Cerebral palsy physiotherapu assessment and management give a short introduction and clinical
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cerebral palsy"[MeSH Terms] AND "physical therapy"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Cerebral Palsy: Physiotherapy Assessment and Management
Introduction
Cerebral palsy (CP) is defined as a group of permanent disorders of the development of movement and posture, causing activity limitation, attributed to non-progressive disturbances that occurred in the developing fetal or infant brain (Rosenbaum et al., 2007). Despite the underlying brain lesion being static (non-progressive), the clinical expression changes dynamically with growth and aging - making CP better understood as an evolving condition rather than a truly "static" one.
To diagnose CP, five criteria must be met:
- A disorder of movement and/or posture (weakness, spasticity, dystonia, ataxia, or choreoathetosis) with onset before age 1-2 years
- Reliable evidence of a fetal or infant brain disturbance
- No evidence of progression over time
- Significant functional limitation in activities
- Reasonable expectation the disorder persists lifelong
(Bradley and Daroff's Neurology in Clinical Practice)
Epidemiology and Causes
CP affects approximately 2-3 per 1,000 live births. Adults with CP now outnumber children by a ratio of 3:1 in many countries.
Congenital CP (85-90% of cases) results from brain injury before or during birth. Acquired CP (remaining ~10-15%) arises after the first month of life - most commonly from perinatal stroke (ischemic, hemorrhagic, or thromboembolic), followed by meningitis/encephalitis in infancy.
Key risk factors:
- Prematurity (strongest single risk; incidence 8.7% in <32 weeks gestation vs. 0.6% in 34-37 weeks)
- Very low birth weight (<1,500 g)
- Periventricular/intraventricular hemorrhage
- TORCH infections (Toxoplasmosis, Other, Rubella, CMV, Herpes)
- Perinatal hypoxic-ischemic injury
- Multiple gestations (largely mediated through prematurity)
(Bradley and Daroff's Neurology in Clinical Practice)
Classification
By Motor Type
| Type | Features | Prevalence |
|---|---|---|
| Spastic | Velocity-dependent increase in muscle tone, hyperreflexia, Babinski sign, clonus - upper motor neuron injury | 70-80% |
| Dyskinetic | Dystonia, chorea, athetosis, or combinations; due to basal ganglia injury | ~15% |
| Ataxic/Hypotonic | Cerebellar or hypotonic features, balance and coordination deficits | ~5% |
