Meconium apsiration syndrom
Reading File
Finding Sources
Searching PubMed
"meconium aspiration syndrome"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from three authoritative textbooks. Here is a thorough overview of Meconium Aspiration Syndrome (MAS):
Meconium Aspiration Syndrome (MAS)
Definition & Epidemiology
MAS is a clinical diagnosis defined by three criteria occurring together:
- Delivery through meconium-stained amniotic fluid (MSAF)
- Respiratory distress
- Characteristic chest X-ray appearance
- MSAF occurs in 4–22% of all deliveries, more commonly in post-term pregnancies
- MAS complicates approximately 1–2% of deliveries with MSAF
- Most common in post-mature (post-term) infants; unusual before 36 weeks due to incomplete maturation of the intestinal myenteric plexus
- Approximately 30% of affected infants require mechanical ventilation
— Grainger & Allison's Diagnostic Radiology; Creasy & Resnik's Maternal-Fetal Medicine
Pathophysiology
Meconium aspiration causes disease through multiple concurrent mechanisms, not just airway obstruction as was previously believed:
| Mechanism | Effect |
|---|---|
| Mechanical obstruction | Thick meconium migrates to distal airways → complete/partial obstruction → "ball-valve" effect → alternating atelectasis and overinflation |
| Chemical pneumonitis | Direct inflammatory injury to the pulmonary parenchyma |
| Surfactant inactivation | Meconium inactivates surfactant, worsening compliance |
| Pulmonary hypertension (PPHN) | Chronic fetal hypoxia → increased muscle in distal pulmonary arterial vessels → persistent pulmonary hypertension of the newborn |
Key pathophysiological link: Fetal hypoxia (especially chronic, third-trimester) → intestinal hyperperistalsis → in-utero meconium passage → fetal breathing aspirates meconium-laden amniotic fluid into the tracheobronchial system.
— Barash Clinical Anesthesia, 9e; Creasy & Resnik's Maternal-Fetal Medicine
