infection vs subclinical infection
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Here is a thorough comparison, drawn from authoritative medical textbooks:
Infection vs. Subclinical Infection
Definitions
| Feature | Clinical (Overt) Infection | Subclinical (Inapparent) Infection |
|---|---|---|
| Pathogen entry & replication | Yes | Yes |
| Signs & symptoms | Present | Absent |
| Immune/serological response | Present | Present |
| Pathogen shedding | Yes | Yes (same as clinical) |
| Detectable by clinical exam | Yes | No - lab tests only |
| Appears in disease statistics | Yes | No |
The Spectrum of Disease (Gradient of Infection)
The term "spectrum of disease" is a graphic representation of variations in disease manifestations - like the spectrum of light, where it is difficult to determine exactly where one color ends and the next begins. At one end lie subclinical infections (not ordinarily identified), and at the other end are fatal illnesses. The middle contains mild-to-severe illness. These different manifestations reflect individuals' different states of immunity and receptivity.
In infectious diseases specifically, this spectrum is called the "gradient of infection" - Park's Textbook of Preventive and Social Medicine, p. 50.
Three Tiers of Host Response
Park's classifies infection in a host as:
-
Clinical infection - illness that may be mild, moderate, severe, or fatal. Mild/ambulant cases are often epidemiologically more important because they spread infection widely, while severe cases remain bedridden.
-
Subclinical infection (also: inapparent, covert, missed, or abortive cases):
- The disease agent multiplies but produces no signs or symptoms
- The agent is still shed and excreted (feces, respiratory droplets, etc.) identically to clinical cases
- Persons are "sick unbeknownst to themselves and others"
- They contribute more to transmission than symptomatic patients, yet never appear in any disease statistics
- Detected only by: organism recovery, antibody response, biochemical tests, or skin sensitivity tests
- Play a dominant role in maintaining endemicity in the community
-
Latent infection - must be distinguished from subclinical infection:
