35 yr old female came wigh pain, swelling over 1st MTP joinf for 2 days
Reading File
Finding Sources
Finding Sources
Searching PubMed
gout first metatarsophalangeal joint diagnosis management
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
I have all the information needed for a comprehensive clinical answer. Here is the full structured response:
Acute Pain & Swelling Over 1st MTP Joint - Clinical Approach
Key Diagnosis: Podagra (Acute Gouty Arthritis)
The most likely diagnosis is acute gouty arthritis (podagra) - acute inflammation of the 1st metatarsophalangeal (MTP) joint is the classic and most common presentation of gout (>50% of first attacks). However, given that this is a 35-year-old premenopausal female, gout is less common than in men and warrants careful consideration of the differential, since gout in premenopausal women is uncommon and should prompt a search for secondary causes.
Step 1: Clinical Framing (Pivotal Questions)
| Question | Answer in this case |
|---|---|
| Monoarticular vs. polyarticular? | Monoarticular (1st MTP) |
| Inflammatory vs. non-inflammatory? | Inflammatory (pain + swelling) |
| Acute vs. chronic? | Acute (2 days) |
This frames the differential as acute, inflammatory, monoarticular arthritis - a narrow and urgent category.
Differential Diagnosis
Most Likely
- Gout (Monosodium urate crystal arthropathy) - classic podagra presentation
- Pseudogout (CPPD) - calcium pyrophosphate crystals; 1st MTP less typical but possible
- Septic arthritis - must always be excluded; can be clinically identical
Also Consider
- Reactive arthritis - especially if recent GI/urogenital infection
- Psoriatic arthritis - check for skin/nail changes
- Trauma / stress fracture - history of injury
- Gonococcal arthritis - important in sexually active females
- Cellulitis / bursitis (1st MTP bursa) - periarticular mimics
Note: In men and postmenopausal women, gout is the top consideration at the 1st MTP. In a premenopausal 35-year-old woman, gout is less common (estrogen has uricosuric properties), so septic arthritis and reactive arthritis must be weighted more heavily. Gout in young women should trigger evaluation for secondary causes: renal disease, diuretic use, cyclosporine, lead nephropathy, or hereditary purine metabolism disorders. - Swanson's Family Medicine Review