| Mixed | Combination of the above | Variable |
By Topography (Spastic CP)
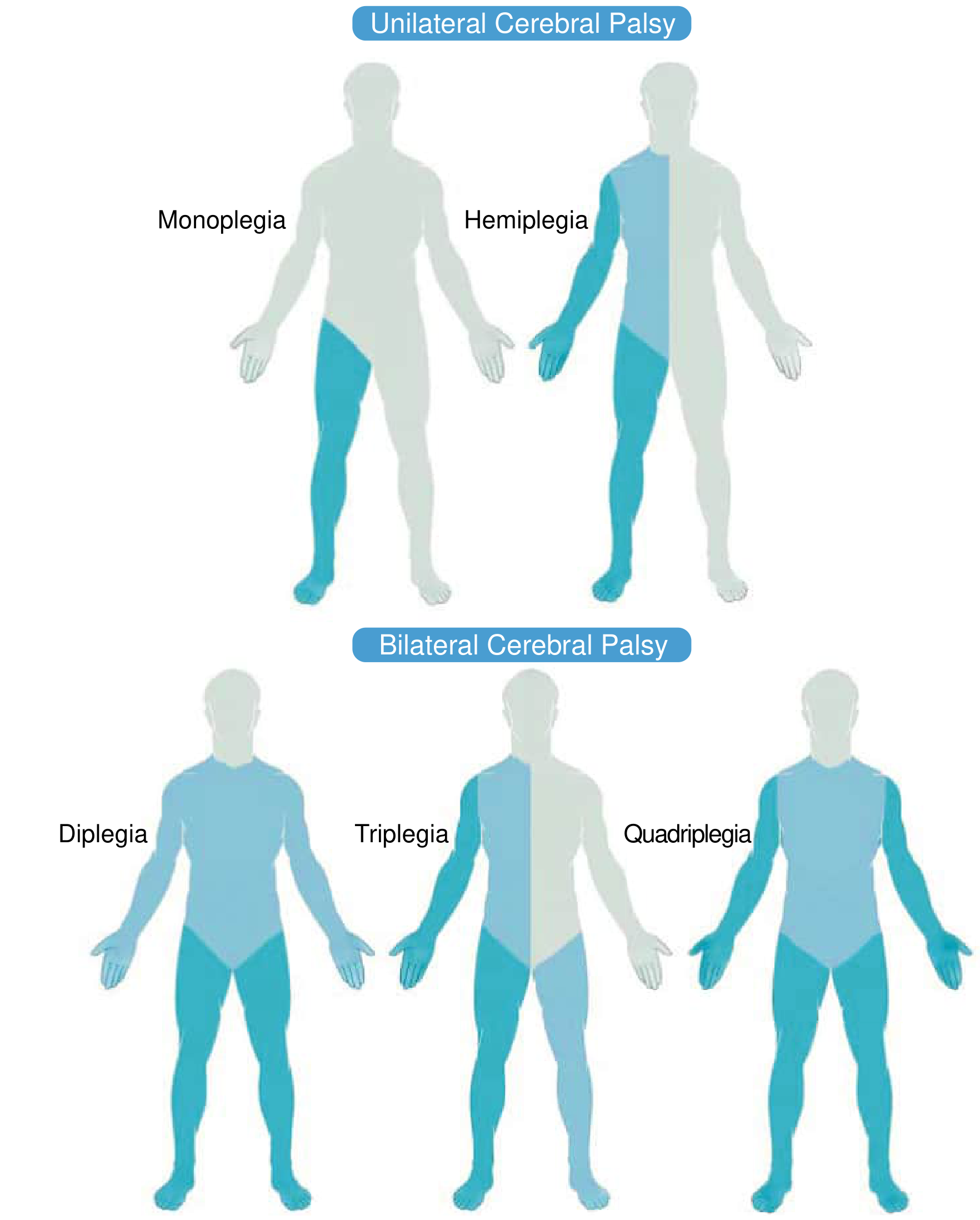
- Monoplegia - one limb affected
- Hemiplegia - one side (arm + leg), usually arm more than leg
- Diplegia - legs predominantly, arms less so (classic in periventricular leukomalacia)
- Triplegia - both legs and one arm
- Quadriplegia - all four limbs plus trunk and face
Gross Motor Function Classification System (GMFCS)
A 5-level system used universally to classify functional mobility:
- Level I: Walks without restrictions
- Level II: Walks with limitations outdoors
- Level III: Walks with assistive devices
- Level IV: Self-mobility limited, uses powered wheelchair
- Level V: Transported in manual wheelchair; no independent mobility
GMFCS IV/V patients carry a nearly 50% risk of developing spinal deformity (scoliosis).
Clinical Features
Upper Motor Neuron Syndrome
CP primarily produces features of UMN syndrome, which are divided into:
Positive features (targetable with intervention):
- Spasticity
- Clonus
- Hyperreflexia with radiation
- Extensor/flexor spasms
- Positive Babinski sign
- Involuntary activation of remote muscles
Negative features (more causative of disability, less responsive to treatment):
- Muscle weakness
- Loss of selective motor control
- Loss of dexterity
- Fatigability
- Cognitive, communication, and behavioral changes
(Bradley and Daroff's Neurology in Clinical Practice)
Characteristic Postures and Gait Patterns
- Upper limb: elbow flexion, wrist/finger flexion, shoulder internal rotation, forearm pronation
- Lower limb: hip flexion and adduction, knee flexion, toe walking
- Gait patterns: toe-walking, crouched gait, jump gait, scissor gait (hip adduction)
Associated Conditions
- Epilepsy (30-50%)
- Intellectual disability
- Sensory impairments (vision, hearing)
- Communication/speech difficulties
- Feeding and swallowing dysfunction (sialorrhea common - may require physiotherapy measures, posture optimization, or botulinum toxin to submandibular ducts)
- Depression (prevalence up to double the general population in adults, correlating with functional disability)
- Cervical myelopathy in dyskinetic CP (onset typically 4th decade due to sustained involuntary movements causing degenerative changes)
Physiotherapy Assessment
A structured PT assessment follows a biopsychosocial framework using the ICF (International Classification of Functioning, Disability, and Health).
