

Already on metformin
Reading File
Finding Sources
Finding Sources
Searching PubMed
type 2 diabetes metformin inadequate glycemic control add-on therapy
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-sourced answer. Here is the full analysis:
Lab Results Summary - Mr. Sandeep Soni Ji, 58M (Dated 27/06/2026)
🔴 Key Abnormal Findings
| Test | Result | Status | Normal |
|---|---|---|---|
| HbA1c | 8.32% | ⬆ HIGH | <5.7% (non-diabetic); Goal of therapy <7.0% |
| Average Blood Glucose | 192.08 mg/dL | ⬆ HIGH | 80-140 mg/dL (good control) |
| Serum Triglycerides | 171.96 mg/dL | ⬆ BORDERLINE HIGH | Desirable <150 mg/dL |
✅ Values Within Normal Range
| Test | Result | Normal |
|---|---|---|
| Total Cholesterol | 168.64 mg/dL | Desirable <200 |
| HDL | 48.32 mg/dL | 35-79.5 |
| LDL | 85.93 mg/dL | 60-165 |
| VLDL | 34.39 mg/dL | 20-50 |
| Cholesterol/HDL Ratio | 3.49 | Low Risk (3.32-4.40) |
| LDL/HDL Ratio | 1.78 | Low Risk (<3.0) |
Clinical Interpretation
1. Diabetes - Inadequately Controlled on Metformin
The HbA1c of 8.32% is clearly in the diabetic range and above the therapeutic target of <7.0%. The report itself notes "action suggested: >8.0%" - his value crosses this threshold, meaning a medication change or addition is needed. Average blood glucose of ~192 mg/dL corresponds to "poor control" by the lab's own reference.
Metformin can reduce HbA1c by 1.0-1.5%, but since he is already on it, monotherapy is no longer sufficient. A second agent must be added.
2. What to Add to Metformin? (Goldman-Cecil Medicine treatment algorithm)
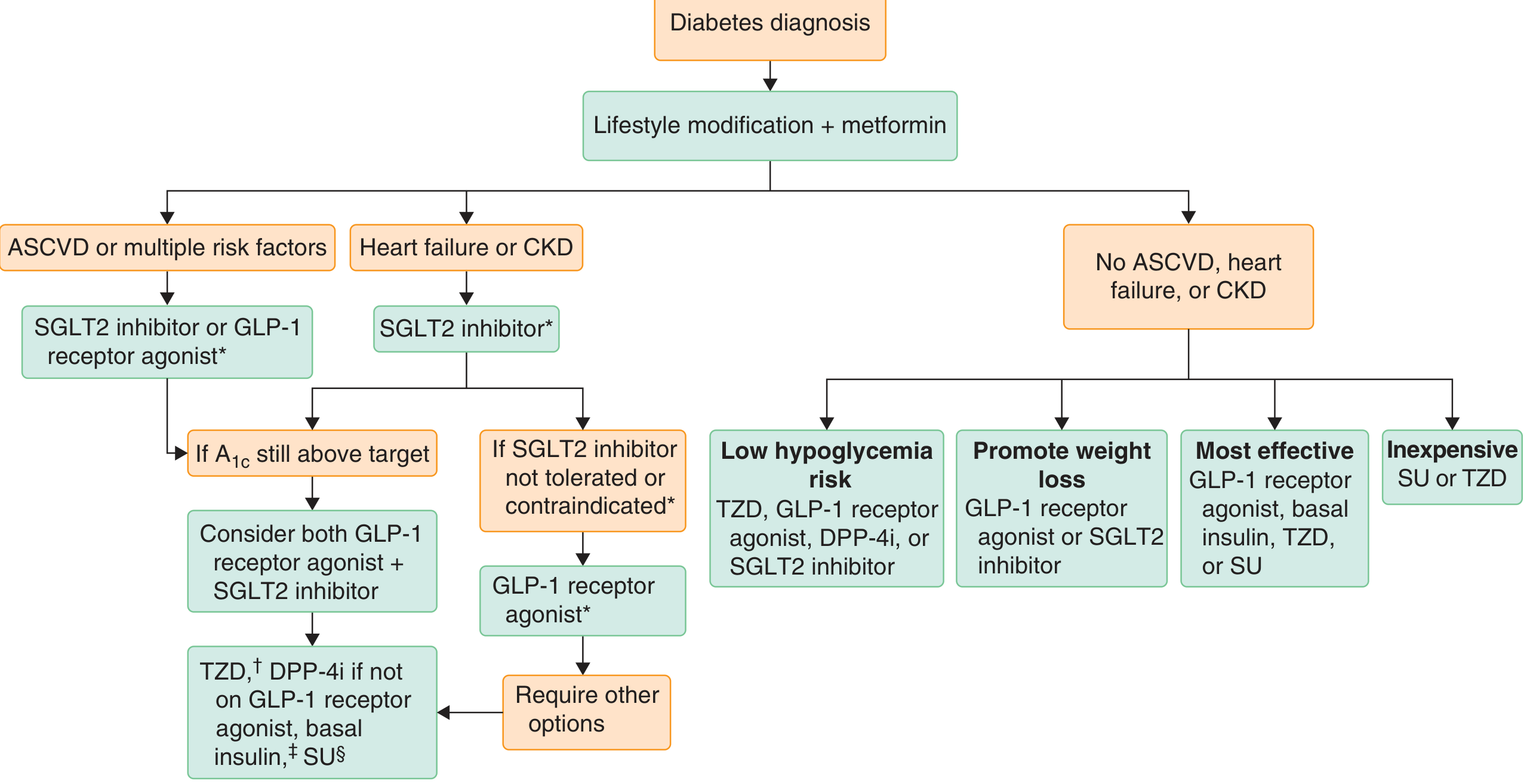
The choice of second agent depends on clinical priorities:
| Priority | Best Add-On | Notes |
|---|---|---|
| Proven CV benefit / multiple risk factors (age 58M is a risk factor) | SGLT2 inhibitor (empagliflozin, dapagliflozin) or GLP-1 RA (semaglutide, liraglutide) | Guidelines strongly prefer these first |