Chest X-Ray Findings
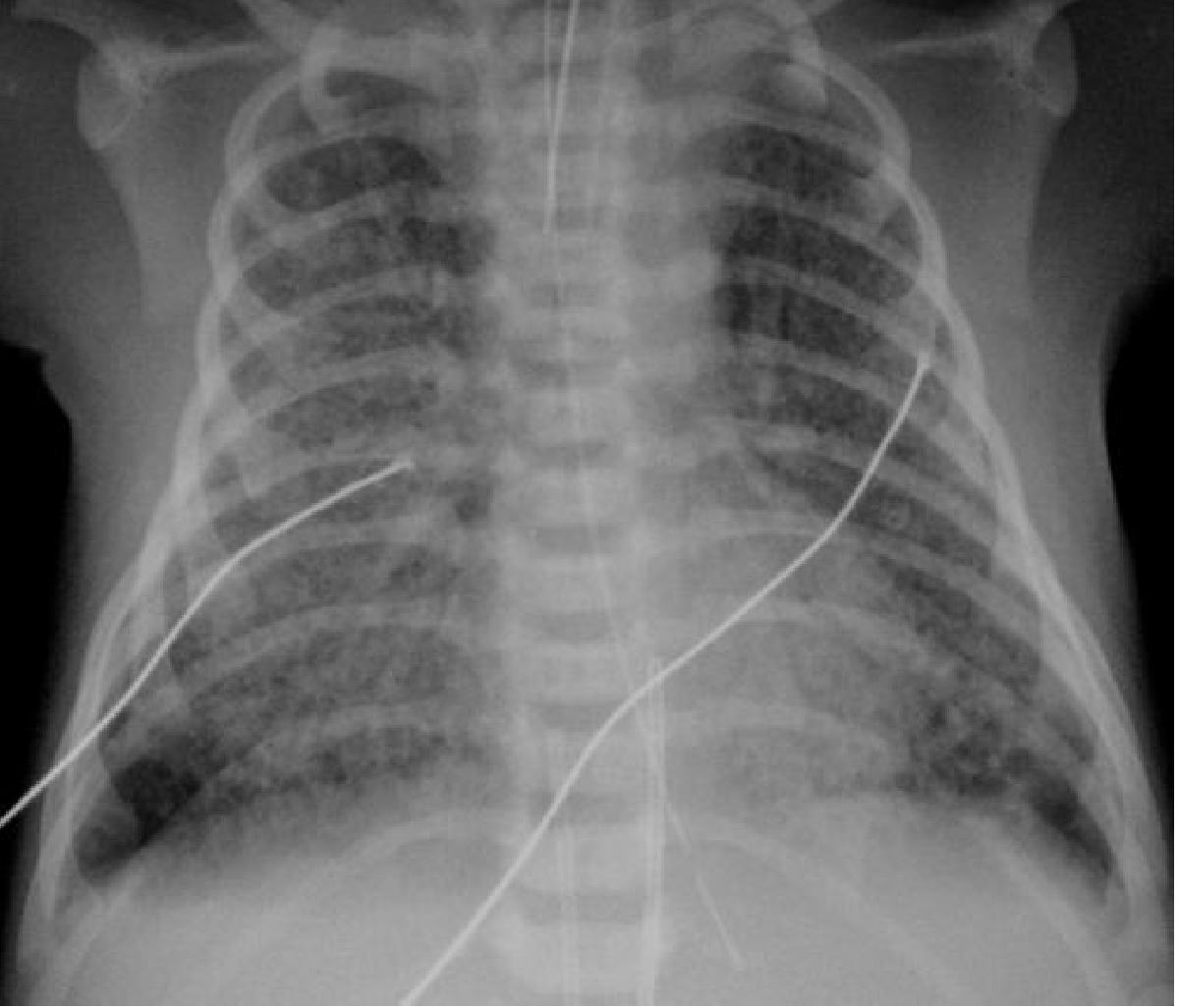
CXR in a 42-week infant with MAS: bilateral hyperinflation, asymmetrical coarse opacification, and small left pleural effusion — Grainger & Allison's Diagnostic Radiology
Characteristic radiographic features:
- Bilateral hyperinflation
- Asymmetrical coarse/patchy opacification (segmental atelectasis alternating with air-trapping)
- Air leaks (pneumothorax, pneumomediastinum) — common complication
- Small pleural effusions may be present
- Chemical pneumonitis pattern
Clinical Severity
Severity ranges from mild to life-threatening. Hallmarks of severe disease:
- Need for positive-pressure ventilation
- Presence of pulmonary hypertension (PPHN)
Complications of severe MAS:
- Air leak syndromes (pneumothorax)
- Chronic lung disease
- Developmental delay
- Death
Prevention
Antenatal
- Induction of labor at 41 weeks — systematic reviews show fewer MAS cases and fewer cesarean sections vs. expectant management
- Amnioinfusion to dilute thick meconium — did NOT reduce MAS incidence or perinatal morbidity in well-monitored settings
Peripartum Suctioning — Evolving Guidelines
This area has undergone major paradigm shifts:
| Era | Practice |
|---|---|
| 1970s–2005 | Aggressive oropharyngeal + tracheal suctioning for all infants |
| 2004 onward | Large RCT showed no benefit of intrapartum suctioning → removed from guidelines |
| 2000 (Wiswell) | No benefit of elective intubation/suctioning in vigorous infants → abandoned |
| 2015 (ILCOR/AAP) | Two small RCTs: no benefit even in depressed infants |
| Current | Routine endotracheal suctioning is NOT recommended for vigorous OR depressed infants after MSAF delivery |
Delaying positive-pressure ventilation (PPV) to suction may cause more harm than benefit. Skilled personnel for airway management should attend all expected depressed deliveries.
