HbA1c- 14.6
HbA1c- 14.6, FBS- 440, PPBS- 430 what OHA to be started?
Reading File
Finding Sources
Finding Sources
Searching PubMed
type 2 diabetes HbA1c very high insulin versus oral antidiabetic
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching PubMed
"type 2 diabetes" AND "insulin" AND "very poorly controlled" AND "HbA1c"
Finding Sources
Finding Sources
Reading File
Searching PubMed
"type 2 diabetes" AND "insulin" AND "HbA1c" AND "initiation"
Loading Image
Here is a thorough, evidence-based answer:
Clinical Assessment
| Parameter | Value | Interpretation |
|---|---|---|
| HbA1c | 14.6% | Severely uncontrolled (normal <5.7%; target <7%) |
| FBS | 440 mg/dL | Severe fasting hyperglycemia |
| PPBS | 430 mg/dL | Severe postprandial hyperglycemia |
Should You Start OHA or Insulin?
At HbA1c 14.6% with glucose >400 mg/dL, insulin is the preferred initial therapy - not OHA alone.
Here is why:
-
Glucose toxicity: Chronic severe hyperglycemia directly impairs beta-cell function ("glucose toxicity"), reducing insulin secretory capacity by up to 50%. OHAs that depend on functioning beta cells (sulfonylureas, DPP-4 inhibitors, GLP-1 agonists) will be less effective until glucose toxicity is reversed. - Harrison's Principles of Internal Medicine 22E
-
ADA threshold: When HbA1c is >10-12% at presentation, most guidelines recommend starting insulin, either alone or in combination with metformin, to rapidly bring down glucose and reverse glucose toxicity. At 14.6%, this is well above that threshold.
-
OHA monotherapy will fail: Metformin typically lowers HbA1c by 1-2%, sulfonylureas by 1-1.5%. With a target of <7%, you need an ~8% reduction - this cannot be safely achieved with OHA alone.
Recommended Management Plan
Step 1 - Rule out DKA/HHS first
With glucose >400, check urine/serum ketones, blood pH, and electrolytes to rule out DKA or HHS, which require urgent IV insulin and hydration.
Step 2 - Start Insulin (Primary therapy)
Basal insulin is the standard starting point:
| Insulin | Dose | Timing |
|---|---|---|
| Glargine (Lantus) or Degludec (Tresiba) | 0.1-0.2 U/kg/day | Once daily (night) |
| OR: NPH insulin | 0.1-0.2 U/kg/day | Bedtime |
- Start at 10 units basal insulin at bedtime, or weight-based (0.1-0.2 U/kg)
- Titrate by 2 units every 3 days targeting FBS 80-130 mg/dL
