Types of uterine closure in lscs
uterine closure cesarean section single double layer
Uterine Closure in Lower Segment Caesarean Section (LSCS)
Types of Uterine Closure
1. Single-Layer Closure
- The uterine wall is closed with a single continuous suture incorporating the full thickness of the myometrium.
- Technically faster and associated with less blood loss intraoperatively.
- Disadvantage: Associated with a higher risk of:
- Uterine scar dehiscence/rupture in subsequent pregnancies
- Isthmocele (scar niche) formation — a defect in the anterior uterine wall
- Thinner residual myometrium at the scar site
2. Double-Layer Closure (traditionally standard practice)
- The uterine incision is repaired in two layers:
- First layer (inner/decidual): Closes the endometrium and inner myometrium — often with a locking (haemostatic) continuous suture
- Second layer (outer/muscular): Imbricates (inverts) the first layer using a continuous or interrupted suture through the outer myometrium
- Provides better haemostasis, stronger scar, and better anatomical apposition.
- Preferred when repeat caesarean or trial of labour after caesarean (VBAC) is anticipated.
Suture Techniques Used
| Technique | Description |
|---|---|
| Continuous locking (blanket) suture | Most common for first layer; provides haemostasis |
| Continuous non-locking (running) suture | Less ischaemic to tissue; increasingly preferred |
| Interrupted sutures | Used for selective reinforcement |
| Imbrication (second layer) | Buries the first layer, reinforces scar |
Decidual Inclusion / Endometrium Closure
- Whether to include or exclude the decidua/endometrium in the first layer is debated.
- Excluding the decidua (closing only myometrium) may reduce endometriosis risk at the scar and potentially improve healing — but evidence is mixed.
Peritoneum — To Close or Not?
- Non-closure of the vesico-uterine peritoneum is now widely practiced and associated with shorter operative time and less adhesion formation.
Clinical Significance: Single vs. Double Layer
| Feature | Single Layer | Double Layer |
|---|---|---|
| Operative time | Shorter | Longer |
| Blood loss | Less | More |
| Scar thickness | Thinner | Thicker |
| Uterine rupture risk | Higher | Lower |
| Isthmocele risk | Higher | Lower |
| Preferred for VBAC candidates | No | Yes |
Summary
- Double-layer closure remains the standard and preferred technique, especially for women desiring future pregnancies or VBAC.
- Single-layer closure is faster and haemostatically adequate for immediate purposes, but carries long-term scar risks.
- Suture material (typically delayed absorbable polyglycolic, e.g., Vicryl or PDS) and whether to lock the suture also influence outcomes.
Give me datails about scar niche
cesarean scar niche isthmocele
PMID: 36317541
PMID: 35985862
PMID: 39004471
PMID: 39680143
PMID: 38673465
PMID: 41485855
cesarean scar niche isthmocele ultrasound
Cesarean Scar Niche (Isthmocele / CSD)
Definition
Ultrasound Appearance


Prevalence
- Approximately 60% of women following caesarean section develop some degree of CSD (Lin et al., 2024; Stavridis et al., 2025).
- Incidence ranges widely — 20–70% — depending on the number of previous CS, diagnostic method, and threshold used.
- Prevalence increases with multiple caesarean deliveries.
