Acute onset painless vision loss detailed information
Reading File
Finding Sources
Finding Sources
Searching PubMed
"painless vision loss" acute causes management
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have excellent material for a detailed, well-organized response. Let me compile the comprehensive answer.
Acute Onset Painless Vision Loss
Acute painless vision loss is a medical emergency. It requires rapid evaluation to identify the underlying cause, many of which are sight-threatening or life-threatening. The key clinical distinction is whether it is monocular or binocular, transient or permanent, and how sudden the onset was.
Classification by Onset and Duration
| Pattern | Typical Cause |
|---|---|
| Transient monocular (<30 min) | Amaurosis fugax (TIA of the eye) |
| Sudden permanent monocular | CRAO, CRVO, AION, vitreous haemorrhage, retinal detachment |
| Gradual monocular | Chronic glaucoma, cataract, macular degeneration |
| Binocular | Cortical/occipital infarction, bilateral AION (GCA) |
1. Amaurosis Fugax (Transient Visual Loss)
Mechanism: Transient monocular painless vision loss, classically described as "a curtain coming down over the eye." Usually lasts a few minutes and recovers in the same pattern, though usually more gradually.
Causes (Amaurosis Fugax Study Group classification):
- Embolic (most common) - carotid or cardiac origin
- Hemodynamic - severe carotid stenosis with hypoperfusion
- Ocular - raised IOP, hyperviscosity
- Neurologic - optic nerve lesion
- Idiopathic
Key point: Embolic amaurosis fugax carries a high risk of stroke. Investigation and systemic management are the same as for retinal artery occlusion and must be undertaken urgently. Frequency can range from several attacks per day to once every few months. Attacks may sometimes be accompanied by contralateral cerebral TIA symptoms.
- Kanski's Clinical Ophthalmology 10th Ed.
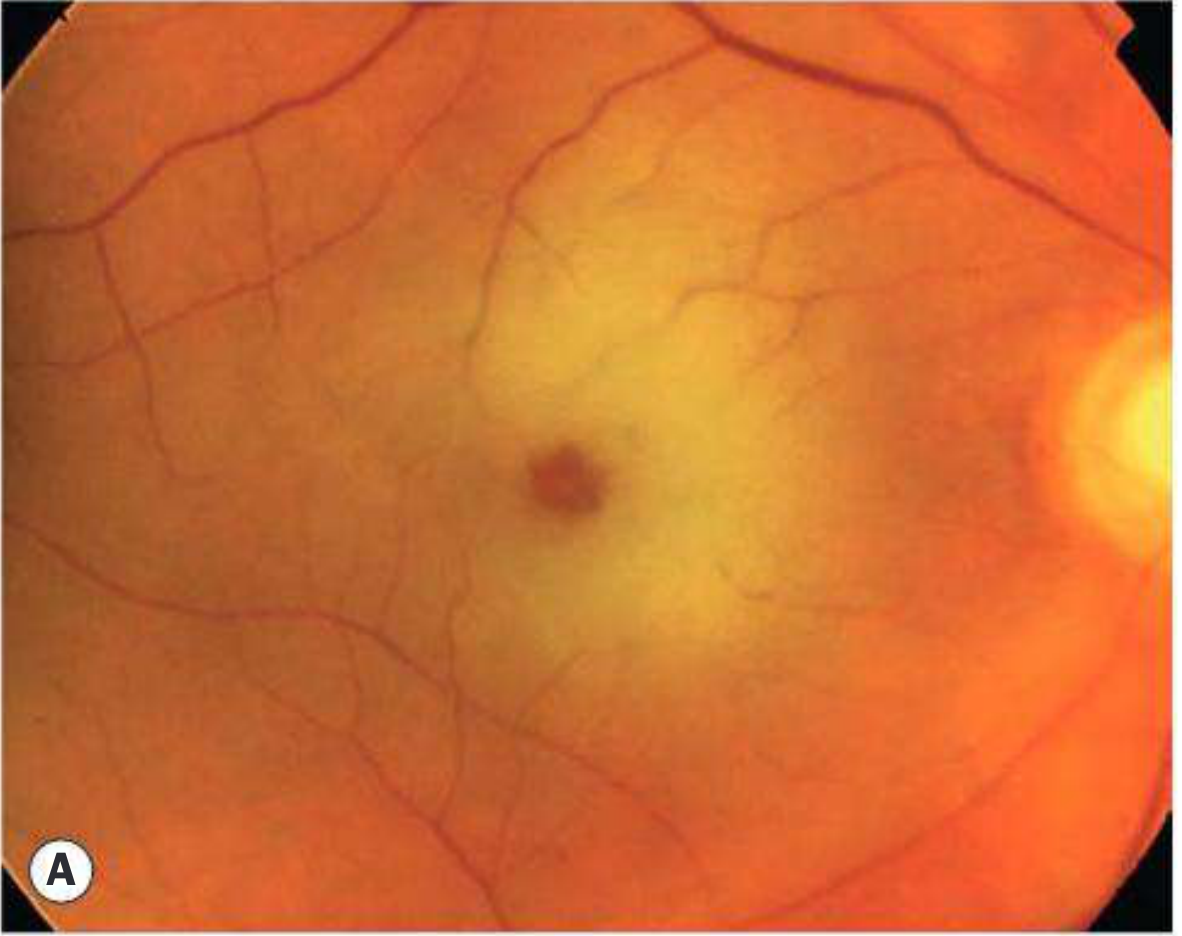
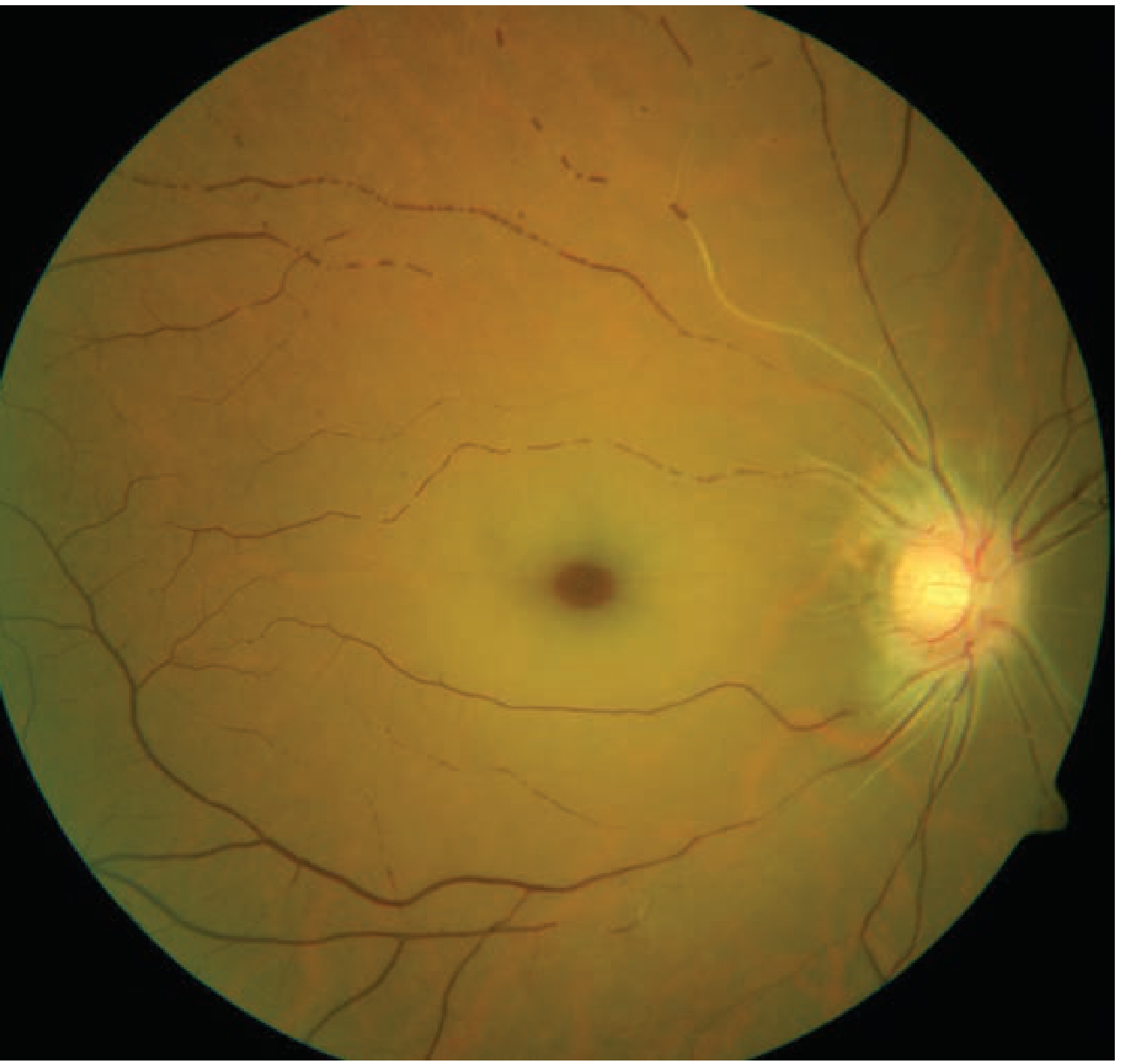
2. Central Retinal Artery Occlusion (CRAO)
CRAO is an ophthalmic stroke. It accounts for approximately 1 in 10,000 ophthalmic visits.
