I now have all the material needed. Here is the comprehensive 10-mark exam answer:
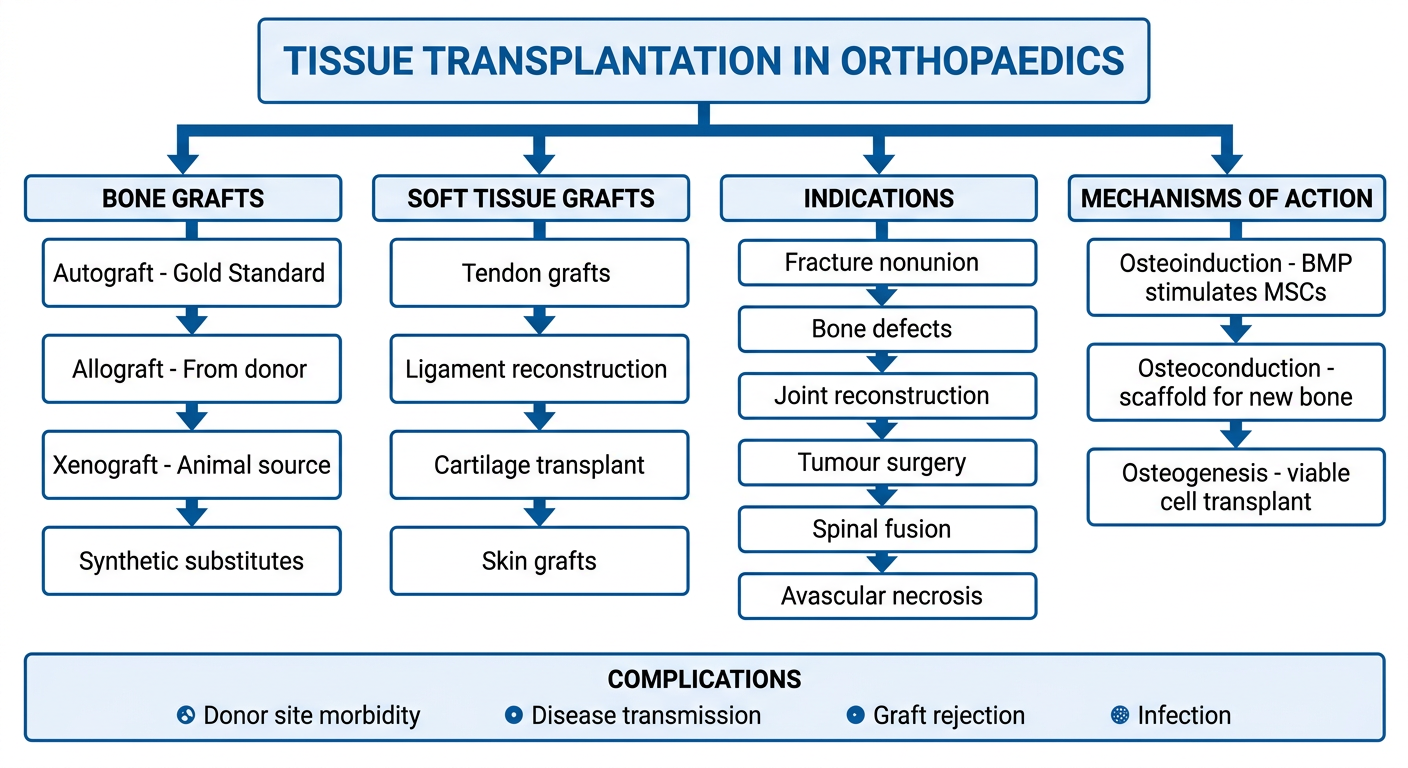
Role of Tissue Transplantation in Orthopaedics
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Rockwood and Green's Fractures in Adults 10th Ed 2025
Flowchart
Introduction
Tissue transplantation in orthopaedics refers to the transfer of biological material - bone, cartilage, tendon, ligament, or skin - from one site to another to restore structural integrity, promote healing, or reconstruct damaged tissues. Bone is a remarkable tissue capable of regenerating new bone (rather than scar) under ideal conditions, but certain defects require exogenous graft material to achieve healing. - Rockwood and Green's, p. 2460
I. Types of Tissue Transplanted
A. Bone Grafts
Bone is the most commonly transplanted tissue in orthopaedics. It is classified based on the source:
| Type | Source | Properties |
|---|
| Autograft | Same individual | Osteoinductive + Osteoconductive + Osteogenic; Gold standard |
| Allograft | Same species (donor) | Osteoconductive + Osteoinductive (variable); risk of disease transmission |
| Xenograft | Different species (animal) | Mainly osteoconductive; limited clinical use |
| Synthetic substitutes | Laboratory-made | Osteoconductive scaffold only |
(Table adapted from Campbell's Operative Orthopaedics 15th Ed, Table 58.6)
II. Mechanisms of Bone Graft Action
Three fundamental mechanisms explain how grafts promote bone healing:
1. Osteoinduction
The recruitment, proliferation, and differentiation of host mesenchymal stem cells (MSCs) into chondroblasts and osteoblasts. Bone Morphogenic Protein (BMP) - discovered by Urist in 1965 - is the principal mediator. Other factors include FGF, PDGF, and VEGF. - Rockwood and Green's, p. 2467-2468
2. Osteoconduction
The graft acts as a passive scaffold along which host blood vessels and new bone tissue grow. All graft types (autograft, allograft, ceramics) have this property.