Pathophysiology
Surgical / Technical Factors
- Single-layer closure (especially locking suture incorporating endometrium) — most important modifiable risk factor
- Low incision placement in the cervical rather than isthmic region
- Endometrium inclusion in suture — impairs healing, can trap endometrial tissue → adenomyosis/endometriosis at scar site
Anatomical Factors
- Uterine retroflexion — alters wound tension and healing dynamics
- Poor vascularisation at the lower uterine segment
Patient Factors
- Obesity (high BMI)
- Smoking
- Advanced maternal age
- Diabetes / poor wound healing
Measurement Parameters (on TVS / SIS)
| Parameter | Description |
|---|---|
| Depth | Perpendicular distance from base to apex of niche (≥2 mm = CSD) |
| Length | Horizontal extent of the defect |
| Width | Transverse dimension |
| Residual Myometrial Thickness (RMT) | Thickness of myometrium between base of niche and uterine serosa — most clinically critical |
- RMT < 2.5–3 mm → high risk, laparoscopic/vaginal repair preferred
- RMT ≥ 3 mm → hysteroscopic repair feasible
Clinical Presentation
| Symptom | Description |
|---|---|
| Postmenstrual spotting/brown discharge | Most characteristic — pooling of blood in the niche, delayed drainage |
| Prolonged menstruation | Mean duration ~13.4 days in symptomatic CSD vs normal |
| Early-cycle intermenstrual bleeding | Mean ~6.8 days pre-period |
| Dysmenorrhea | |
| Chronic pelvic pain / dyspareunia | |
| Secondary infertility | Impaired implantation, cervical mucus alteration |
Complications in Subsequent Pregnancy
- Cesarean scar ectopic pregnancy (CSEP) — gestational sac implants within the niche; life-threatening
- Placenta accreta spectrum (PAS) — abnormal placentation at the scar site
- Uterine rupture — especially with thin RMT
- Uterine dehiscence
Diagnosis
| Modality | Notes |
|---|---|
| Transvaginal ultrasound (TVS) | First-line; best in luteal phase or early follicular phase when fluid may fill niche |
| Saline infusion sonohysterography (SIS/SHG) | Enhances niche visibility with saline distension; more accurate sizing |
| Hysteroscopy | Directly visualises niche; allows simultaneous treatment |
| MRI | Best for soft tissue characterisation, complex cases, pre-surgical planning |
Management
Conservative / Expectant
- Asymptomatic women without desire for further fertility: observe
Hormonal
- Combined oral contraceptive pill (COCP) or levonorgestrel-IUD — reduces abnormal bleeding by suppressing endometrial activity in the niche
- Does not correct the structural defect
Surgical (for symptomatic women or those desiring fertility)
| Approach | Indication | Notes |
|---|---|---|
| Hysteroscopic resection | RMT ≥ 3 mm | Least invasive; resects niche margins to improve drainage; reduces AUB |
| Laparoscopic repair | RMT < 3 mm | Excises niche and re-sutures; increases RMT; preferred for fertility restoration |
| Vaginal repair | RMT < 3 mm | Comparable outcomes to laparoscopy; longer hospital stay |
| Robotic-assisted repair | Limited data | Promising early results |
| Combined laparoscopic-hysteroscopic | Complex cases |
Prevention
- Double-layer closure (especially excluding endometrium) reduces niche formation
- A 3-layer closure (as proposed by Bujold & Romero, Am J Obstet Gynecol 2026, PMID: 41485855) — approximating junctional myometrium (excluding endometrium) in layer 1, bulk myometrium in layer 2, superficial myometrium + serosa in layer 3 — is proposed to optimise long-term uterine healing
- Avoiding overly low incisions
- Non-locking suture technique
Key References
- Armstrong et al. "Cesarean scar niche: An evolving concern in clinical practice." Int J Gynaecol Obstet 2023 — PMID: 36317541
- Murji et al. "Cesarean scar defects and abnormal uterine bleeding: systematic review and meta-analysis." Fertil Steril 2022 — PMID: 35985862
- Stavridis et al. "Current surgical treatment of uterine isthmocele." Arch Gynecol Obstet 2025 — PMID: 39680143
- Baldini et al. "Isthmocele and Infertility." J Clin Med 2024 — PMID: 38673465
- Bujold & Romero. "Uterine closure after cesarean delivery." Am J Obstet Gynecol 2026 — PMID: 41485855
Give me details about double layer closure
double layer uterine closure cesarean hysterotomy
PMID: 36724750
PMID: 39547444
PMID: 37790067
PMID: 34131999
PMID: 41485813
single versus double layer uterine closure scar thickness rupture
double layer uterine closure cesarean section suture technique diagram
uterine closure cesarean VBAC rupture myometrial thickness
Double-Layer Uterine Closure in LSCS — Detailed Overview
Anatomy Relevant to Closure
- Endometrium / decidua — innermost mucosal layer
- Myometrium — thick muscular layer (further divided into junctional/inner and outer/bulk zones)
- Serosa (perimetrium) — outermost peritoneal layer
Step-by-Step Technique
Before Starting
- Uterus may be repaired in situ (intra-abdominal) or exteriorised (extra-abdominal); both are acceptable. Intra-abdominal repair is associated with less postoperative nausea and pain.
- Angles (lateral corners) of the incision must be secured first with a figure-of-eight or Z-suture to control bleeding from uterine vessels — before continuous suturing begins.
First Layer (Deep / Inner Layer)
- Purpose: Close the deep myometrium and decidua; achieve haemostasis.
- Suture type: Continuous running suture — either non-locking (preferred) or locking (blanket).