Symptoms
- Sudden, profound, painless monocular vision loss occurring over seconds
- Vision usually counting fingers to light perception (94% of eyes)
- Often preceded by episodes of amaurosis fugax
Signs
- Profound RAPD (relative afferent pupillary defect) - sometimes a complete "amaurotic" pupil
- Cherry-red spot at the macula - the foveola's thin retina allows the normal choroidal circulation to show through, contrasting with surrounding pale ischaemic retina
- Pale, oedematous retina in all quadrants
- Attenuated arteries with "cattle-trucking" or "box-car" segmentation of blood column
- Peripapillary retinal swelling
Special variant
- Cilioretinal artery (present in ~20% of people): if it supplies the papillomacular bundle, central vision can be partially preserved despite total CRAO
- GCA-related CRAO: absence of light perception; combined with anterior ischaemic optic neuropathy; very poor prognosis
Causes
Carotid or cardiac embolus, retinal artery thrombosis, giant cell arteritis, vasculitis (SLE, PAN), sickle cell disease, trauma, vasospasm (migraine), elevated IOP (glaucoma), hypercoagulable states, hypotension/severe carotid stenosis.
Treatment (Time-critical - window ~4-6 hours)
Irreversible retinal damage occurs after approximately 4-6 hours of ischaemia. Two-thirds of patients end up with final VA worse than 6/120.
The following can be attempted for occlusions < 6 hours:
- Ocular massage - using a three-mirror contact lens or through closed eyelids. 10-15 seconds pressure, then release, for 3-5 minutes. Aims to mechanically dislodge embolus/thrombus by alternating flow.
- Anterior chamber paracentesis - 27-gauge needle to lower IOP abruptly
- IOP-lowering drugs - topical timolol, acetazolamide
- CO2 inhalation / paper bag breathing - to cause vasodilation
- IV tPA (alteplase) - 0.9 mg/kg within 4.5 hours of onset. 10% given over 1 minute, remainder over 59 minutes. Local intra-arterial thrombolysis has NOT shown benefit over conservative management. Evidence remains limited and ophthalmologists have not reached consensus.
Systemic workup (urgent - risk of stroke)
- 30% will have severe carotid disease, coincidental stroke or extreme hypertension
- 20% will have simultaneous MI or critical heart disease
- ~95% need a change in systemic medication
- 25% require urgent surgical intervention
Management: Urgent referral to stroke clinic. Antiplatelet therapy (aspirin loading 600 mg). Oral anticoagulation for AF. Carotid endarterectomy if stenosis >70%. Lipid-lowering therapy. Smoking cessation.
- Kanski's Clinical Ophthalmology 10th Ed.; Tintinalli's Emergency Medicine
3. Branch Retinal Artery Occlusion (BRAO)
- Sudden, profound painless altitudinal or sectoral visual field loss
- Can go unnoticed if central vision is spared
- RAPD often present
- Fundus: cloudy white oedematous ("ground glass") retina in the ischaemic zone; "cattle-trucking" of blood column; emboli visible at bifurcation points
- FA: delayed arterial filling and hypofluorescence due to retinal swelling
- Management same as CRAO (urgent systemic evaluation, antiplatelet therapy, stroke risk reduction)
- Review at 3 months
4. Central Retinal Vein Occlusion (CRVO)
- Vision loss is variable - from vague blurring to rapid, painless, monocular loss
- Risk factors: diabetes, hypertension, dyslipidaemia, hypercoagulable states, glaucoma, vasculitis
- Classic fundus: "blood and thunder" appearance - optic disc oedema with diffuse retinal haemorrhages in all quadrants
- Distinguishing features: contralateral optic nerve is normal (unlike papilloedema); haemorrhages are peripheral (unlike optic neuritis)
- Treatment: anti-VEGF injections; laser-induced chorioretinal anastomosis
- Consult neurology and ophthalmology
5. Non-Arteritic Anterior Ischaemic Optic Neuropathy (NAION)
Mechanism: Occlusion of the short posterior ciliary arteries causing partial or total infarction of the optic nerve head. The "crowded disc" (absent physiological cup) is a structural predisposition.