History to Elicit
- Onset: Did it wake her from sleep? (Classic in gout - rapid onset over 8-12 hours)
- Previous similar attacks: Recurrence supports gout
- Diet: Purine-rich foods (red meat, shellfish, alcohol - especially beer)
- Medications: Diuretics (thiazides), low-dose aspirin, cyclosporine
- Menstrual status / OCP use
- Comorbidities: Renal disease, hypertension, metabolic syndrome
- STI risk / recent GI illness (for gonococcal/reactive arthritis)
- Skin lesions, eye symptoms (psoriatic, reactive)
Physical Examination
Expected findings in acute gout:
- Erythema, warmth, swelling, tenderness at the 1st MTP
- Skin typically tense and shiny over the joint
- Swelling may extend beyond the joint (periarticular edema) - can mimic cellulitis
- Patient unable to bear weight on the affected foot
- Check for tophi (ear helices, tendons, fingers) - uncommon in first attack
- Low-grade fever possible (up to 39.4°C) - does not exclude gout
Investigations
Mandatory
| Test | Rationale |
|---|---|
| Arthrocentesis + synovial fluid analysis | Gold standard - rules out septic arthritis, confirms crystals |
| Synovial fluid: cell count, Gram stain, culture, crystal microscopy | |
| Serum uric acid | Often normal during acute flare (suppressed by up to 2 mg/dL) - not diagnostic alone |
| CBC | Leukocytosis seen in gout and septic arthritis |
| CRP / ESR | Elevated in inflammatory arthritis |
| Renal function (eGFR, creatinine) | Gout association + guides treatment choice |
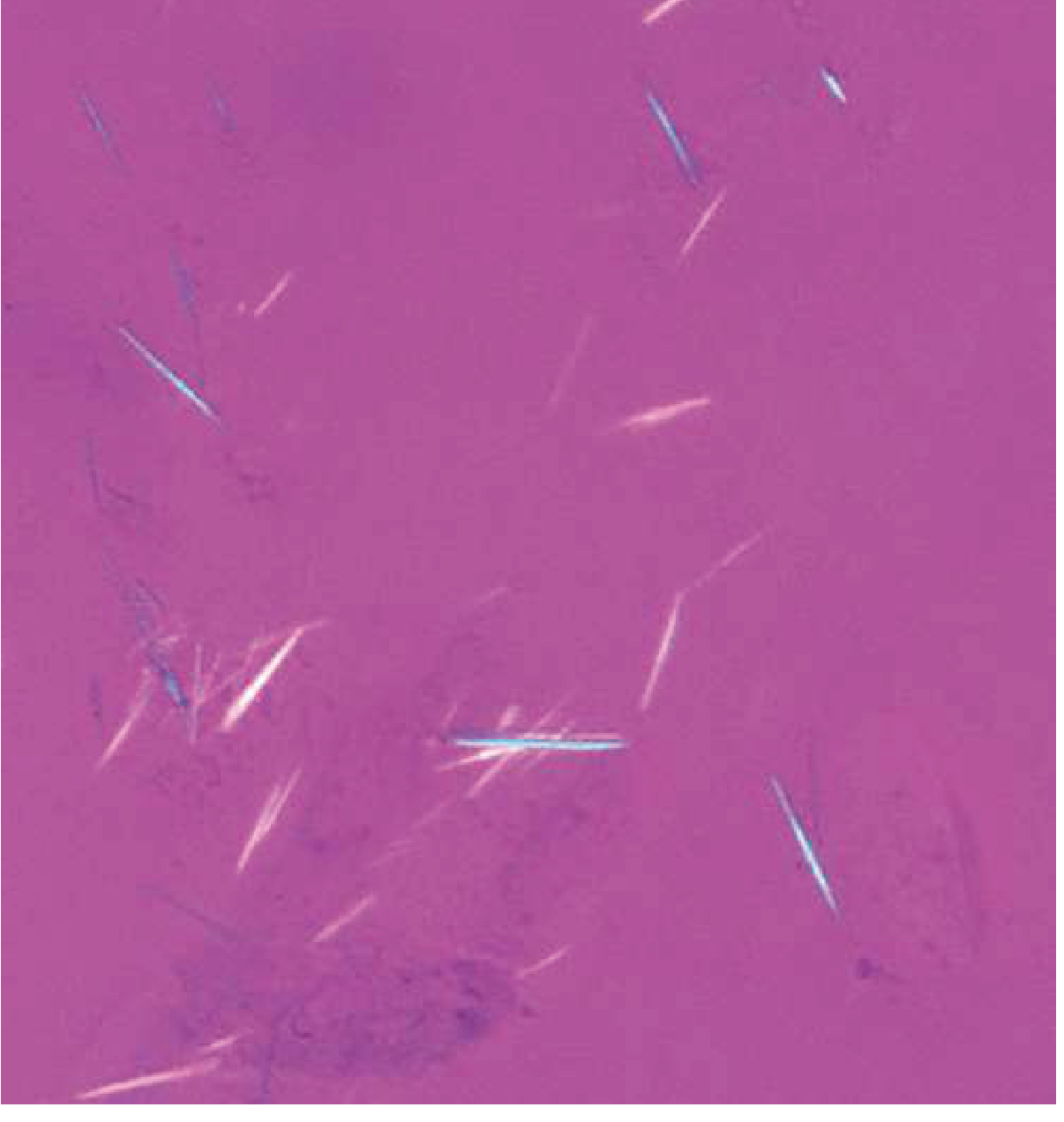
Synovial Fluid Findings
| Finding | Gout | Pseudogout | Septic Arthritis |
|---|---|---|---|
| WBC | 20,000-100,000 | 10,000-50,000 | >50,000 (often >100,000) |
| Crystal shape | Needle-shaped | Rhomboid | None |
| Birefringence | Negatively birefringent (yellow under polarizer) | Weakly positive | None |
| Culture | Negative | Negative | Positive |
The definitive diagnosis of gout requires negatively birefringent, needle-shaped monosodium urate crystals on polarized compensated microscopy. - Goldman-Cecil Medicine, 22e
Imaging
- X-ray foot: Useful mainly to exclude fracture. Acute gout shows only soft-tissue swelling. Chronic gout: punched-out periarticular erosions with overhanging edges.
