Hyperthyroidism
Reading File
Finding Sources
Searching PubMed
hyperthyroidism management
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of hyperthyroidism drawn from Harrison's Principles of Internal Medicine (22e), Robbins & Kumar Basic Pathology, Textbook of Family Medicine, and the Tietz Textbook of Laboratory Medicine.
Hyperthyroidism
Definition
Hyperthyroidism refers to increased thyroid hormone biosynthesis and secretion from the thyroid gland itself, producing a hypermetabolic state. The term thyrotoxicosis is broader - it describes any state of excess thyroid hormone, including from exogenous sources or tissue destruction. Diagnosis rests on a suppressed TSH (<0.1 mIU/L) with elevated free T4 and/or free T3. - Textbook of Family Medicine 9e
Causes
| Cause | Notes |
|---|---|
| Graves' disease | Most common; autoimmune (TSH receptor antibody) |
| Toxic multinodular goiter (TMNG / Plummer disease) | Autonomous nodular function |
| Toxic (autonomous) adenoma | Single hyperfunctioning nodule |
| Destructive thyroiditis | Subacute, silent, postpartum - transient hormone leak |
| TSH-secreting pituitary adenoma | Secondary/central hyperthyroidism - rare |
| Factitious / iatrogenic | Exogenous thyroid hormone ingestion |
| Excess iodine | Jod-Basedow phenomenon |
| hCG stimulation | Gestational thyrotoxicosis, hydatidiform mole |
- Textbook of Family Medicine 9e, Table 35-5
Graves' Disease - Pathogenesis
Graves' disease is the most common cause of endogenous hyperthyroidism, with a peak incidence between 20-40 years and women affected up to 7 times more often than men (estimated 1.5-2% of US women).
The key mechanism involves TSH receptor antibodies (TRAb), IgG autoantibodies that bind the TSH receptor and mimic TSH action, causing unregulated T4 and T3 production. Pituitary feedback is overridden, so TSH falls dramatically - often <0.01 mIU/L or unmeasurable.
-
Genetic susceptibility: increased in monozygotic twins; associated with specific HLA alleles and CTLA4 polymorphisms.
-
Stimulating and blocking TRAbs can coexist in the same patient, explaining intermittent hypothyroid episodes.
-
Ophthalmopathy: TSH receptors on orbital fibroblasts/fat cells are activated by CD4+ T cells, increasing extracellular matrix deposition in the retroorbital space.
-
Dermopathy (pretibial myxedema): glycosaminoglycan deposition + lymphocyte infiltration in the skin, most commonly over the shins.
-
Robbins & Kumar Basic Pathology
Morphology (Histology)
- Symmetric gland enlargement from diffuse follicular cell hypertrophy and hyperplasia
- Follicular cells tall, crowded; form small papillae projecting into lumen (no fibrovascular cores - unlike papillary carcinoma)
- Pale, scalloped colloid
- Lymphoid infiltrates (predominantly T cells) with germinal centers
Clinical Features
Symptoms Common to All Thyrotoxicosis
- Tachycardia, wide pulse pressure, systolic hypertension
- Warm, moist skin; heat intolerance
- Weight loss despite increased appetite
- Tremor, anxiety, hyperactivity, insomnia
- Diarrhea
- Menstrual irregularities, reduced fertility; gynecomastia in men
- Anemia, relative neutropenia, lymphocytosis
Graves'-Specific Features (the "triad")
- Diffuse goiter - bruit may be audible over the gland
- Ophthalmopathy - exophthalmos (proptosis), lid lag, stare, periorbital edema, diplopia; scored by the EUGOGO system
- Dermopathy - present in <5%; nodular, indurated, pink/purple plaques on shins ("orange skin" texture). Acropachy (clubbing) occurs in <1%.