— Creasy & Resnik's Maternal-Fetal Medicine
Treatment
Management targets hypoxemia and respiratory failure:
Respiratory Support
- Positive-pressure ventilation for respiratory failure
- If vigorous and crying at birth → no suctioning needed; if depressed → intubate and suction if meconium present, then proceed with PPV if bradycardia develops
Pulmonary Hypertension (PPHN)
Selective pulmonary vasodilators:
- Inhaled nitric oxide (iNO) — first-line; improves oxygenation and allows less injurious ventilation
- Sildenafil — oral PDE-5 inhibitor
- Bosentan — endothelin receptor antagonist
Surfactant
- Exogenous surfactant — early administration is a useful adjunct (counteracts surfactant inactivation by meconium)
Salvage Therapy
- ECMO (Extracorporeal Membrane Oxygenation) — for infants failing conventional treatment
- VA-ECMO: cannulae via internal jugular vein + common carotid artery
- VV-ECMO: double-lumen catheter via internal jugular vein
- Antibiotics and steroids — selectively used; no demonstrated effectiveness in trials
— Grainger & Allison's Diagnostic Radiology; Creasy & Resnik's Maternal-Fetal Medicine
Key Takeaways
- MAS is distinct from simply having MSAF — requires respiratory distress + CXR findings
- Pathophysiology is multifactorial: obstruction + inflammation + surfactant inactivation + PPHN
- Routine tracheal suctioning is no longer recommended regardless of infant vigor — a major departure from historical practice
- iNO + surfactant are the cornerstones of treatment; ECMO is salvage
- Prognosis has improved dramatically with modern management
Persistent pulmonary hypertension
Finding Sources
Searching PubMed
"persistent pulmonary hypertension of the newborn"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from three authoritative sources. Here is a complete overview:
Persistent Pulmonary Hypertension of the Newborn (PPHN)
Definition & Epidemiology
PPHN — sometimes called persistent fetal circulation — is the failure of the normal postnatal fall in pulmonary vascular resistance (PVR), resulting in sustained right-to-left shunting through fetal channels (ductus arteriosus, foramen ovale).
- Incidence: ~2/1000 live births in term and late preterm infants
- Presents within the first 12–24 hours of birth
- One of the leading causes of neonatal morbidity and mortality
— Creasy & Resnik's Maternal-Fetal Medicine; Harriet Lane Handbook, 23e
Normal Fetal-to-Neonatal Transition