Predispositions: Hypertension (very common), diabetes, hyperlipidaemia, sleep apnoea syndrome, collagen vascular disease, antiphospholipid antibody syndrome, hyperhomocysteinaemia, sudden hypotensive events, cataract surgery, high altitude. Patients usually >50 years, but younger than arteritic AION.
Symptoms
- Sudden painless monocular visual loss, frequently discovered on awakening (suggesting nocturnal hypotension plays a role)
Signs
- VA: normal or slightly reduced in ~30%; moderate-to-severe impairment in the remainder
- Visual field: typically inferior altitudinal defect (most characteristic), but also central, paracentral, quadrantic, or arcuate defects
- Dyschromatopsia proportional to visual impairment (unlike optic neuritis where colour vision is disproportionately affected)
- Diffuse or sectoral hyperaemic disc swelling with peripapillary splinter haemorrhages
- Disc swelling resolves and pallor ensues over 3-6 weeks
Prognosis
- Improvement in vision is common; recurrence in ~6%
- About 50% achieve 6/9 or better; 25% only reach 6/60 or worse
- Fellow eye involvement: ~10% after 2 years, ~15% after 5 years
Treatment
- No definitive treatment
- Exclude GCA (ESR, CRP, temporal artery biopsy if any doubt)
- Treat underlying systemic conditions
- Aspirin frequently prescribed for systemic vascular risk reduction
- Optic nerve fenestration is NOT beneficial
- Short-term steroids advocated by some authorities
6. Arteritic Anterior Ischaemic Optic Neuropathy (AAION) - GCA
Mechanism: Giant cell arteritis (GCA) is a granulomatous necrotizing arteritis affecting large and medium arteries. AAION affects 30-50% of untreated GCA patients. One-third develop fellow-eye involvement, usually within a week.
Symptoms of GCA
- Scalp tenderness (noticed on combing hair)
- Headache (frontal, occipital, or temporal)
- Jaw claudication (pathognomonic) - cramp on chewing due to masseter ischaemia
- Weight loss, fever, night sweats, malaise
- Polymyalgia rheumatica (PMR) in ~50% at diagnosis
- Double vision
Ocular symptoms
- Sudden, profound unilateral visual loss, not uncommonly preceded by amaurosis fugax
- Prognosis is very poor; typically more severe than NAION
Epidemiology
- Average age: 70 years; extremely rare under 50
- Women affected 4x more than men
Investigations
| Test | Finding |
|---|---|
| ESR | Typically >50 mm/h (ACR criterion) |
| CRP | Often markedly elevated |
| Platelets | Thrombocytosis common |
| Temporal artery biopsy (TAB) | >2.5 cm specimen; granulomatous arteritis with giant cells; sensitivity ~77% |
| Temporal artery ultrasound (Doppler) | Hypoechoic "halo" sign in ~75%; valid non-invasive alternative to TAB |
| Liver function | Abnormal in 1/3 |
Note: A negative TAB should not prevent treatment if clinical picture is convincing (~20% have normal histology). Never delay steroids pending biopsy - perform TAB within 3 days of starting steroids.