Radioiodine treatment can worsen ophthalmopathy (especially in smokers). Antithyroid drugs and surgery do not adversely affect eye disease. - Harrison's 22e
Laboratory Diagnosis
The diagnostic algorithm from Harrison's is shown below:
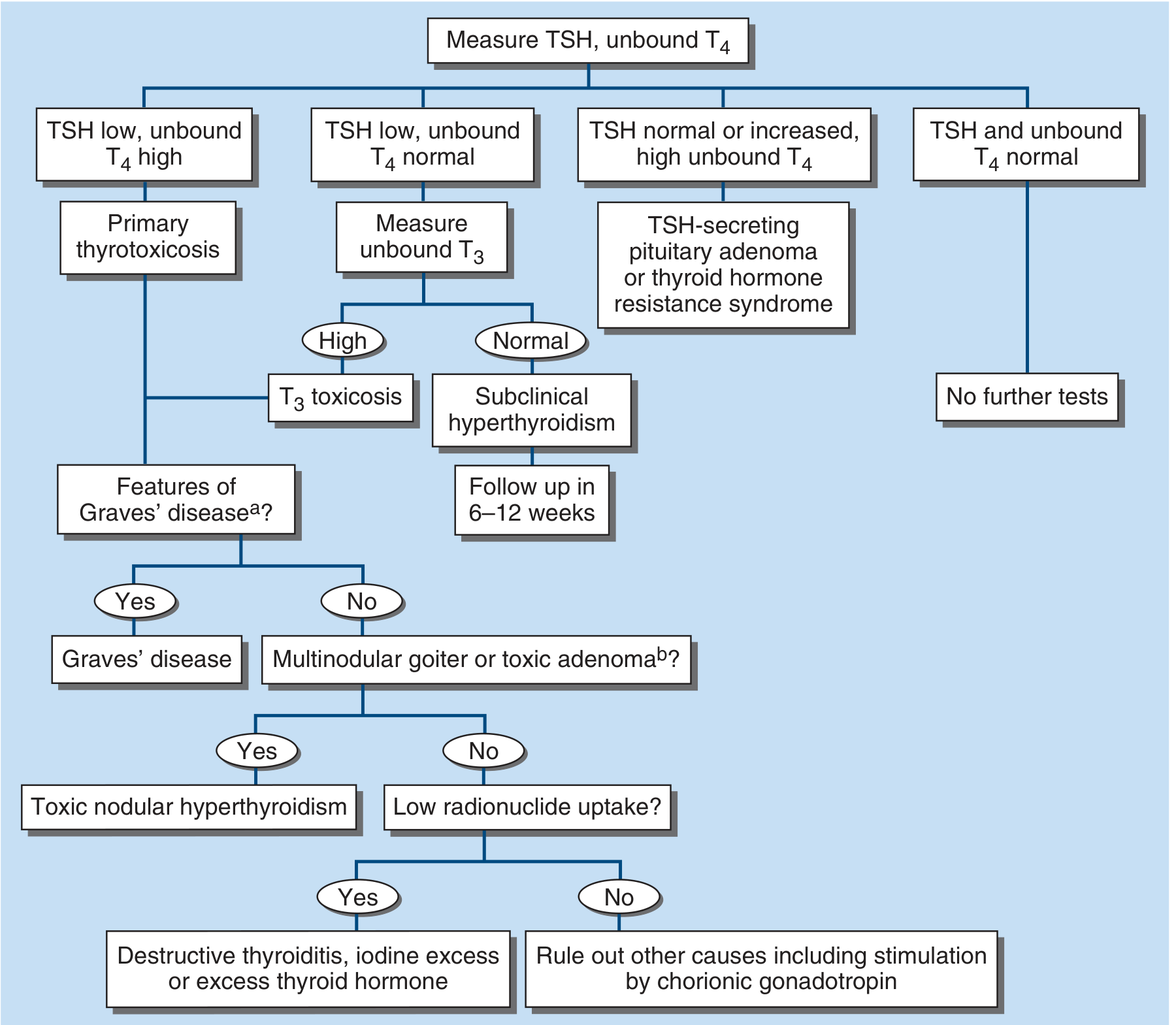
Key lab points:
- TSH is the most sensitive biomarker - suppressed in all primary hyperthyroidism
- Free T4 is elevated in most cases; if normal, check free T3 (T3 toxicosis occurs in 2-5%)
- T4 toxicosis (elevated T4, normal T3) is seen with iodine excess
- TRAb (3rd-generation assay): confirms Graves' disease with high sensitivity and specificity
- If TSH is not suppressed but T4 is high: suspect TSH-secreting pituitary adenoma or thyroid hormone resistance
- Additional: elevated bilirubin, liver enzymes, ferritin; microcytic anemia; thrombocytopenia may all occur
Radionuclide scan (⁹⁹mTc, ¹²³I, or ¹³¹I) distinguishes diffuse high uptake (Graves') from low uptake (thyroiditis, factitious) or focal uptake (toxic adenoma/TMNG). Color-flow Doppler ultrasound is an alternative that avoids radioactivity. - Harrison's 22e, Tietz 7e
Treatment
Three Main Options for Graves' Disease
| Option | Notes |
|---|---|
| Antithyroid drugs (thionamides) | Preferred initial therapy in Europe, Latin America, Japan |
| Radioiodine (¹³¹I) | More often first-line in North America; contraindicated in pregnancy |
| Thyroidectomy | For large goiters, non-remitting disease, young patients |
"No single approach is optimal and patients may require multiple treatments to achieve remission." - Harrison's 22e
Antithyroid Drugs (Thionamides)
All inhibit thyroid peroxidase (TPO), reducing iodide oxidation and organification, thereby blocking thyroid hormone synthesis. They also reduce thyroid antibody levels and enhance spontaneous remission rates.