- Bite depth: Full-thickness myometrium, typically including the decidua/endometrium (classical approach) — though recent evidence favours excluding the endometrium (see below).
- Suture material: Delayed absorbable (e.g., polyglactin 910 / Vicryl 0 or 1, or poliglecaprone / Monocryl).
- Direction: Begins at one angle, runs to the opposite angle.
Second Layer (Superficial / Outer Layer)
- Purpose: Reinforce the first layer, imbricate (bury) it, reduce dead space, ensure serosa apposition.
- Technique: Continuous non-locking or imbricating (Lembert-type) suture through the outer myometrium and serosa.
- Effect: Covers and inverts the first suture line → smoother surface, less adhesion risk.
Locking vs. Non-Locking Suture
| Type | Mechanism | Pros | Cons |
|---|---|---|---|
| Locking (blanket) | Each pass locks the previous | Better immediate haemostasis | More ischaemic to tissue; may impair healing |
| Non-locking (running) | Simple continuous pass | Less ischaemia, better healing | Slightly less haemostatic |
To Include or Exclude the Endometrium?
Classical Double-Layer (Endometrium Inclusive)
- Both layers close full-thickness myometrium including endometrium
- Faster and simpler
- Risk: endometrial tissue entrapment → adenomyosis, defective healing, niche formation
Endometrium-Free / Exclusive Double-Layer
- First layer approximates only the junctional myometrium, deliberately excluding the endometrium (suture bites stay within the myometrium, not entering the cavity)
- Second layer closes outer myometrium + serosa
- Evidence (Antoine et al., Am J Obstet Gynecol 2026, PMID: 41485813): a 30-year retrospective series showed significant reduction in scar defects and abnormal placentation in subsequent pregnancies with this technique
Babu & Magon Technique (Modified Double-Layer)
- Designed to achieve better tissue alignment during suturing
- RCT result: niche formation 23.5% (Babu-Magon) vs 50% (standard double-layer), p=0.02
- Large niche: 2.9% vs 23.7%, p<0.01
- Supports that technique within double-layer closure also matters
Double-Layer vs. Single-Layer — Evidence Summary
| Outcome | Single-Layer | Double-Layer |
|---|---|---|
| Scar niche (isthmocele) | Higher rate | Lower rate |
| Residual myometrial thickness (RMT) | Thinner | Thicker |
| Uterine rupture risk | Higher | Lower |
| Operative time | Shorter | Slightly longer |
| Blood loss | Comparable | Comparable |
| VBAC suitability | Inferior | Superior |
The Emerging 3-Layer Closure
- Layer 1: Junctional myometrium (excluding endometrium)
- Layer 2: Bulk/outer myometrium
- Layer 3: Superficial myometrium + serosa
Suture Material Recommendation
- Polyglactin 910 (Vicryl) No. 1 or 0 — most commonly used; braided, delayed absorbable
- Poliglecaprone (Monocryl) — monofilament, less tissue drag, less ischaemia
- PDS (polydioxanone) — longer-lasting absorption, used when extra support needed
Key Principles Summary
- Secure the angles first — prevents haemorrhage from uterine vessels
- Use continuous non-locking suture in both layers — reduces ischaemia
- Exclude the endometrium where possible in the first layer — reduces niche, adenomyosis, and defective healing
- Second layer imbricates the first — reinforces scar, reduces adhesions
- Double-layer is preferred over single-layer for women who may attempt VBAC or have future pregnancies
Give me detailed info about babu and magon technique
Babu Magon uterine closure technique cesarean
Babu and Magon uterine closure technique cesarean section details steps
PMID: 22912945
PMID: 22912945
PMID: 34525487
Babu Magon uterine closure technique cesarean mattress suture
python3 -c " import xml.etree.ElementTree as ET tree = ET.parse('/home/daytona/workspace/library/xml/e8cc659483dd.xml') root = tree.getroot() # Extract all text recursively def get_text(elem, depth=0): parts = [] if elem.tag: tag = elem.tag.split('}')[-1] if '}' in elem.tag else elem.tag if tag in ['p', 'title', 'sec', 'caption', 'label']: text = ''.join(elem.itertext()).strip() if text: parts.append(f'[{tag}] {text}') for child in elem: parts.extend(get_text(child, depth+1)) return parts texts = get_text(root) for t in texts: print(t[:500]) print('---') "
Babu & Magon Uterine Closure Technique — Detailed Overview
Background & Rationale
- Cut edges may overlap rather than appose correctly
- The decidua, myometrium, and serosa may not align decidua-to-decidua, myometrium-to-myometrium, serosa-to-serosa
- There is high inter-surgeon variability
- The result: thinning of the lower uterine segment scar, predisposing to rupture, dehiscence, and niche formation
Core Concept
- Takes a deep bite (full-thickness myometrium, stopping at the myometrium-decidua junction — intentionally excluding the decidua from entrapment)
- Takes a superficial bite (encircling outer margins, sub-peritoneal fascia, and outer myometrium)
- The two bites together tighten simultaneously, achieving correct anatomical apposition of all layers in one continuous pass
Suture Material
- Polyglactin 910 (Vicryl No. 0) or Polyglycolic acid (PGA No. 0)
- Delayed absorbable, monofilament/braided
Step-by-Step Technique
Preparation
- Secure both lateral angles of the uterine incision first (as in all methods) to control uterine vessel bleeding.