History
- Pregnancy history: gestational age, birth weight, perinatal complications, NICU course
- Developmental trajectory: motor, language, visual-motor milestones
- Current functional abilities, assistive devices used
- Pain complaints and fatigue (very common in adults)
- Previous interventions: botulinum toxin, surgeries, orthoses
Physical Examination
1. Tone Assessment
- Modified Ashworth Scale (MAS) or Tardieu Scale for spasticity
- Distinguish spasticity (velocity-dependent) from dystonia (sustained abnormal postures) and rigidity
2. Range of Motion (ROM)
- Passive and active ROM of all joints
- Hip: Thomas test (hip flexion contracture), Ober test (IT band tightness), Staheli test (hip extension)
- Knee: popliteal angle for hamstring tightness
- Ankle: Silfverskiöld test (distinguishes gastrocnemius vs. soleus tightness)
- Foot: Coleman block test (hindfoot flexibility in cavovarus)
3. Strength Assessment
- Selective motor control (proximal and distal)
- Manual muscle testing (often limited by poor cooperation in younger children)
- Functional strength testing
4. Reflexes and Primitive Reflexes
- Persistent primitive reflexes (ATNR, STNR, Moro) beyond expected integration age
- Deep tendon reflexes: hyperreflexia typical
- Babinski sign
5. Posture and Alignment
- Static and dynamic postural control
- Pelvic tilt, trunk alignment
- Hip surveillance (radiographic hip migration percentage monitored regularly)
- Spinal curves: scoliosis assessment (particularly GMFCS IV/V)
6. Gait Analysis
- Clinical observational gait analysis
- Instrumented 3D gait analysis (gold standard for surgical planning): assesses kinematics, kinetics, and EMG to identify pathological patterns and guide multi-level surgical decisions
- Common patterns: equinus, crouch gait, jump gait, stiff-knee gait (rectus femoris overactivity)
7. Functional Assessments (Outcome Measures)
- GMFCS - functional mobility classification
- MACS (Manual Ability Classification System) - hand function
- CFCS (Communication Function Classification System)
- Gross Motor Function Measure (GMFM-66 or GMFM-88) - quantifies motor function and tracks change over time
- Pediatric Evaluation of Disability Inventory (PEDI)
- 6-Minute Walk Test - endurance in ambulatory patients
Physiotherapy Management
The overarching goal is to maximize function by improving biomechanics through tone management, addressing musculoskeletal deformities, and building strength. Treatment is best delivered in a multidisciplinary setting embedding rehabilitation within a patient-centered framework involving physiatry, orthopaedics, PT, OT, speech therapy, and primary care.
(Bradley and Daroff's Neurology in Clinical Practice)
1. Physiotherapy Techniques
Stretching and Passive ROM
- Regular stretching to prevent/delay contracture formation
- Sustained (static) stretching preferred for spastic muscles
- Serial casting used for progressive contractures (commonly ankle, knee, elbow)
Strengthening
- Progressive resistance training - shown to improve strength without worsening spasticity
- Focus on weak antagonists (hip extensors/abductors, ankle dorsiflexors)
- Task-specific training improves motor learning
Neurodevelopmental Treatment (NDT) / Bobath Approach
- Facilitates normal movement patterns; inhibits abnormal reflex activity
- Widely used but evidence base continues to evolve
Constraint-Induced Movement Therapy (CIMT)
- Used in hemiplegic CP: constrains unaffected limb to force use of affected arm
- Good evidence for improving upper limb function in hemiplegia
Treadmill and Gait Training
- Partial body-weight-supported treadmill training
- Robotics-assisted gait training (Lokomat) in non/low-ambulatory patients
- Improves walking speed, endurance, and GMFM scores
Hydrotherapy
- Warm water reduces muscle tone temporarily, allowing improved ROM and movement
- Useful for strengthening in reduced gravity environment
Functional Electrical Stimulation (FES)
- Peroneal nerve FES for foot drop/equinus