3. Osteogenesis
Direct formation of new bone by viable cells transplanted within the graft itself. Only autograft and fresh allograft possess this property, as they contain living osteoprogenitor cells. The cancellous autograft offers the largest surface area and highest number of pluripotent cells. - Rockwood and Green's, p. 2486
III. Specific Graft Types and Their Properties
A. Autogenous Bone Graft (Gold Standard)
Autograft is the transfer of bone from a site of abundance (donor) to a site of need within the same individual. It possesses all three properties (osteoinduction, osteoconduction, osteogenesis) and carries:
- No risk of histoincompatibility or disease transmission
- Both cancellous and cortical forms available
- Cancellous graft: rapid incorporation due to large surface area and high cell content
- Cortical graft (e.g., tricortical iliac crest): provides structural support but slower incorporation
Donor sites: Iliac crest (19-26 cc anteriorly, 34 cc posteriorly), fibula, tibia, RIA (Reamer-Irrigator-Aspirator) for intramedullary harvest.
Limitations:
- Donor site morbidity (~20.6% minor, ~8.6% major complication rates)
- Limited quantity available
- Added operative time and blood loss
Rockwood and Green's, p. 2486-2503
B. Allograft
Allograft uses bone from a human donor (cadaveric or living). Processed forms include:
- Fresh-frozen: best biological activity
- Freeze-dried: structural support, less osteoinductive activity
- Irradiated (electron beam/gamma): sterilised, reduced osteoinductive properties
- Demineralized Bone Matrix (DBM): decalcified allograft retaining BMP; supplied as putty, gel, paste, or strips
Advantages: No donor site morbidity; available in large volumes; can be used structurally (bulk allograft for massive defects after tumour resection).
Disadvantages:
- Disease transmission risk (HIV, Hepatitis B and C documented)
- Variable osteoinductive strength
- Immune-mediated graft rejection
- Cannot guarantee complete sterilisation despite rigorous donor screening