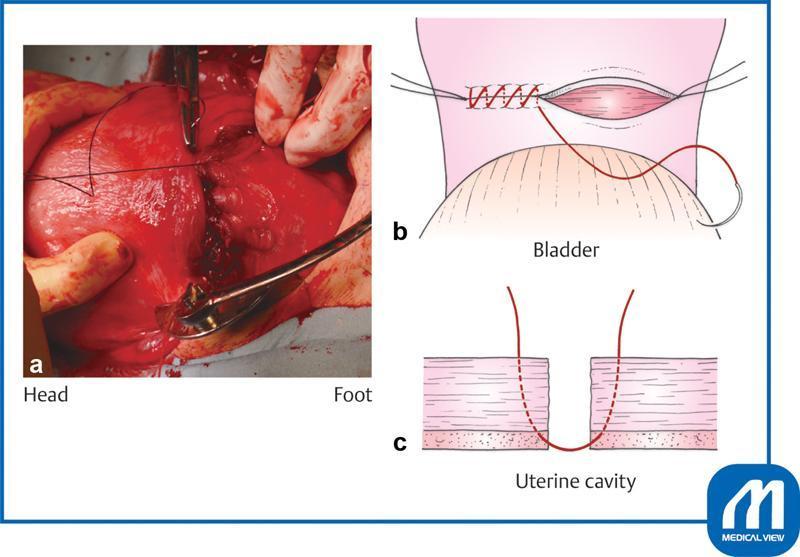
Step 1 — Deep (Full-Thickness) Bite
"A full-thickness needle bite is taken starting 1 cm away from the margin of the incision and coming out at the junction of the myometrium and decidua of the lower edge of the incision. We then enter at the junction of the myometrium and decidua of the upper edge of the incision, and come out 1 cm away from the margin of the upper edge."
- Needle enters 1 cm from the cut edge on the lower lip → traverses full thickness → exits at the myometrium-decidua junction (inner surface of lower lip)
- Needle then re-enters at the myometrium-decidua junction of the upper lip → exits 1 cm from the cut edge on the outer surface of upper lip
- Decidua does NOT get incorporated in the suture (exits and re-enters at the myometrium-decidua junction, not through the decidua itself)
- Good apposition of the deep myometrium without overlapping decidual margins
The assistant maintains traction on the previously tied suture thread throughout.
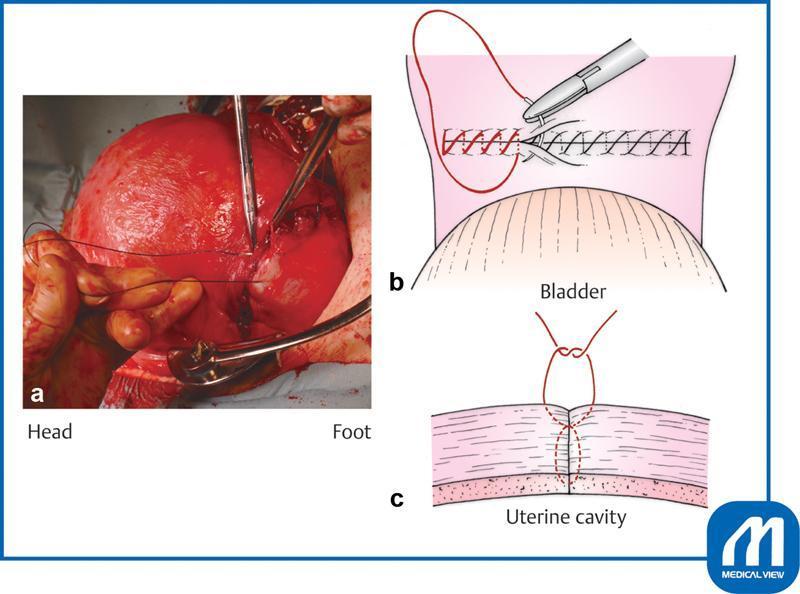
Step 2 — Superficial Bite (Without Changing Needle Direction)
"Without changing the direction of the needle, a superficial bite is taken encircling the outer margins, sub-peritoneal fascia, and outer myometrium from the lower edge and followed by the upper edge, and then the needle bite as described in Step 1 is started again."