| Weight loss needed | GLP-1 RA or SGLT2 inhibitor | Both cause weight loss; GLP-1 RA also reduces triglycerides |
| Cost-conscious | Sulfonylurea (glimepiride) or TZD (pioglitazone) | Effective but SU causes weight gain and hypoglycemia risk |
| Low hypoglycemia risk | DPP-4 inhibitor (sitagliptin), GLP-1 RA, SGLT2i | All three |
At age 58 with borderline-high triglycerides and diabetes, a GLP-1 receptor agonist is particularly attractive - it lowers HbA1c by ~1.0-1.2%, reduces triglycerides, promotes weight loss, and has cardiovascular outcome benefits (semaglutide, liraglutide, dulaglutide). - Goldman-Cecil Medicine, International Edition
The SGLT2 inhibitors are also excellent if there is any concern about cardiac or kidney disease.
3. Triglycerides - Borderline High (171.96 mg/dL)
At 171.96 mg/dL, this falls in the borderline-high zone (150-199 mg/dL). This does not yet require drug therapy but warrants attention:
- For TG <200 mg/dL: first-line treatment is lifestyle modification - weight reduction and increased physical activity. - Tietz Textbook of Laboratory Medicine, 7th Ed.
- Drug therapy (fibrates, high-intensity statins, omega-3) is considered when TG reaches 200-499 mg/dL.
- Importantly, poorly controlled diabetes itself drives hypertriglyceridemia. Getting HbA1c under control will likely bring triglycerides down too.
- GLP-1 receptor agonists also independently lower triglyceride levels, making them doubly appropriate here.
Action Points for the Treating Doctor
- Add a second antidiabetic agent - GLP-1 receptor agonist (e.g., oral or injectable semaglutide) is a strong option given his age, TG elevation, and the need for HbA1c reduction >1%. SGLT2 inhibitor is an alternative.
- Check renal function (eGFR) before adding SGLT2i (needs eGFR >45) and ensure metformin dose is appropriate.