- Ultrasound: Can detect monosodium urate crystals over articular cartilage - the "double contour sign" (hyperechoic line parallel to cortex). Tophi appear as "wet clumps of sugar."
- MRI not routinely required but detects soft-tissue tophi early.
Clinical Diagnosis of Gout (Without Aspiration)
If aspiration cannot be done, ≥6 of these 12 criteria support gout (Sens 87%, Spec 96%, LR+ 22):
- More than 1 prior attack
- Maximal inflammation within 1 day
- Monoarthritis
- Joint erythema
- First MTP involvement ✓ (present here)
- Unilateral MTP arthritis
- Unilateral tarsal acute arthritis
- Tophus
- Asymmetric joint swelling
- Hyperuricemia
- Bone cysts without erosion on X-ray
- Negative joint fluid culture
- Symptom to Diagnosis: An Evidence-Based Guide, 4e
Management
Acute Flare - Three Drug Options (all equally effective)
| Drug | Dose | Notes |
|---|---|---|
| NSAIDs (1st line) | Indomethacin 50 mg TID or Naproxen 500 mg BID x 5-7 days | Avoid if renal insufficiency, peptic ulcer disease, or anticoagulation |
| Colchicine | 1.2 mg at onset, then 0.6 mg 1 hour later; then 0.6 mg OD or BD x 7-10 days | Reduce dose in renal impairment; GI side effects common |
| Corticosteroids | Prednisone 30-40 mg/day x 5 days (oral) or intra-articular injection | Use when NSAIDs and colchicine are contraindicated |
- Rest the joint; apply ice packs
- Do NOT start or stop urate-lowering therapy (allopurinol, febuxostat) during an acute flare - this can prolong or worsen the attack
- Existing long-term prophylactic medications may be continued but not initiated
Long-Term / Urate-Lowering Therapy (after acute flare resolves)
- Allopurinol (xanthine oxidase inhibitor) - first-line urate-lowering agent; start at low dose after flare settles
- Febuxostat - alternative XO inhibitor
- Probenecid - uricosuric agent (avoid if renal insufficiency)
- Target serum urate <6 mg/dL (<5 mg/dL in tophaceous gout)
- Colchicine 0.6 mg daily as flare prophylaxis during ULT initiation (3-6 months)
In This Premenopausal 35-Year-Old Female
- Screen for secondary causes of gout: renal function, diuretic/medication use, hereditary purine disorders
- If confirmed gout, counsel on dietary modifications (reduce alcohol, red meat, shellfish; increase dairy, water intake)
Summary
| Details | |
|---|---|
| Most likely diagnosis | Acute gouty arthritis (podagra) |
| Can't miss | Septic arthritis (must exclude with joint aspiration) |
| Gold standard test | Synovial fluid crystal analysis (negatively birefringent needle crystals) |
| Acute treatment | NSAIDs / Colchicine / Corticosteroids |
| Special consideration | Gout uncommon in premenopausal women - investigate for secondary causes |
Sources: Goldman-Cecil Medicine 22e; Symptom to Diagnosis: An Evidence-Based Guide 4e; Rosen's Emergency Medicine; Swanson's Family Medicine Review
11 yr old boy with pain over Lt 4,5 gh toes, side Foot for 3 days, no history of trauma, on ecamination tenderness over 3,4,5 MT head, 4, 5 th toes, no wound, no signs of inflammation, no ferver, lymphadenopathy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
11 year old lateral foot pain 4th 5th metatarsal head tenderness no trauma no inflammation differential diagnosis Iselin disease
Finding Sources
Searching the Web
child 11 year tenderness 3rd 4th 5th metatarsal head lateral foot no trauma Freiberg infraction metatarsalgia differential
I now have comprehensive information. Let me compile a thorough, well-structured clinical answer.