At birth, an 8- to 10-fold increase in pulmonary blood flow is achieved through:
- Effective clearance of lung fluid
- Lung aeration and oxygenation
- Ventilation
- Cord clamping → rise in systemic vascular resistance (SVR)
- Reversal of flow across the ductus arteriosus and foramen ovale
PPHN occurs when this transition fails.
The graph below shows normal mean pulmonary artery pressure declining over the first 72 hours of life:
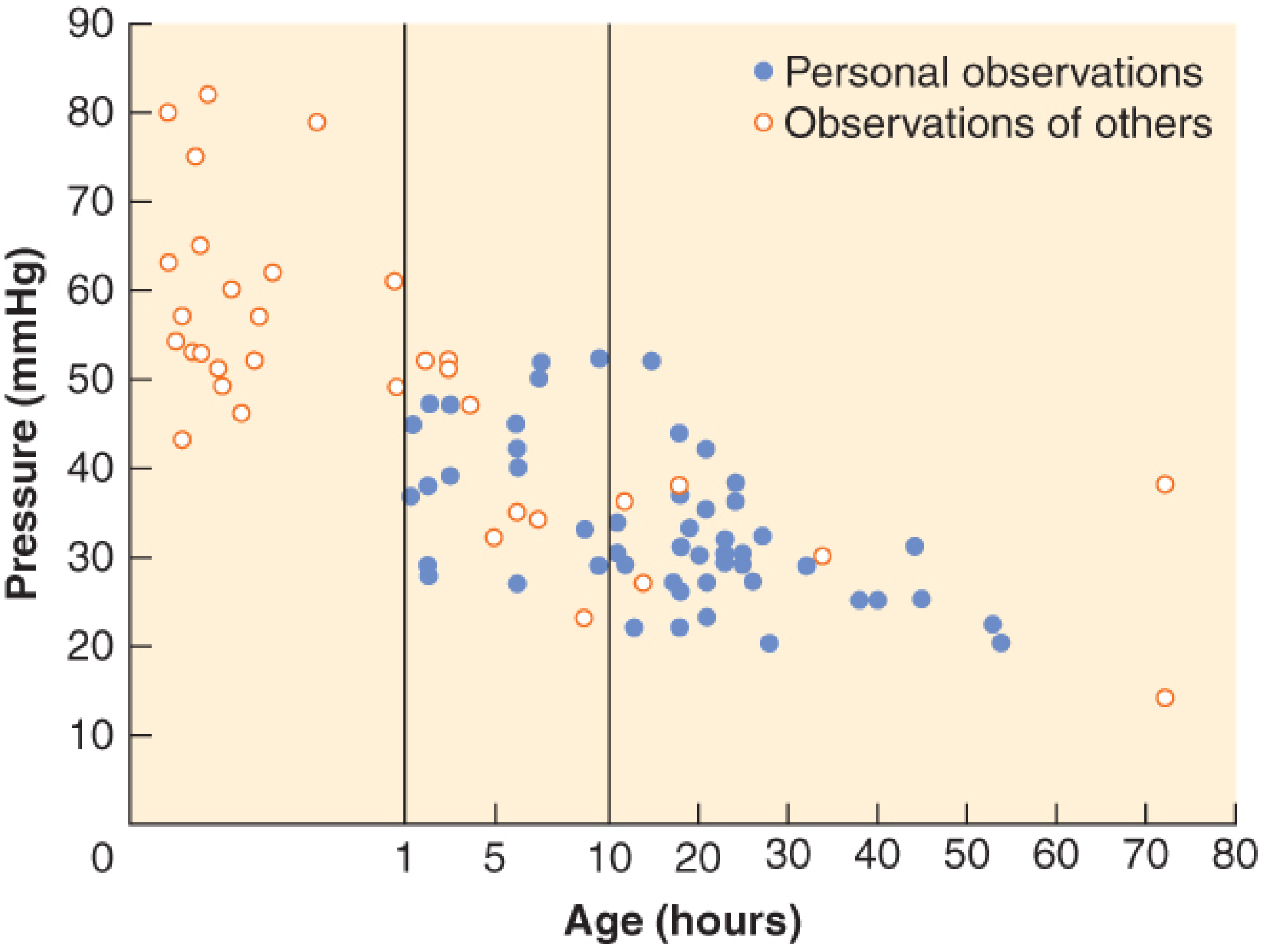
Normal mean PA pressure in 85 term infants: rapid decline from near-systemic levels at birth to normal (~25–30 mmHg) by 24–48 hours — Barash Clinical Anesthesia, 9e
Causes & Classification
PPHN arises from two core mechanisms: pulmonary arteriolar vasoconstriction and vascular structural remodeling.
| Category | Examples |
|---|---|
| Idiopathic | Abnormally remodeled pulmonary vasculature (no identifiable cause) |
| Lung parenchymal disease | Meconium aspiration syndrome (MAS), pneumonia/sepsis |
| Abnormal birth transition | Transient tachypnea of the newborn (TTN), RDS, perinatal asphyxia |
| Congenital lung malformation | Congenital diaphragmatic hernia (CDH), pulmonary hypoplasia |
Additional risk factors:
- Maternal SSRI or NSAID use (in utero ductal constriction)
- Maternal smoking, uncontrolled diabetes, asthma
- Cesarean section delivery, polycythemia, low Apgar scores
Pathophysiology
Elevated PVR → both the ductus arteriosus and foramen ovale remain patent → right-to-left shunting bypasses the pulmonary circulation → severe hypoxemia
Key features:
- Hypoxemia out of proportion to other clinical/radiologic findings
- Normal or elevated PaCO₂ (lungs not being perfused)
- The pulmonary circulation is exquisitely sensitive to hypoxia, acidosis, and inflammatory mediators, all of which perpetuate vasoconstriction
Diagnosis
Clinical Features
- Severe hypoxemia (PaO₂ <35–45 mmHg in 100% O₂)
- Pre-/postductal SpO₂ gradient ≥7–15 mmHg is significant (right hand preductal vs. lower extremity postductal)
- Structurally normal heart on echo — right-to-left shunt at foramen ovale and/or ductus arteriosus
Key Diagnostic Step
Distinguish from cyanotic congenital heart disease:
- Hyperoxia test: PaO₂ fails to rise significantly with 100% O₂ in both cyanotic CHD and PPHN
- Echocardiography is definitive — confirms structurally normal heart and shows direction of shunting
Treatment
General Principles
Treatment targets the underlying etiology while managing hypoxemia and reducing PVR.