- Check Vitamin B12 - long-term metformin use is associated with B12 deficiency, which can worsen neuropathy.
- Lifestyle counseling - dietary fat/carbohydrate restriction, alcohol avoidance, and regular aerobic exercise will help both glycemic control and triglycerides.
- Repeat HbA1c in 3 months after medication adjustment to assess response.
- Triglycerides - reassess after glycemic control improves; if still elevated, consider fenofibrate.
Disclaimer: This analysis is for informational purposes only and is not a substitute for consultation with the treating physician. All medication changes should be made by a qualified doctor who knows the full clinical picture.
Sources: Goldman-Cecil Medicine International Edition; Katzung's Basic & Clinical Pharmacology 16th Ed.; Tietz Textbook of Laboratory Medicine 7th Ed.
Snake bite management
Reading File
Finding Sources
Searching PubMed
"snakebite" AND "management" AND "antivenom"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive, multi-source content. Here is the full structured guide on snakebite management:
Snakebite Management
1. Epidemiology & Overview
Snakebite is the world's deadliest neglected tropical disease. Estimates suggest 1.2-5.5 million bites annually worldwide, causing ~63,000-125,000 deaths and ~400,000 amputations. The burden falls overwhelmingly on South Asia, Sub-Saharan Africa, and Latin America - particularly among farmers, women, and children in rural communities. In India, the "big four" venomous snakes are the Indian cobra (Naja naja), Russell's viper (Daboia russelii), saw-scaled viper (Echis carinatus), and common krait (Bungarus caeruleus). - Park's Textbook of Preventive & Social Medicine; Harrison's 22E
Key fact: 70% of all snakebites are from non-venomous species. Of bites by venomous snakes, only ~50% actually envenomate the patient (the rest are "dry bites"). - Park's / Government of India National Protocol 2007
2. Types of Snake Venom
| Venom Type | Mechanism | Key Species | Clinical Effects |
|---|---|---|---|
| Cytotoxic / Haemotoxic | Tissue digestion, haemolysis, destroys endothelial lining | Vipers, Russell's viper | Local necrosis, swelling, coagulopathy, DIC, haemorrhage |
| Neurotoxic | Blocks neuromuscular transmission | Cobras, kraits, coral snakes, sea snakes | Ptosis, dysphagia, diplopia, respiratory paralysis |
| Mixed | Both effects | Some cobras, spitting cobras | Combined local + systemic |
3. Clinical Features
Warning Signs of Severe Envenomation
- Snake identified as a dangerous species
- Rapid early extension of local swelling from bite site
- Early tender regional lymphadenopathy (spread via lymphatics)
- Systemic symptoms: collapse, hypotension, shock, nausea, vomiting, severe headache
- Heaviness of eyelids / early ptosis or ophthalmoplegia
- Early spontaneous systemic bleeding (gums, nose, vomit, stool, urine)
- Dark brown/black urine (haemoglobinuria/myoglobinuria - indicates rhabdomyolysis/AKI)
Local Effects (Viper/Cytotoxic)
- Fang marks, pain, progressive oedema (can involve entire limb within 1 hour in severe cases)
- Ecchymosis, haemorrhagic blebs (may appear within hours)
- Local tissue necrosis


Systemic Effects (Neurotoxic - Elapids)
- Ptosis (often first sign), ophthalmoplegia, diplopia
- Dysphagia, dysphonia
- Respiratory failure (respiratory paralysis is the main cause of death)
- Altered sensorium
Haematological (Viper)
- Coagulopathy (DIC pattern): thrombocytopenia, elevated PT, low fibrinogen
- Haemolysis, haemoconcentration followed by anaemia
4. First Aid (Prehospital)
DO ✅
- Reassure the patient - panic increases heart rate and venom absorption
- Immobilize the bitten limb - splint as you would a fracture; keep at or below heart level