ACR 1990 Criteria (3 of 5 required):
- Age ≥50 at onset
- New headache
- Temporal artery tenderness or decreased pulsation
- ESR ≥50 mm/h
- Abnormal artery biopsy (granulomatous inflammation with multinucleated giant cells)
Treatment
- Without visual symptoms: Oral prednisolone 1 mg/kg/day
- With visual symptoms / AAION: High-dose IV methylprednisolone (500 mg-1 g/day for 3 days), then oral prednisolone to prevent fellow-eye involvement
- Duration: 1-2 years; some need indefinite maintenance
- Monitor ESR and CRP
- Do not taper rapidly, especially below 10 mg/day
7. Vitreous Haemorrhage
- Mild: sudden floaters and diffuse blurring without significant VA reduction
- Dense: severe, sudden painless vision loss
- Causes: Acute posterior vitreous detachment with retinal tear or vessel avulsion, proliferative diabetic retinopathy, retinal vein occlusion, sickle cell disease, trauma, Terson syndrome (vitreous + subarachnoid haemorrhage from aneurysmal rupture)
- Investigations: B-scan ultrasound is critical to exclude retinal detachment or choroidal melanoma underlying a dense haemorrhage
- Treatment: Early vitrectomy increasingly adopted for dense haemorrhage; otherwise observation
Terson syndrome: Intraocular haemorrhage combined with subarachnoid haemorrhage, most commonly from anterior communicating artery aneurysm. Usually bilateral; typically intraretinal/preretinal. Vitreous haemorrhage usually resolves within months with good visual prognosis; early vitrectomy may be considered.
8. Retinal Detachment
- Preceding symptoms: photopsia (flashes of light), floaters, and a "curtain or shadow" across the visual field
- If the macula is detached - sudden onset of painless, blurred central vision
- Three types:
- Rhegmatogenous (most common) - retinal break/tear with vitreous fluid entry
- Tractional - fibrovascular membranes pulling retina (diabetic retinopathy)
- Exudative/serous - fluid accumulation without break (choroidal tumour, inflammation)
- Emergency if macula-on (central vision intact); surgery within 24 hours
- Examination: raised, corrugated retinal folds; if detachment is large, the retina billows forward
9. Ocular Ischaemic Syndrome (OIS)
- Results from chronic ocular hypoperfusion due to severe (>90%) ipsilateral carotid atherosclerotic stenosis
- Typically affects older patients with diabetes and hypertension
- Presents with dull periorbital ache (can be painless) and gradual or acute visual symptoms
- Signs include dilated tortuous retinal veins, retinal haemorrhages, neovascularization
- Associated with very high cardiovascular mortality
Differential Diagnosis Summary by Laterality
| Feature | CRAO | CRVO | NAION/AAION | Retinal Detachment | Vitreous Haemorrhage |
|---|---|---|---|---|---|
| Laterality | Unilateral | Unilateral | Unilateral | Unilateral | Unilateral |
| Onset | Seconds | Hours-days | On waking | Gradual (with prodrome) | Sudden |
| Pain | None | None | None (NAION) / Headache (GCA) | None | None |
| Visual field | Total loss | Variable | Altitudinal (inferior) | Curtain/sector | Diffuse blurring |
| RAPD | Profound | Present | Present | Present (if macula off) | Variable |
| Fundus | Cherry-red spot | Blood and thunder | Disc swelling | Elevated retina | No fundus view |
| Age | >60 | Any | >50 | Any | Any |
| Key systemic clue | AF, carotid disease | HTN, DM | Sleep apnoea, nocturnal hypotension | Myopia, prior trauma | DM, bleeding disorder |
Immediate Emergency Assessment
- Visual acuity both eyes
- Pupillary responses - look for RAPD (afferent defect = retinal/optic nerve pathology)
- Confrontation visual fields
- Slit-lamp - anterior segment for cells/flare
- Fundoscopy (direct and indirect) - disc, macula, vessels, vitreous, periphery
- IOP measurement
- B-scan ultrasound if fundus not visible
Urgent systemic workup
- BP, ECG (AF?), fasting lipids, glucose, FBC, ESR/CRP, coagulation screen
- Carotid Doppler ultrasound
- Echocardiogram if cardiac embolism suspected
- If GCA suspected: temporal artery biopsy / ultrasound; do not delay steroids
Key Mnemonics
Causes of acute painless vision loss (CRAVE TV):
- C - CRAO/CRVO
- R - Retinal detachment
- A - AION (NAION/AAION-GCA)
- V - Vitreous haemorrhage
- E - Embolic (amaurosis fugax)
- T - Temporal arteritis (GCA)
- V - Vascular occlusion (ophthalmic artery)
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed. | Tintinalli's Emergency Medicine, 9th Ed. | Goldman-Cecil Medicine | Textbook of Family Medicine, 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.