1. Optimize Oxygenation
- Supplemental oxygen — a potent pulmonary vasodilator
- Target preductal O₂ saturations (to reduce lung injury from overdistention)
- Correct polycythemia, hypoglycemia, metabolic disturbances
2. Minimize Pulmonary Vasoconstriction
- Minimal handling — noxious stimuli spike PVR; sedation (and occasionally paralysis in intubated infants) is important
- Avoid severe hyperventilation — hypocarbia (PCO₂ <30 mmHg) causes myocardial ischemia and decreased cerebral blood flow; can also lead to barotrauma
- Consider high-frequency oscillatory ventilation to limit lung injury
3. Maintain Systemic Blood Pressure
- Reversal of right-to-left shunt requires adequate SVR
- Volume expanders and/or inotropes (e.g., dopamine, dobutamine)
- Note: dobutamine may reduce SVR in normotensive patients — can paradoxically worsen R→L shunting but offloads the RV
Target: PaO₂ 60–100 mmHg, normocapnia
4. Pulmonary Vasodilator Therapy
| Agent | Mechanism | Notes |
|---|---|---|
| Inhaled nitric oxide (iNO) | Selective pulmonary vasodilator via cGMP pathway | Only FDA-approved drug for PPHN; start at 20 ppm; no additional benefit >40 ppm; monitor methemoglobin (<4%) and NO₂ (<1–2 ppm); indicated when OI ≥15 |
| Sildenafil | PDE-5 inhibitor → ↑cGMP → pulmonary vasodilation | Used as adjuvant; oral/IV |
| Bosentan | Endothelin receptor antagonist | Adjuvant; longer-term use |
| Prostacyclin (epoprostenol) | Vasodilator normally produced by lung vessels | Adjuvant |
| Milrinone | PDE-3 inhibitor; inotrope + vasodilator | Adjuvant; improves RV function |
OI formula: OI = (Mean Airway Pressure × FiO₂ × 100) / PaO₂
5. ECMO (Salvage)
Criteria for ECMO consideration:
- OI >40 sustained for >3 hours, OR
- A-aO₂ gradient ≥610 for 8 hours
- Severe cardiovascular instability unresponsive to therapy
ECMO candidacy requirements: Weight >2000 g, gestation >34 weeks
- Obtain head ultrasound (exclude IVH) and consider EEG before initiating
- iNO has not reduced the need for ECMO in CDH specifically
Prognosis
- Outcome varies directly with ability to reduce PVR and address the underlying cause
- Ischemic encephalopathy is a major negative prognostic factor
- Survivors of severe PPHN are at risk for neurodevelopmental impairment and chronic lung disease
Summary Flowchart
PPHN suspected (severe hypoxemia, pre/postductal gradient)
↓
Echo → rule out cyanotic CHD
↓
Treat underlying cause + optimize ventilation
↓
iNO (OI ≥15) ± adjuvant vasodilators
↓
OI >40 for >3h → ECMO evaluation
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Barash Clinical Anesthesia, 9e; Harriet Lane Handbook, 23e
Screening in infant of diabetic mother
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Excellent — I have rich content from the Harriet Lane Handbook and Creasy & Resnik. Here is the complete answer:
Infant of a Diabetic Mother (IDM) — Screening
Overview of Complications
IDM complications are a direct function of maternal glycemic control. The underlying driver is fetal hyperinsulinism — chronic maternal hyperglycemia → excess fetal glucose → fetal pancreatic β-cell hypertrophy → hyperinsulinemia.