11-Year-Old Boy - Lateral Foot Pain, 4th & 5th Toes, No Trauma
Clinical Summary
- Age: 11 years (active growing child)
- Left foot pain x 3 days
- Tenderness: 3rd, 4th, 5th MT heads + 4th, 5th toes
- No trauma, no wound, no inflammation signs, no fever, no lymphadenopathy
The clinical picture is: atraumatic, non-inflammatory, lateral forefoot pain in a growing child - this is an overuse/osteochondrosis pattern, not infectious or inflammatory.
Top Differential Diagnoses
1. Iselin's Disease (Traction Apophysitis - 5th Metatarsal Base) - MOST LIKELY
Traction apophysitis of the base of the 5th metatarsal - first described by Hans Iselin in 1912.
- Age: 9-14 years (growth plate active); peaks around 10-12 years
- Sex: More common in active boys and girls involved in running/jumping sports
- Mechanism: Repetitive traction on the apophysis at the 5th MT base by the peroneus brevis tendon and plantar fascia - essentially an overuse/growth plate stress injury (like Sever's disease of the heel, Osgood-Schlatter of the knee)
- Key exam finding: Point tenderness at the lateral base of the 5th metatarsal tuberosity; pain with resisted eversion; no erythema/warmth
- No trauma needed - cumulative microtrauma from daily walking/activity is sufficient
- Fits this child's lateral foot pattern perfectly
"Iselin disease should be kept in the differential diagnosis in an adolescent with localized fifth metatarsal base pain" - MRIMS Journal of Health Sciences
2. Freiberg's Infraction (Osteochondrosis of MT Heads) - IMPORTANT
Avascular necrosis of the metatarsal head growth centre - explains tenderness at the MT heads (3rd, 4th in this case).
- Age: 11-17 years; peak 11-15 years
- Sex: Rare exception - slightly more common in males for 3rd/4th MT; 2nd MT more common in females
- Joints affected: 2nd MT head (68%), 3rd (27%), 4th (3%), 5th (rare) - the 3rd and 4th MT head tenderness here fits
- Mechanism: Microtrauma + vascular compromise to MT head epiphysis during rapid growth; leads to progressive flattening and collapse of metatarsal head
- Symptoms: Forefoot pain, stiffness, pain at MT head on palpation, worsens with activity
- No inflammation in early stages - matches this child
Key finding: "The condition affects the second metatarsal in 68% of cases, the third metatarsal in 27%, and the fourth metatarsal in 3%" - StatPearls/NCBI
3. Stress Fracture of 4th/5th Metatarsal Shaft
- Common in children with repetitive loading (sports, long walking)
- Presents as insidious forefoot pain without clear trauma
- Tenderness along the MT shaft (diaphysis), not just the head
- X-ray may be negative in first 2 weeks (periosteal reaction appears later)
- More likely if child is very physically active or recently increased activity
4. Kohler's Disease (Navicular Osteochondrosis)
- AVN of the tarsal navicular in children aged 3-10 years
- Medial arch pain, not lateral forefoot - less likely here
- More typical in younger boys (3-7 years)
5. Sever's Disease (Calcaneal Apophysitis)
- Heel pain, not forefoot/toe pain - unlikely given location
- Mentioned for completeness as the most common pediatric foot overuse condition
6. Reactive Arthritis / Juvenile Idiopathic Arthritis
- Atraumatic, could be oligoarticular JIA or reactive arthritis post-infection
- Usually with some morning stiffness, systemic features, or prior infection history
- No inflammation/fever here makes less likely but worth asking about
- More commonly involves large joints in JIA
Summary Differential Table
| Diagnosis | Key Feature | Location | Age |
|---|---|---|---|
| Iselin's disease | 5th MT base apophysitis | 5th MT base (lateral) | 9-14 yrs |
| Freiberg's infraction | MT head AVN/osteochondrosis | 2nd-4th MT head (forefoot) | 11-17 yrs |
| Stress fracture | Shaft tenderness, activity-related | MT diaphysis | Any active child |
| Kohler's disease | Navicular AVN | Medial arch | 3-10 yrs |
| JIA / Reactive arthritis | Atraumatic joint inflammation | Variable | Any |
Investigations
1. X-Ray Foot (AP, Oblique, Lateral) - FIRST LINE
- Iselin's disease: Widening or fragmentation of the 5th MT base apophysis; the apophysis runs parallel to the shaft (unlike an avulsion fracture which is perpendicular)
- Freiberg's infraction: Flattening/sclerosis/fragmentation of the metatarsal head; later collapse
- Stress fracture: May be negative in first 2 weeks; periosteal reaction or callus later
- Important to differentiate apophysis from avulsion fracture or Jones fracture
Key radiographic tip: The normal 5th MT apophysis is longitudinally oriented (parallel to the shaft), while an avulsion fracture runs transversely (perpendicular).
