radiology
MRI / MRCP
Preferred over CT when renal failure precludes IV contrast, or to evaluate the pancreatic duct and identify choledocholithiasis without ERCP. MRCP has largely replaced diagnostic ERCP.
- Grainger & Allison's Diagnostic Radiology, pp. 677-681
Severity Classification (Revised Atlanta)
| Category | Definition |
|---|---|
| Mild | No organ failure, no local/systemic complications; self-limiting |
| Moderately Severe | Organ failure lasting <48 hours OR local/systemic complications without persistent organ failure |
| Severe | Persistent organ failure (>48 hours), single or multi-organ |
Severe AP is associated with mortality of ~29.5%, predominantly from organ failure (respiratory or hemodynamic) or infection.
Severity Scoring Systems
Ranson's Criteria (1974)
Assessed at admission (5 criteria) and at 48 hours (6 criteria). Score ≥3 predicts severe disease.
| At Admission | At 48 Hours |
|---|---|
| Age >55 years | Hematocrit fall >10% |
| WBC >16,000/mm³ | BUN rise >5 mg/dL |
| Blood glucose >200 mg/dL | Ca²⁺ <8 mg/dL |
| LDH >350 IU/L | PaO₂ <60 mmHg |
| AST >250 IU/L | Base deficit >4 mEq/L |
| Fluid sequestration >6 L |
BISAP Score
A simpler bedside tool - one point for each:
- BUN >25 mg/dL
- Impaired mental status
- SIRS (≥2 of 4 criteria)
- Age >60 years
- Pleural effusion
CT Severity Index (CTSI) - Modified
| Prognostic Indicator | Points |
|---|---|
| Normal pancreas | 0 |
| Intrinsic abnormalities ± peripancreatic fat changes | 2 |
| Peripancreatic fluid collection or fat necrosis | 4 |
| No pancreatic necrosis | 0 |
| Necrosis ≤30% | 2 |
| Necrosis >30% | 4 |
| Extrapancreatic complications (pleural effusion, ascites, vascular, GI) | 2 |
Total 0-2 = Mild; 4-6 = Moderate; 8-10 = Severe
Note: CT scoring alone does not supersede clinical scoring systems for identifying severe pancreatitis.
- Grainger & Allison's Diagnostic Radiology, p. 681
- Sleisenger & Fordtran's GI and Liver Disease, p. 174
Management
1. Fluid Resuscitation (Most Important Step)
Aggressive IV fluid replacement is the single most important intervention:
- 250-500 mL/hr of isotonic crystalloid (lactated Ringer's preferred by many guidelines)
- Higher rates for patients with hypotension and tachycardia
- Goal: decrease BUN; hematocrit may be elevated from hypovolemia due to third-spacing
- Most beneficial in the first 12-24 hours - may minimize or prevent pancreatic necrosis
- Avoid over-resuscitation (abdominal compartment syndrome risk)
2. Pain Management
Adequate analgesia is essential - IV opioids are standard. NSAIDs and metamizole are alternatives. Good analgesia may reduce the inflammatory response.
3. Nutrition
- Mild AP: Oral feeding can restart immediately once nausea/vomiting have resolved and pain is controlled. A low-fat solid diet is as safe as a clear liquid diet.
- Severe AP: Early enteral nutrition is preferred over parenteral nutrition - reduces infectious complications and cost.
- Nasogastric (NG) feeding appears as effective as nasojejunal feeding, but nasojejunal tubes are preferred when gastric retention occurs from duodenal edema.
- NPO >7 days requires nutritional support.
4. Antibiotics
- Not started routinely - no benefit in sterile pancreatitis.
- Indicated for extrapancreatic infections (e.g., cholangitis, pneumonia) or infected necrotizing pancreatitis.
5. ERCP
Reserved for specific indications only:
- Concurrent cholangitis → ERCP within 24 hours
- Biliary obstruction (elevated bilirubin) with suspected choledocholithiasis
- Not indicated for routine uncomplicated gallstone pancreatitis
- MRCP or EUS should be used first to screen for CBD stones - prevents unnecessary ERCP
6. Cholecystectomy (for Gallstone AP)
-
Laparoscopic cholecystectomy within 3 days of admission in mild biliary pancreatitis improves outcomes and decreases the need for ERCP.
-
Early cholecystectomy is the standard of care.
-
In patients not fit for surgery, ERCP with biliary sphincterotomy reduces risk of recurrent gallstone pancreatitis.
-
Sleisenger & Fordtran's GI and Liver Disease, Clinical GI Endoscopy, pp. 2783-2787
-
Textbook of Family Medicine 9e, pp. 1137-1138
Local Complications (Revised Atlanta Nomenclature)
| Complication | Timing | Description |
|---|---|---|
| Acute peripancreatic fluid collection | <4 weeks | No defined wall; usually resolves spontaneously |
| Pancreatic pseudocyst | >4 weeks | Encapsulated fluid collection from ductal leak; no solid debris |
| Acute necrotic collection | <4 weeks | Contains variable amounts of both fluid and necrotic tissue |
| Walled-off necrosis (WON) | >4 weeks | Mature, encapsulated necrosis; may be sterile or infected |
Endoscopic drainage is used for symptomatic and/or infected collections in close proximity to the gastric or duodenal wall.
Systemic Complications
- Hypovolemia and shock
- Acute renal failure
- Hepatic dysfunction
- Hypocalcemia (from saponification of fat)
- ARDS / respiratory failure
- Pleural effusion
- Colonic infarction (due to thrombosis of middle or right colic artery) - may present as rapid hemodynamic collapse; requires emergent laparotomy
Special Populations: Pediatric AP
Etiology differs from adults - biliary tract disease (10-30%), medications (25%, especially valproate and L-asparaginase), systemic disease (33%, including hemolytic uremic syndrome, SLE), trauma (10-40%), and metabolic causes. Genetic mutations (SPINK1, CFTR combinations) are found in many "idiopathic" cases and should be tested after recurrent episodes.
- Sleisenger & Fordtran's GI and Liver Disease, p. 14 (pediatric chapter)
Key Take-Aways
- Most cases (80%) are mild and self-limiting; ~20% develop severe disease
- Gallstones and alcohol account for ~80% of all etiologies - always get an abdominal ultrasound
- Aggressive IV fluid resuscitation in the first 12-24 hours is the cornerstone of management
- Antibiotics are not given prophylactically
- Enteral nutrition is preferred over parenteral in severe disease
- Early ERCP only for cholangitis or confirmed biliary obstruction; early cholecystectomy is standard for biliary AP
- CT should be reserved for diagnostic uncertainty or clinical deterioration, ideally after 48-72 hours
This is a shared conversation. Sign in to Orris to start your own chat.