| Complication | Mechanism |
|---|---|
| Macrosomia / LGA | Excess insulin → anabolic growth, increased fat deposition |
| Hypoglycemia | Hyperinsulinism persists postnatally after glucose supply from mother is cut |
| Polycythemia | Chronic fetal hypoxia → ↑ erythropoietin → ↑ RBC mass |
| Hypocalcemia / hypomagnesemia | Electrolyte disturbances (mechanism not fully understood) |
| Delayed lung maturation | Insulin antagonizes cortisol-induced surfactant synthesis → ↑ risk of RDS at any given gestational age |
| Delayed neurological maturation | Decreased tone → delayed feeding competence |
| Congenital heart disease | Hypertrophic cardiomyopathy; septal defects |
| Skeletal malformations | Sacral agenesis, femoral hypoplasia (pathognomonic association) |
| Transient tachypnea of the newborn (TTN) | Delayed lung fluid clearance |
— Harriet Lane Handbook 23e; Creasy & Resnik's Maternal-Fetal Medicine
Screening Protocol
1. Hypoglycemia Screening (Most Critical)
IDM ≥34 weeks is a high-risk group that mandates routine glucose screening per AAP/Adamkin guidelines.
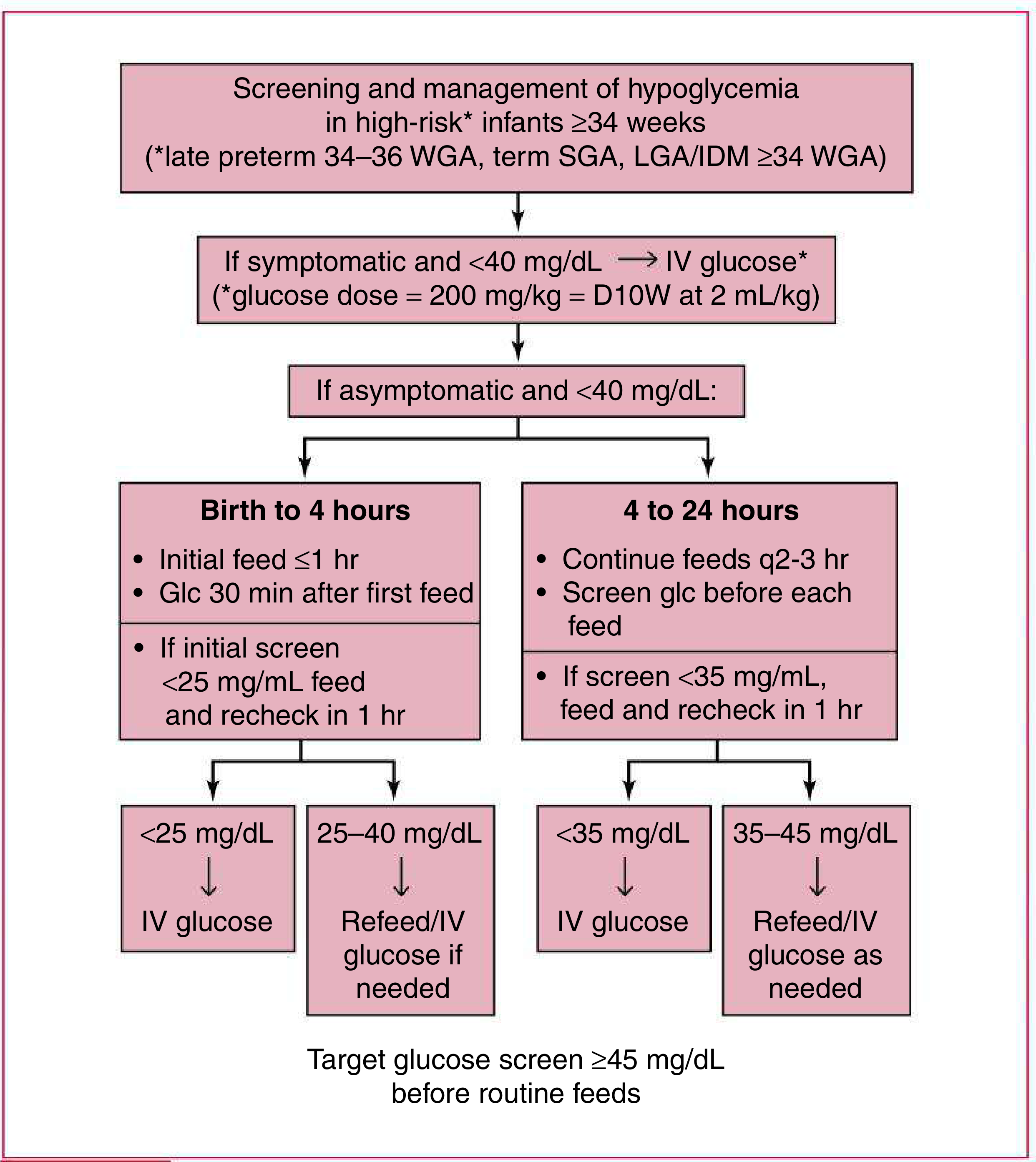
Key thresholds:
| Time | Action threshold | Response |
|---|---|---|
| Symptomatic, any age | <40 mg/dL | IV glucose immediately (200 mg/kg = D10W at 2 mL/kg) |
| Birth to 4 hours (asymptomatic) | Screen 30 min after first feed; if <25 mg/dL → IV glucose; if 25–40 mg/dL → refeed and recheck | Target ≥45 mg/dL before routine feeds |
| 4–24 hours (asymptomatic) | Screen before each feed q2–3h; if <35 mg/dL → IV glucose; if 35–45 mg/dL → refeed as needed | Continue until target ≥45 mg/dL |
Initial feed should occur within ≤1 hour of birth for IDM infants.
2. Polycythemia Screening
- Check hematocrit/hemoglobin — polycythemia defined as venous Hct >65%
- Polycythemia → hyperviscosity → risk of stroke, NEC, renal vein thrombosis, PPHN
3. Electrolyte Screening
- Serum calcium (hypocalcemia: <7 mg/dL total or <4 mg/dL ionized)
- Serum magnesium (hypomagnesemia often accompanies hypocalcemia; correcting Mg is prerequisite to correcting Ca)