- Remove rings, bracelets, watches, tight clothing around the bitten limb (anticipate swelling)
- Clean the wound with soap and running water; cover with sterile dressing
- Transport immediately to the nearest facility with antivenom - this is the single most important step
- For elapid (neurotoxic) bites - apply pressure-immobilization bandage (wrap entire limb snugly, 40-70 mmHg; should allow 1-2 fingers underneath) to delay lymphatic absorption
- Take a photograph of the snake from a safe distance for identification - do NOT attempt to capture it
DO NOT ❌
| Harmful Practice | Reason |
|---|---|
| Tourniquets / tight ligatures | Cause ischaemia; do not prevent systemic envenomation |
| Incision and suction | Worsens local tissue damage, increases infection risk; ineffective |
| Ice application | Causes additional tissue injury |
| Alcohol / stimulants | Vasodilators - accelerate venom absorption |
| Seeking traditional healers first | Causes critical life-threatening delays |
| Electric shock "therapy" | No evidence; dangerous |
| Pressure immobilization for viper bites | Concentrates necrotizing venom locally - worsens tissue damage |
- Harrison's 22E; Tintinalli's Emergency Medicine; Park's / Government of India Protocol
5. Assessment at Health Facility
History
- Time of bite, snake description/photo
- First aid applied
- Symptoms developed since bite
Clinical Examination
- Fang marks (number, location)
- Extent of local swelling - mark the edge with pen and document time (advancing edge >10 cm/hour = indication for antivenom)
- Signs of systemic envenomation (as above)
- Vital signs: BP, pulse, SpO2, RR
Investigations (20WBCT - a quick bedside test)
20-Minute Whole Blood Clotting Test (20WBCT):
- Place 2 mL fresh venous blood in a clean glass test tube; leave undisturbed for 20 minutes
- If blood is non-clotting = viper envenomation with coagulopathy → antivenom indicated
- Repeat every 6 hours to monitor response
Lab tests:
- CBC, coagulation profile (PT, aPTT, fibrinogen, D-dimer)
- Serum creatinine, urea, electrolytes (renal function)
- Urine: appearance (dark = haemoglobin/myoglobin), dipstick for blood
- ECG, chest X-ray as needed
6. Antivenom - The Definitive Treatment
Indications for Antivenom
Give antivenom when ANY of the following are present:
| Category | Signs |
|---|---|
| Local | Rapid progressive swelling involving >half the bitten limb within hours; advancing edge >10 cm/h |
| Haematological | Positive 20WBCT (non-clotting blood), thrombocytopenia, active bleeding |
| Neurological | Ptosis, ophthalmoplegia, respiratory distress, bulbar palsy |
| Cardiovascular | Hypotension, shock, ECG changes |
| Renal | Oliguria, dark urine, rising creatinine |
Administration (Polyvalent Antivenom - India / South Asia)
- Skin test is NOT recommended by WHO - it is unreliable and causes delays without preventing anaphylaxis
- Dilute antivenom in 250-500 mL of 0.9% normal saline
- Infuse IV over 1 hour (not as IV push)
- Starting dose: 8-10 vials (adults and children receive the same dose - dose is based on venom, not body weight)
- If signs of envenomation persist or 20WBCT remains positive at 6 hours, repeat the same dose
- Keep adrenaline (epinephrine) 0.5 mg IM drawn up and ready before starting infusion
Antivenom Reactions
| Reaction | Time | Management |
|---|---|---|
| Early anaphylaxis | Within 10-180 min | Stop infusion immediately. Give adrenaline 0.5 mg IM (thigh). Antihistamines IV. Steroids IV. Restart when controlled at slow rate (5-10 mL/h, titrate up). |
| Pyrogenic reaction | 1-2 hours | Paracetamol, slow infusion rate |
| Serum sickness | 1-2 weeks later | Oral prednisolone 1-2 mg/kg/day, taper over 1-2 weeks; antihistamines |
- Harrison's 22E; Park's Textbook
7. Specific Complications and Management