Campbell's Operative Orthopaedics 15th Ed, p. 3276-3278
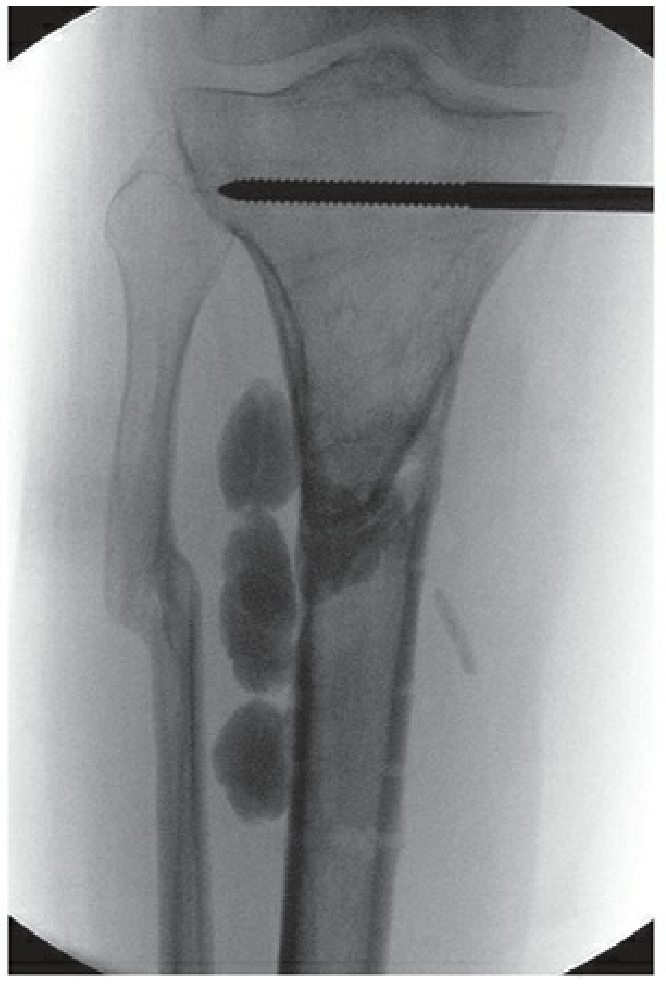
X-ray - Infected Tibial Nonunion treated with tricortical iliac crest autograft (Rockwood & Green):
Intraoperative fluoroscopy showing RIA (Reamer-Irrigator-Aspirator) instrument being used to harvest autograft from the femoral canal - demonstrating a modern technique for obtaining large volumes of bone graft with reduced morbidity.
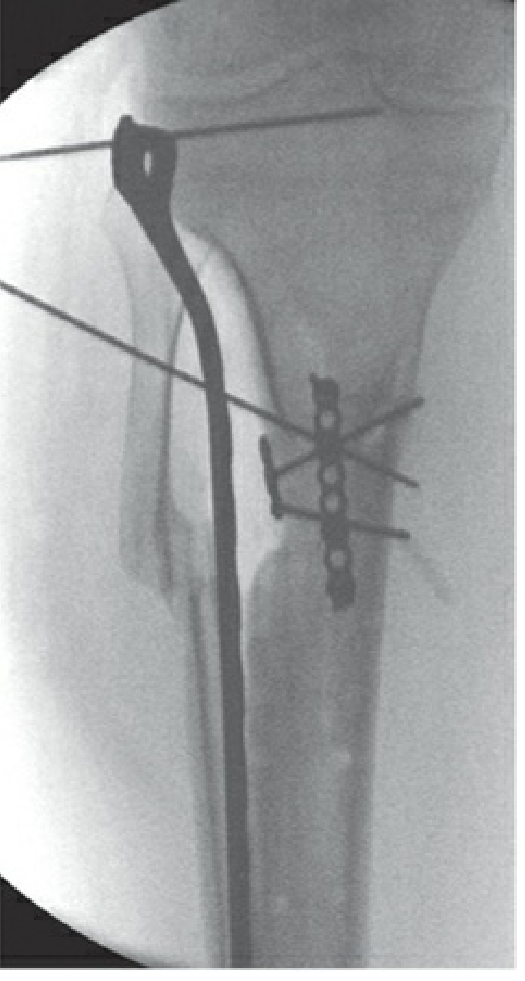
Post-operative radiograph showing combined intramedullary nail and plate fixation following bone graft reconstruction of a critical tibial defect.
IV. Bone Graft Substitutes
When autograft supply is insufficient, substitutes are employed. Laurencin's classification divides them into five categories:
| Category | Example | Key Property |
|---|
| Allograft-based | DBM (Demineralized Bone Matrix) | Osteoconductive + osteoinductive |
| Factor-based | rhBMP-2 | Osteoinductive (approved for spinal fusion, open tibial fractures) |
| Cell-based | Mesenchymal stem cells, bone marrow aspirate | Osteogenic |
| Ceramic-based | Hydroxyapatite, tricalcium phosphate, calcium sulfate | Osteoconductive scaffold |
| Polymer-based | Biodegradable polymers | Osteoconductive scaffold |
rhBMP-2: Currently the only approved recombinant growth factor for clinical use; induces enchondral bone formation. Complications include inflammatory reactions, ectopic bone formation, and possible tumour risk. Contraindicated in children and pregnant women. - Campbell's, p. 1050-1068
Calcium Phosphate: Three forms - hydroxyapatite (slowest resorption, >10 years), tricalcium phosphate (6-18 months), calcium phosphate cement (highest compressive strength). RCTs show calcium phosphate cement equals or exceeds autograft outcomes in tibial plateau, distal radius, and calcaneus fractures. - Rockwood and Green's, p. 2558-2564
Calcium Sulfate: Rapidly resorbed (6-12 weeks); used since 1892 as an osteoconductive material; provides less biomechanical stability but resorbs quickly to allow bone in-growth.