2. MRI Foot (if X-ray inconclusive)
- Most sensitive for early Freiberg's (bone marrow edema before collapse)
- Shows stress fracture before periosteal reaction visible on X-ray
- Gold standard for soft tissue evaluation
3. Ultrasound
- Can show periosteal edema in early stress fracture
- Useful as bedside tool
4. Blood work (if JIA/reactive arthritis suspected)
- CBC, ESR, CRP, ANA, RF, HLA-B27
- Not primary investigation given non-inflammatory picture
Management
Iselin's Disease (5th MT Apophysitis)
- Activity modification - reduce running/jumping; relative rest
- Analgesics - paracetamol or ibuprofen for pain
- Footwear modification - well-cushioned, supportive shoes; avoid flat hard-soled footwear
- Heel cup / lateral wedge orthosis - offloads pressure from 5th MT base
- Stretching - calf/peroneal stretching if tight
- Walking boot/cast in severe cases for 3-4 weeks
- Prognosis excellent - self-limiting once growth plate fuses (typically by age 14-15)
- Surgery almost never needed
Freiberg's Infraction (Smillie Stage 1-3 - Early)
- Rest and offloading - stiff-soled shoes, metatarsal pad/dome orthosis to unload MT head
- Activity restriction from high-impact sports
- NSAIDs for pain
- Walking boot in moderate cases
- Follow-up X-rays at 4-6 weeks to monitor progression
- Surgery (debridement, dorsiflexion osteotomy) for advanced/refractory cases
Stress Fracture
- Rest and avoidance of impact activity 4-6 weeks
- Stiff-soled shoe or short-leg walking cast if severe
- Calcium/Vitamin D assessment
- Gradual return to activity
Recommended Next Steps
- X-ray left foot (AP + oblique + lateral) - mandatory first step
- Assess activity level - sports participation, recent increase in activity
- Nutritional history - calcium, vitamin D intake (stress fracture risk)
- Footwear assessment - hard-soled, ill-fitting, or flat shoes
- If X-ray inconclusive and symptoms persist → MRI foot
Key Clinical Pearl
This 11-year-old boy has the classic age, sex, and presentation for Iselin's disease (5th MT base apophysitis) combined with possible Freiberg's infraction (3rd/4th MT head tenderness) - both are osteochondroses unique to the growing skeleton, both atraumatic and non-inflammatory, and both managed conservatively. The combination of lateral forefoot and digit tenderness in a growing child without trauma or inflammation is essentially pathognomonic for growth-related bone stress conditions. X-ray is the essential next step to confirm and differentiate.
Xray is normal
Finding Sources
Searching the Web
Iselin disease normal xray early stage MRI management child 5th metatarsal apophysitis
This is a very clear and well-supported answer now. Here it is:
Normal X-Ray - What Does This Mean?