Neurotoxic Envenomation (Elapids - Cobra, Krait)
- Give antivenom promptly
- Neostigmine + atropine trial: Neostigmine 0.5-2.5 mg IV/IM + Atropine 0.6 mg IV (blocks muscarinic side effects) - may reverse post-synaptic neurotoxicity (cobra); ineffective for pre-synaptic (krait)
- Endotracheal intubation and mechanical ventilation if respiratory failure - may be needed for days to weeks
- Monitor for aspiration
Haemotoxic / Coagulopathy (Vipers)
- Antivenom reverses coagulopathy within hours; blood products should ONLY be given after adequate antivenom to avoid fuelling consumptive coagulopathy
- Fresh frozen plasma (FFP) or whole blood if dangerously low fibrinogen/platelet count with active haemorrhage
- Avoid NSAIDs, aspirin (increase bleeding risk) - use paracetamol for analgesia
Acute Kidney Injury (AKI)
- Maintain urine output; IV fluids
- AKI is usually due to acute tubular necrosis and is frequently reversible with antivenom and supportive care
- Peritoneal dialysis or haemodialysis if oliguric renal failure develops
- Snake envenomation is a significant cause of AKI in South Asia (recent meta-analysis: PMID 41776424)
Rhabdomyolysis
- IV fluids, urinary alkalinization
- Monitor urine output, creatinine kinase
Local Necrosis / Wound
- Do NOT perform fasciotomy unless compartment pressure confirmed >30-40 mmHg after adequate antivenom has been given
- Tetanus prophylaxis
- Antibiotics only if wound was manipulated, incised, or mouth suction was applied (prophylactic antibiotics not routinely needed)
- Surgical debridement of necrotic tissue; skin grafting for major tissue loss at specialist centre
- Encourage early mobilization/exercises of the bitten limb
8. Referral Criteria (Transfer to Higher Centre)
Transfer patient if:
- 20WBCT still positive 6 hours after initial antivenom dose
- Progressive paralysis or respiratory difficulty
- Oliguria / rising creatinine
- Anaphylaxis unresponsive to adrenaline
- Shock unresponsive to fluids
- Severe necrosis or compartment syndrome signs
- No antivenom available at current facility
9. Management Summary by Level of Care
COMMUNITY (First Aid)
└─ Reassure, immobilize, remove jewellery, transport FAST
PRIMARY HEALTH CENTRE
└─ ABC assessment, 20WBCT, antivenom if available
└─ Paracetamol analgesia (NOT NSAIDs)
└─ IV saline for shock
└─ Transfer if not improving or antivenom unavailable
DISTRICT HOSPITAL
└─ Full bloods, ECG, urinalysis
└─ Antivenom (repeat doses as needed)
└─ Neostigmine/atropine for neurotoxic
└─ Intubation + ventilation for respiratory failure
└─ Dialysis for AKI
REFERRAL / SPECIALIST HOSPITAL
└─ ICU monitoring
└─ Advanced surgical management (skin grafting)
└─ Haemodialysis
└─ Renal/surgical specialities as needed
10. Monitoring
- Vital signs and neurological status: hourly in first 24 hours
- Mark swelling margins with time-stamped pen markings
- Repeat 20WBCT at 6 hours after antivenom dose
- Urine output hourly (catheterise if needed)
- All snakebite patients should be admitted for at least 24 hours even if initially asymptomatic, as envenomation signs can be delayed
Sources: Harrison's Principles of Internal Medicine 22E (2025); Tintinalli's Emergency Medicine: A Comprehensive Study; Park's Textbook of Preventive and Social Medicine; Government of India National Snakebite Protocol 2007
Snake bite management
I just covered snakebite management in detail in our previous conversation. Here's a concise structured summary you can reference quickly:
Snakebite Management - Quick Reference
Key Facts
- 70% of bites are from non-venomous snakes
- 50% of venomous bites are dry bites (no venom injected)
- Commonest cause of death: respiratory paralysis (elapids) and haemorrhage/AKI (vipers)
- India's "Big Four": Cobra, Russell's Viper, Saw-Scaled Viper, Common Krait