- The host does not shed the infectious agent
- The agent lies dormant within the host, without symptoms and often without detectable presence in blood/tissues/secretions
- Examples: herpes simplex, Brill-Zinsser disease, slow virus infections, ancylostomiasis
The Iceberg Phenomenon
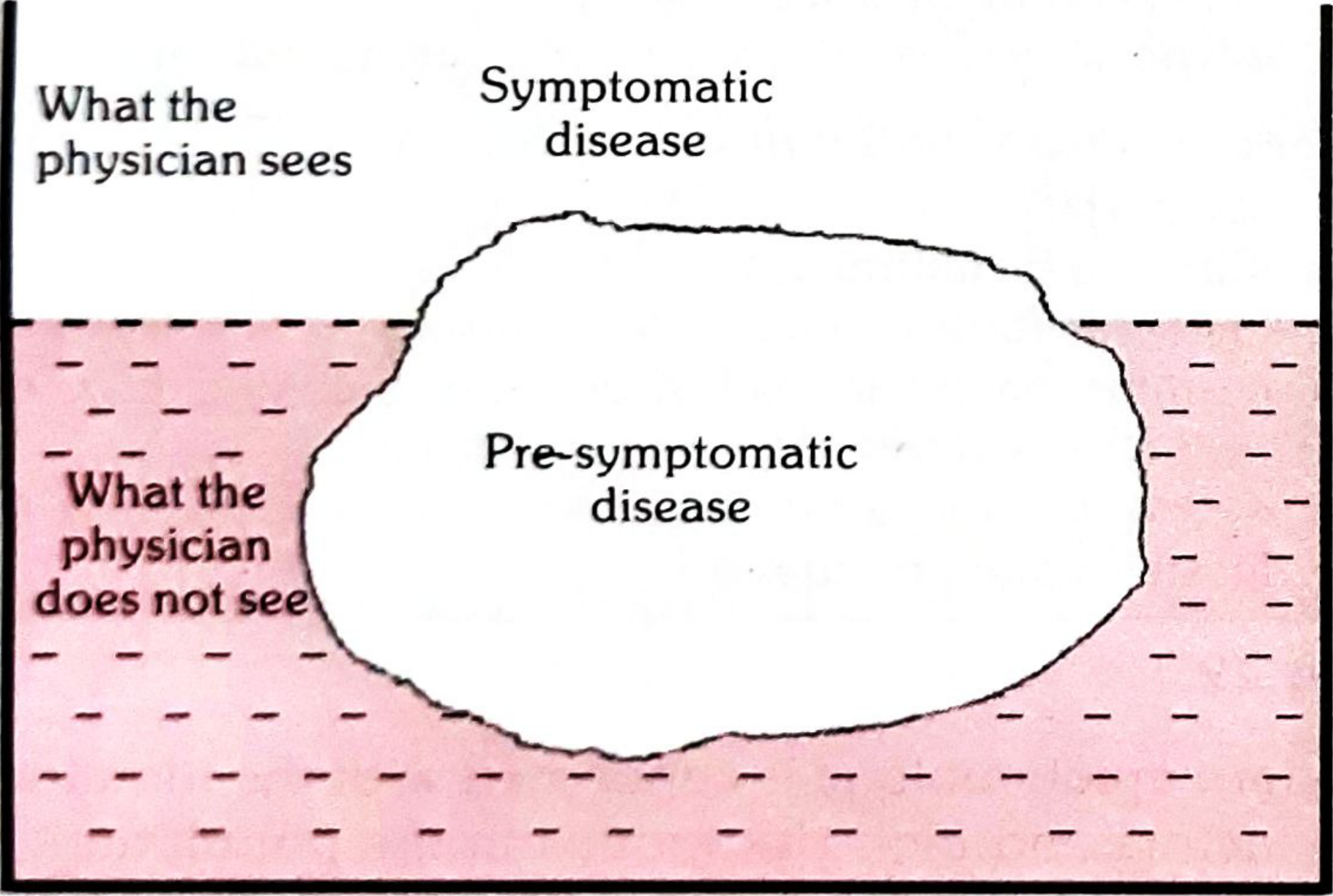
Fig. 10 - The Iceberg of Disease (Park's Textbook of Preventive & Social Medicine)
The floating tip = what the physician sees (clinical cases). The vast submerged portion = the hidden mass of disease: latent, inapparent, presymptomatic, and undiagnosed cases and carriers. The "waterline" separates apparent from inapparent disease.
In many diseases (hypertension, diabetes, anaemia, malnutrition), the hidden portion far exceeds known morbidity. This hidden reservoir is a major public health challenge.
Diseases With High Subclinical Rates
The following diseases have a great deal of subclinical infection (Park's):
- Rubella, mumps, polio
- Hepatitis A and B
- Japanese encephalitis
- Influenza
- Diphtheria
Exceptions with very low subclinical rates: measles (nearly all infections become clinical), rabies (almost universally fatal).
Epidemiological significance of subclinical infections: Since subclinical infections occur frequently over a lifetime, they are responsible for the natural immunity adult humans show against a variety of pathogens - essentially acting as silent natural immunization.
Summary: Key Distinction
| Clinical Infection | Subclinical Infection | Latent Infection | |
|---|---|---|---|
| Symptoms | Yes | No | No |
| Pathogen shedding | Yes | Yes | No |
| Serological evidence | Yes | Yes | Sometimes |
| Detectable clinically | Yes | No | No |
| Epidemiological risk | High (known) | Higher (unknown, ambulant) | Low (dormant) |
The most important point: subclinical infections are not harmless from a public health standpoint - they are often more dangerous than clinical ones precisely because they go undetected while actively spreading the pathogen.
Sources: Park's Textbook of Preventive and Social Medicine, pp. 45, 50; Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.; Sherris & Ryan's Medical Microbiology, 8th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.