- Typically checked at 24–48 hours of life
4. Cardiac Screening
- Echocardiogram if clinically indicated — IDM has increased risk of:
- Hypertrophic cardiomyopathy (asymmetric septal hypertrophy)
- Structural CHD (TGA, VSD)
- Critical CHD screening: Pre- and postductal pulse oximetry before discharge (standard for all newborns, especially important in IDM)
5. Respiratory Assessment
- IDM has delayed surfactant maturation → monitor for RDS symptoms, especially in late preterm IDM
- Lung maturity at a given gestational age is less than in non-IDM infants — avoid elective delivery <39 weeks without documented lung maturity
6. Bilirubin Monitoring
- Polycythemia → increased RBC breakdown → hyperbilirubinemia
- Transcutaneous or serum bilirubin monitoring per standard risk assessment protocols
7. Standard Newborn Screens (All Infants)
- Newborn metabolic screen (PKU, congenital hypothyroid, etc.) — ≥24h after feeding, within 72h
- Hearing screen
- Red reflex examination
- Hepatitis B vaccine
Summary Screening Checklist for IDM
| Parameter | Timing | Threshold/Action |
|---|---|---|
| Blood glucose | 30 min after 1st feed, then pre-feeds q2–3h until 24h | Screen <40 mg/dL symptomatic → IV; target ≥45 mg/dL |
| Hematocrit | 4–6 hours of life | >65% venous → evaluate for partial exchange transfusion |
| Serum Ca²⁺ / Mg²⁺ | 24–48 hours | Ca <7 mg/dL or ionized <4 mg/dL → supplement |
| Bilirubin | Clinical monitoring ± TcB | Per standard nomogram |
| Echo | If symptomatic or clinically indicated | HCM, structural CHD |
| Pulse oximetry | Pre-discharge | Critical CHD screen |
| CXR / respiratory | If tachypnea/distress | RDS, TTN |
The key principle: most IDM complications are transient and resolve without long-term sequelae if identified and managed promptly. Neonatal morbidity is proportional to the degree of maternal glycemic control during pregnancy.
— Harriet Lane Handbook, 23e; Creasy & Resnik's Maternal-Fetal Medicine; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.