- Methimazole (MMI): preferred agent (half-life 6 h, once-daily dosing possible); initial dose 10-20 mg every 12 h
- Carbimazole: prodrug of methimazole; not available in the US
- Propylthiouracil (PTU): shorter half-life (90 min), requires dosing every 6-8 h at 100-200 mg per dose. PTU also inhibits peripheral T4 → T3 conversion. FDA-restricted indications: first trimester of pregnancy, thyroid storm, and minor MMI side effects. Hepatotoxicity risk requires LFT monitoring.
Regimens:
- Titration: gradually reduce dose as euthyroidism is restored (preferred - minimizes drug exposure)
- Block-replace: high-dose antithyroid drug + levothyroxine supplementation to prevent hypothyroidism
Review thyroid function 4-6 weeks after starting treatment. - Harrison's 22e
Side effects (applies to all thionamides):
- Minor: rash, urticaria, arthralgia, fever (~5%)
- Major: agranulocytosis (~0.3%) - warn patients to report sore throat/fever urgently
- PTU-specific: hepatotoxicity (rare but severe)
Radioiodine (¹³¹I)
- Ablates thyroid tissue; most patients develop hypothyroidism and require lifelong levothyroxine
- Absolutely contraindicated in pregnancy or possibility of pregnancy
- Pre-treatment with antithyroid drugs for at least 1 month reduces risk of post-radioiodine thyrotoxic crisis
- Can worsen Graves' ophthalmopathy (particularly in smokers) - Tietz 7e
- Preferred for toxic multinodular goiter and toxic adenoma
Beta-Blockers
Used for symptomatic relief (tachycardia, tremor, anxiety) while awaiting antithyroid drug effect. Do not affect thyroid hormone levels. - Frameworks for Internal Medicine
Thyroid Storm (Thyrotoxic Crisis)
A rare but life-threatening exacerbation of thyrotoxicosis with multiorgan dysfunction. Mortality can reach 75% if unrecognized.
- Occurs in 1-5% of hospitalized thyrotoxic patients
- Usually precipitates on a background of unrecognized Graves' disease
- Precipitants: infection, surgery, trauma, DKA, labor, cardiac disease, radioiodine
- Clinical diagnosis - not defined by TSH/T4/T3 levels
Clinical Features
- Hyperpyrexia (>38.9°C / 102°F)
- Tachycardia disproportionate to fever
- GI dysfunction: nausea, vomiting, diarrhea, jaundice
- CNS dysfunction: severe irritability, confusion, coma
- Pronounced decompensation of organ systems
Treatment
- Beta-blockers (high-dose propranolol or esmolol IV)
- PTU (preferred over MMI in storm - blocks T4→T3 conversion) in high doses
- Iodine (Lugol solution or SSKI) - given only after antithyroid drug loading, to block T4 release
- Corticosteroids (dexamethasone) - reduce T4→T3 conversion, treat possible adrenal insufficiency
- Antipyretics (paracetamol - NOT aspirin, which displaces T4 from binding proteins)
- Aggressive IV fluid resuscitation
- Identify and treat precipitating cause
- Lithium or sodium ipodate for refractory cases
- Manage in medical ICU with endocrinology consultation
- Textbook of Family Medicine 9e, Goodman & Gilman's Pharmacology, Tietz 7e
Special Situations
Pregnancy
- PTU is preferred in the first trimester (MMI associated with embryopathy - choanal atresia, aplasia cutis)
- Switch to MMI after first trimester (lower hepatotoxicity risk)
- ¹³¹I is absolutely contraindicated
- Neonatal Graves' can occur from placental transfer of TRAb
- hCG-mediated gestational thyrotoxicosis is transient and usually does not require treatment
Subclinical Hyperthyroidism
- Suppressed TSH with normal free T4 and T3
- Follow-up in 6-12 weeks; treat if persistent, elderly, at risk for atrial fibrillation or osteoporosis
Cardiovascular Risks
Cardiovascular complications - particularly atrial fibrillation and heart failure - represent the highest potential for morbidity and mortality in thyrotoxicosis. A 2024 systematic review (PMID 38902995) specifically characterized the clinical course of atrioventricular conduction blocks in hyperthyroidism.
Sources: Harrison's Principles of Internal Medicine 22e | Robbins & Kumar Basic Pathology | Textbook of Family Medicine 9e | Tietz Textbook of Laboratory Medicine 7e | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.