Venom Types
| Type | Species | Features |
|---|---|---|
| Neurotoxic | Cobra, Krait, Coral snake | Ptosis → respiratory failure |
| Haemotoxic/Cytotoxic | Russell's Viper, Saw-scaled Viper | Coagulopathy, local necrosis, AKI |
| Mixed | Some cobras | Both local + systemic |
Signs of Severe Envenomation
- Rapid advancing local swelling
- Tender regional lymphadenopathy
- Ptosis, ophthalmoplegia (neurotoxic)
- Spontaneous bleeding from gums/nose/urine
- Hypotension, shock
- Dark brown/black urine (rhabdomyolysis/haemolysis)
- Positive 20WBCT (blood non-clotting = viper coagulopathy)
First Aid - DO / DON'T
| ✅ DO | ❌ DO NOT |
|---|---|
| Reassure, keep calm | Apply tourniquet |
| Immobilize limb (splint) | Incise or suck the wound |
| Remove jewellery/tight clothing | Apply ice |
| Clean wound, cover with dressing | Give alcohol/stimulants |
| Transport IMMEDIATELY | Seek traditional healers first |
| Photograph snake from safe distance | Try to catch the snake |
| Pressure-immobilization bandage (elapids only) | Pressure bandage for viper bites |
20-Minute Whole Blood Clotting Test (20WBCT)
Place 2 mL blood in clean glass tube - leave 20 min undisturbed
- Non-clotting = viper envenomation → antivenom indicated
- Repeat at 6 hours post-antivenom to confirm response
Antivenom - The Only Definitive Treatment
Indications (any ONE present)
- Positive 20WBCT / active bleeding
- Ptosis, neurological signs
- Progressive swelling >half the limb / advancing >10 cm/hr
- Hypotension/shock
- Oliguria, dark urine
Administration
- Dilute 8-10 vials in 250-500 mL normal saline
- Infuse IV over 1 hour (never rapid IV push)
- Same dose for adults and children (based on venom quantity, not weight)
- No skin test - unreliable and causes harmful delay
- Have adrenaline 0.5 mg IM drawn up before starting
- Repeat dose at 6 hours if 20WBCT still positive or signs persist
Antivenom Reactions
| Reaction | Timing | Treatment |
|---|---|---|
| Anaphylaxis | 10-180 min | Stop infusion → Adrenaline 0.5 mg IM → Antihistamine + steroid IV → Restart slowly |
| Pyrogenic | 1-2 hr | Paracetamol, slow rate |
| Serum sickness | 1-2 weeks | Prednisolone 1-2 mg/kg/day, taper |
Complication Management
| Complication | Management |
|---|---|
| Respiratory paralysis | Intubation + mechanical ventilation (days to weeks); Neostigmine + Atropine trial (cobra) |
| Coagulopathy | Antivenom first; FFP/blood only AFTER adequate antivenom |
| AKI | IV fluids, monitor urine output; dialysis if oliguric |
| Local necrosis | Tetanus prophylaxis, antibiotics if wound manipulated, surgical debridement |
| Compartment syndrome | More antivenom first; fasciotomy only if pressure confirmed >30-40 mmHg post-antivenom |
| Rhabdomyolysis | IV fluids, urine alkalinization, monitor CK |
Analgesia: Paracetamol (adults 500 mg-1g; children 10-15 mg/kg) - avoid NSAIDs/aspirin (increase bleeding)
Transfer to Higher Centre If:
- 20WBCT positive at 6 hours after antivenom
- Progressive neurological deterioration
- Oliguria / rising creatinine
- Shock unresponsive to fluids
- Anaphylaxis unresponsive to adrenaline
- Compartment syndrome / severe necrosis
- No antivenom available
Monitoring (Minimum 24 hours admission)
- Hourly vitals + neurological status
- Mark swelling border with pen + timestamp
- Repeat 20WBCT at 6 hours post-antivenom
- Urine output monitoring (catheterize if needed)
- All patients admitted ≥24 hours - envenomation signs can be delayed
Sources: Harrison's Principles of Internal Medicine 22E (2025); Tintinalli's Emergency Medicine; Park's Textbook of Preventive & Social Medicine; Government of India National Snakebite Protocol 2007
This is a shared conversation. Sign in to Orris to start your own chat.