- If PPBS remains high after FBS is controlled, add prandial (short-acting) insulin
Step 3 - Add Metformin (Simultaneously, if no contraindications)
Metformin should be started alongside insulin, or shortly after:
- Metformin 500 mg once daily with meals, titrate to 500-1000 mg twice daily over 2-4 weeks (extended-release formulation preferred to reduce GI side effects)
- Contraindications: eGFR <30, contrast dye exposure, severe hepatic disease, metabolic acidosis
"Metformin remains the consensus first line of therapy and should be started at the time of diagnosis... for individuals failing to reach target, basal insulin addition to metformin leads to slightly better glycemic control." - Goodman & Gilman's Pharmacological Basis of Therapeutics
Step 4 - After Glucose Toxicity is Reversed (HbA1c <10%)
Once glucose is controlled (usually 4-8 weeks), reassess. At that point you may:
- Continue metformin + basal insulin (most common)
- Consider adding a GLP-1 receptor agonist (semaglutide, liraglutide) if cardiovascular risk is present
- Consider SGLT-2 inhibitor (empagliflozin, dapagliflozin) if heart failure or diabetic nephropathy is present - these have proven mortality benefit
- Consider sulfonylurea (glimepiride 1-2 mg/day, or glipizide 5 mg/day) as a cheaper add-on if insulin is not available
Type 2 Diabetes Treatment Algorithm
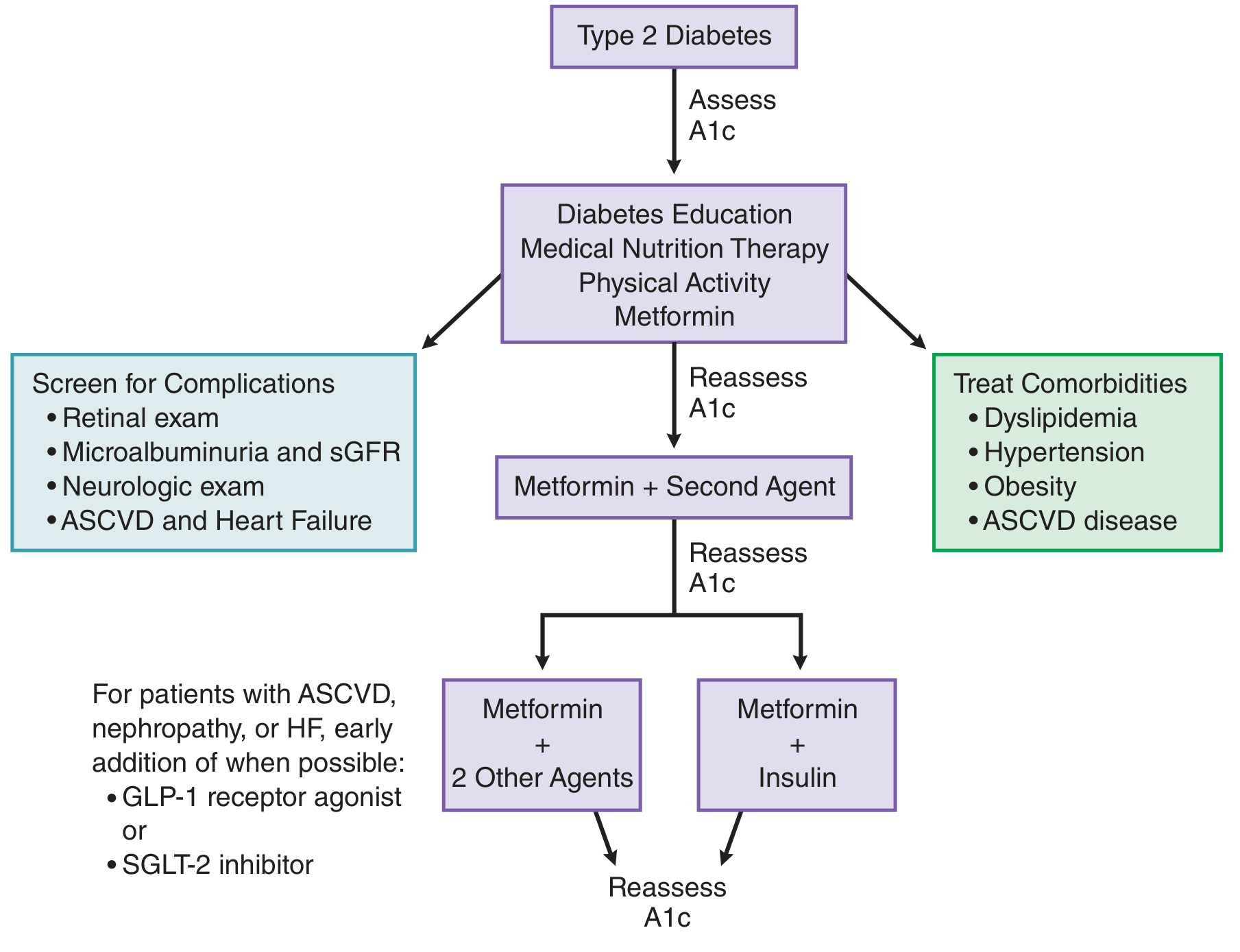
Source: Goodman & Gilman's Pharmacological Basis of Therapeutics
Summary
| Priority | Action |
|---|---|
| Immediate | Rule out DKA/HHS; start basal insulin (10 U or 0.1-0.2 U/kg) |
| Same time | Start metformin 500 mg BD (if renal function normal) |
| Monitor | FBS daily; titrate insulin every 3 days |
| Re-evaluate at 4-8 weeks | Add GLP-1 agonist or SGLT-2i based on comorbidities |
| Do NOT start | Sulfonylurea alone, DPP-4i alone, or SGLT-2i alone at this glucose level |
Do not start insulin secretagogues (sulfonylureas) as sole therapy at this level - the pancreas is exhausted from glucose toxicity, and hypoglycemia risk from these agents is also significant once glucose begins falling rapidly.
Disclaimer: This is educational clinical guidance. Actual prescribing decisions must be made by a qualified clinician based on full patient assessment, renal function, comorbidities, and clinical context.
This is a shared conversation. Sign in to Orris to start your own chat.