V. Soft Tissue Transplantation
Beyond bone, several soft tissues are transplanted in orthopaedics:
1. Tendon Grafts
- Used in tendon reconstruction (e.g., Achilles tendon repair, flexor tendon injuries)
- Sources: palmaris longus, plantaris, hamstring tendons, toe extensors
- Allograft tendons used when autograft is insufficient
2. Ligament Reconstruction
- ACL (Anterior Cruciate Ligament) reconstruction is the most common orthopaedic ligament transplant
- Graft options: patellar tendon (bone-tendon-bone), hamstring tendons, quadriceps tendon (autografts) or Achilles/tibialis anterior allograft
3. Cartilage Transplantation
- Osteochondral autograft transfer (OATS/mosaicplasty): cylindrical plugs transferred from non-weight-bearing areas to repair chondral defects
- Fresh osteochondral allograft: for large defects (>4 cm²), especially in post-traumatic or tumour reconstruction
- Autologous Chondrocyte Implantation (ACI): cell-based technique; cartilage cells harvested, expanded in culture, then reimplanted
4. Free Soft Tissue and Vascularized Bone Transfer
- Composite tissue transplantation (free flaps) for soft tissue cover over exposed bone and joints
- Vascularized fibula graft: gold standard for large segmental bone defects (>6 cm), avascular necrosis of femoral head, and tumour reconstruction
VI. Indications for Tissue Transplantation in Orthopaedics
- Fracture nonunion - autograft or DBM to stimulate healing at non-healing fracture sites
- Critical bone defects - post-traumatic, post-infective, or post-tumour resection defects requiring structural graft
- Spinal fusion - ICBG (iliac crest bone graft) remains standard; BMP-2 as alternative
- Avascular necrosis - vascularized fibula for femoral head AVN
- Tumour surgery (limb salvage) - massive structural allografts or vascularised grafts after wide resection
- Ligament/tendon reconstruction - ACL, PCL, rotator cuff, Achilles
- Articular cartilage defects - OATS, ACI, osteochondral allografts
- Infected nonunion / osteomyelitis - after debridement, bone grafting for defect reconstruction
- Congenital pseudarthrosis - vascularized fibula in difficult cases
VII. Complications
| Complication | Details |
|---|
| Donor site morbidity | Pain, haematoma, nerve injury, fracture, hernia (autograft) |
| Disease transmission | HIV, Hepatitis B and C (allograft); risk despite screening |
| Graft failure/resorption | Especially in large structural allografts |
| Infection | Bacterial contamination of graft |
| Immune rejection | More relevant with fresh allografts |
| Ectopic bone formation | Especially with BMP-based substitutes |
| Limited supply | Constrains autograft volume |
| Variable osteoinductive activity | DBM products vary widely by donor, processing, and carrier |
Summary Points for Exam
- Autograft = gold standard (all three properties: osteoinduction + osteoconduction + osteogenesis)
- Three mechanisms: Osteoinduction (BMP, growth factors), Osteoconduction (scaffold), Osteogenesis (viable cells)
- Allograft - available in large amounts but risk of disease transmission and variable activity
- DBM - demineralized allograft retaining osteoinductive proteins; available as putty/gel/strips
- rhBMP-2 - only approved recombinant BMP; used for spinal fusion and open tibial fractures
- Calcium phosphate - purely osteoconductive ceramic; hydroxyapatite most durable
- Vascularized fibula - for large segmental defects and AVN of femoral head
- ACL reconstruction - commonest ligament transplant; patellar tendon or hamstring autograft preferred
References: Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 58 (Bone Graft and Substitutes); Rockwood and Green's Fractures in Adults 10th Ed 2025, Chapter 3 (Bone Grafting and Enhancement of Fracture Healing)