This Is Expected and Does NOT Rule Out the Diagnosis
A normal X-ray in this 11-year-old boy actually supports rather than contradicts the top diagnoses. Here's why:
How a Normal X-Ray Changes the Approach
| Condition | Why X-ray Can Be Normal | What to Do Next |
|---|---|---|
| Iselin's Disease | Early apophysitis - radiographic fragmentation/widening of apophysis appears later; X-rays may be completely normal in early disease | Clinical diagnosis sufficient; MRI if doubt |
| Stress fracture (4th/5th MT) | Periosteal reaction takes 10-21 days to appear on X-ray; early stress fractures are invisible on plain film | MRI (most sensitive) or bone scan |
| Freiberg's Infraction (early) | Bone marrow edema precedes visible flattening/sclerosis; early stages are X-ray silent | MRI shows marrow edema before X-ray changes |
"Radiographs may be negative early in the course of the disease... MRI findings precede the radiographic epiphyseal fragmentation and are thus useful in early detection." - Translational Pediatrics, 2017
"An X-ray is usually not required to diagnose Iselin disease - it may be ordered only to exclude fracture." - Nationwide Children's Hospital / CHOrtho
Revised Most Likely Diagnoses (Post-Normal X-Ray)
1. Iselin's Disease - Still Top Diagnosis
- Normal X-ray is entirely consistent with early Iselin's disease
- The diagnosis at this stage is clinical:
- Age 11, male, active child
- Lateral foot pain, no trauma
- Tenderness at 5th MT base / lateral forefoot
- No fever, no inflammation
- The apophysis at the 5th MT base fuses by ~14 years in boys - this child is still in the vulnerable window
- Normal X-ray confirms: no avulsion fracture, no Jones fracture - making Iselin's disease the confident diagnosis
2. Early Stress Fracture(s) - Second Consideration
- 3-day history is too short for periosteal reaction to appear on X-ray
- Tenderness at multiple MT heads (3rd, 4th, 5th) could suggest multiple stress reactions - especially in a child with sudden increase in activity
- A normal X-ray with this presentation warrants MRI
3. Early Freiberg's Infraction - Still Possible
- Smillie Stage 1 (earliest) is X-ray silent
- Tenderness specifically at MT heads supports this
- MRI would show bone marrow edema at the MT head
Next Step Algorithm
Normal X-ray + Atraumatic lateral forefoot pain in 11-yr-old
↓
Clinical diagnosis of Iselin's Disease
(if 5th MT base tender, active child, no red flags)
↓
START conservative treatment now
+ Review at 4 weeks
↓
If NO improvement at 4 weeks
or if 3rd/4th MT head tenderness prominent
↓
MRI Foot
(detect marrow edema, stress fracture,
early Freiberg's, muscle/tendon injury)
Immediate Management - Start Now
Conservative Treatment (suitable while awaiting further workup)
| Intervention | Detail |
|---|---|
| Activity modification | Reduce/stop running, jumping, sports; walking is allowed |
| Analgesics | Paracetamol (15 mg/kg 4-6 hourly) or Ibuprofen (10 mg/kg TDS with food) for 5-7 days |
| Ice packs | 15 min, 3-4x/day over lateral foot for first 48-72 hrs |
| Footwear | Change to well-cushioned, supportive, closed shoes; avoid flip-flops and flat hard soles |
| Lateral wedge orthosis | Offloads 5th MT base pressure - simple insole modification |
| Rest from sport | Minimum 2-4 weeks relative rest |
| Walking boot | If pain is severe enough to cause limping - short-leg walking boot for 3-4 weeks |
What NOT to Do
- Do not dismiss as "growing pains" and send home without follow-up
- Do not apply heat in the acute phase
- Do not continue high-impact sports activity
Red Flags - When to Escalate Urgently
Order MRI foot if any of the following:
- No improvement after 4 weeks of conservative treatment
- Symptoms worsening despite rest
- Pain at rest or at night (red flag for bone tumor/infection)
- Child unable to bear weight at all
- Bilateral foot pain (consider systemic cause - JIA, metabolic bone disease)
Key Take-Home Points
- Normal X-ray does not rule out Iselin's disease or early stress fracture - this is expected in the first 2 weeks
- The X-ray's main value here was to exclude fracture and Jones fracture - which it has done
- Clinical diagnosis of Iselin's disease is valid in this age group with this presentation
- Start conservative management now - most cases resolve within 4-8 weeks
- If no improvement at 4 weeks, proceed to MRI to evaluate for stress fracture, Freiberg's infraction, or ligamentous injury
This is a shared conversation. Sign in to Orris to start your own chat.