- Improves dorsiflexion during gait
2. Orthotic Management (PT co-managed)
- Ankle-Foot Orthoses (AFO) - most commonly used; prevents equinus, supports walking
- Solid AFO, hinged AFO, ground reaction AFO (for crouch gait)
- Knee-Ankle-Foot Orthoses (KAFO) - for more proximal weakness
- Hip abduction orthoses - in early hip subluxation
- Upper limb splints - wrist/hand in hemiplegic CP
3. Pharmacological Management (PT works alongside)
Oral Medications for Diffuse Spasticity
- Baclofen (first-line) - GABA-B agonist
- Tizanidine, dantrolene, benzodiazepines (diazepam)
- Second-line: clonidine or gabapentin (dual benefit for tone and sleep, pain, dysautonomia)
Focal Spasticity - Chemodenervation
- Botulinum Toxin A (BoNT-A) - gold standard for focal spasticity
- Injections every 4-6 months (minimum 3 months to avoid resistance)
- Targets specific overactive muscles (e.g., gastrocnemius, hip adductors, rectus femoris)
- Maximally effective when combined with physiotherapy immediately post-injection
- Phenol / Ethyl alcohol - nerve blocks for larger muscle groups
Intrathecal Baclofen (ITB)
- For severe, widespread spasticity not adequately controlled with oral baclofen
- Delivers baclofen directly to CSF at a fraction of the oral dose
- Avoids systemic side effects (sedation, weakness, GI symptoms)
- Reversible (unlike SDR)
- Requires test dose before pump implantation
4. Surgical Management (PT role: pre/post-op rehab)
Soft Tissue Procedures
- Tendon lengthening/release (gastrocnemius-soleus, hamstrings, hip flexors, adductors)
- Tendon transfers (e.g., split anterior tibialis transfer - SPLATT - for spastic varus)
- Rectus femoris transfer/release for stiff-knee gait
Bony Procedures
- Femoral/tibial derotation osteotomies for rotational malalignment
- Hip reconstruction (varus derotation osteotomy + acetabuloplasty) for subluxation/dislocation
Selective Dorsal Rhizotomy (SDR)
- Surgical sectioning of sensory nerve rootlets (L1-S1) reducing spastic input
- Best candidates: spastic diplegia, GMFCS II-III, age 4-8 years, no fixed contractures
- Produces permanent, significant spasticity reduction
- Intensive post-operative PT for 12-24 months is mandatory
Spinal Fusion for Scoliosis
- Indicated for curves >50 degrees in skeletally immature or progressive curves
- Posterior instrumentation with pedicle screws; pelvic fixation preferred for pelvic obliquity
- Complication rates reported up to 81% (infection 15-19%); pulmonary management is critical perioperatively
(Campbell's Operative Orthopaedics 15th Ed 2026; Bradley and Daroff's Neurology in Clinical Practice)
Adult Considerations in CP
- Gait and self-care worsen in a substantial proportion of adults
- Pain and fatigue are frequent complaints (multifactorial: hypertonia, musculoskeletal changes, reduced rehabilitation access)
- Dyskinetic CP is complicated by cervical spine degeneration and myelopathy (onset ~4th decade)
- Depression prevalence up to double the general population
- Orthopedic interventions become less important once the skeleton matures; tone management and seizure management remain lifelong priorities
Summary Table: Physiotherapy Framework
| Domain | Assessment Tools | Interventions |
|---|---|---|
| Tone | Modified Ashworth Scale, Tardieu Scale | Stretching, casting, BoNT-A, oral baclofen |
| ROM/Contracture | Goniometry, Silfverskiöld, Thomas test | Serial casting, SDR, tendon surgery |
| Strength | MMT, dynamometry | Resistance training, FES |
| Gait | Observational + 3D gait analysis | Treadmill training, BWSTT, AFOs |
| Function | GMFM, MACS, PEDI, 6MWT | Task-specific therapy, CIMT |
| Posture/Spine | Spinal X-ray, GMFCS | Seating systems, bracing, spinal fusion |
| Upper limb | MACS, grip strength | CIMT, splints, OT |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Campbell's Operative Orthopaedics 15th Ed 2026; Miller's Review of Orthopaedics 9th Ed; Bailey and Love's Short Practice of Surgery 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.