- Immediately after Step 1, the needle takes a superficial pass around the outer margins of both incision lips — encircling the sub-peritoneal fascia and outer myometrium
- This imbrication encircles the exterior of the wound
Step 3 — Tightening the Modified Mattress
"At this stage, two loose loops are formed at the cranial and caudal ends. Surgeon will pull the caudal loop, and the cranial loop gets tightened once the assistant leaves the traction. The surgeon now tightens the caudal loop by pulling the thread. Both the deep and superficial bites are tightened, and the assistant maintains the traction of the thread. The surgeon continues the same process for the next bite."
- The deep bite and the superficial bite together form a mattress loop
- When tightened: the deep suture appoints decidua-to-decidua, myometrium-to-myometrium; the superficial suture apposes serosa-to-serosa
- Result: full-thickness correct anatomical apposition in a single continuous pass
Diagrammatic Summary
UPPER LIP LOWER LIP
___________________ ___________________
| serosa | | serosa |
| outer myometrium| | outer myometrium| ← Superficial bite
| inner myometrium| | inner myometrium| ← Deep bite exits here
| decidua | | decidua | ← NOT incorporated
|___________________| |___________________|
(Uterine cavity)
- Deep bite: enters outer surface → exits at myometrium-decidua junction → re-enters upper lip junction → exits outer surface
- Superficial bite: wraps around outer margins
- Together: a mattress that tightens all layers simultaneously
What Makes This Different
| Feature | Conventional Single-Layer | Conventional Double-Layer | Babu-Magon |
|---|---|---|---|
| No. of suture passes | 1 | 2 | 1 (but modified mattress) |
| Decidua incorporated | Yes (usually) | Yes (first layer) | No |
| Layer-specific apposition | Not guaranteed | Partial | Guaranteed |
| Inter-surgeon variability | High | Moderate | Minimal |
| Scar thinning | Higher risk | Moderate risk | Reduced |
| Niche formation | High | Moderate | Lower |
Evidence
Original Series (Babu & Magon, 2012)
- After suturing 50 cases with this technique, TVS at 6 months showed no observable thinning of the anterior lower uterine segment in any case.
- Comparison specimen: conventional double-layer LSCS (12 years prior) showed significant scar thinning at hysterectomy.
- Their own first patient (fibroid uterus, post-LSCS, repeat elective CS) had hysterectomy later → specimen showed no thinning at the closure site.
RCT Validation (Tahermanesh et al., J Obstet Gynaecol Res 2021, PMID: 34131999)
| Outcome | Babu-Magon (n=34) | Standard Double-Layer (n=38) | p-value |
|---|---|---|---|
| Any niche | 23.5% | 50% | 0.02 |
| Large niche | 2.9% | 23.7% | <0.01 |
| Closure time | No significant difference | — | NS |
| Postpartum haemorrhage | No significant difference | — | NS |
| Adjacent myometrium thickness | No significant difference | — | NS |
Advantages
- Correct anatomical apposition — decidua-to-decidua, myometrium-to-myometrium, serosa-to-serosa in every bite
- Decidua excluded — prevents endometrial entrapment, reduces adenomyosis at scar, reduces niche
- Less inter-surgeon variability — technique is self-guiding
- No scar thinning on follow-up TVS
- Single pass — comparable operative time to double-layer
- Stronger scar — capable of withstanding labour (VBAC)
Limitations
- Original study was descriptive with small numbers (n=50, no comparator)
- RCT validation (n=72) is relatively small
- No long-term RCT data on uterine rupture in subsequent labour
- Requires familiarity with the modified mattress technique
- Requires accurate identification of the myometrium-decidua junction (challenging in well-thinned lower segment)
Summary
e8cc659483dd
XML File · XML