Shoulder girdle notes acc to bdc
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
I now have sufficient information to compile comprehensive BDC-style notes on the shoulder girdle. Let me present these notes.
Shoulder Girdle - Notes (BDC Style)
Note: BD Chaurasia's Human Anatomy is not available in this library. These notes are compiled from Gray's Anatomy for Students and Imaging Anatomy (Vol. 3), following the BDC chapter structure and format.
INTRODUCTION
The shoulder girdle (pectoral girdle) connects the upper limb to the axial skeleton. It consists of two bones:
- Clavicle (collar bone) - anteriorly
- Scapula (shoulder blade) - posteriorly
It is incomplete posteriorly (no bony connection to vertebral column) - this allows greater mobility of the upper limb compared to the lower limb.
1. CLAVICLE
General Features
- A long bone with a double curve (S-shaped in superior view)
- First bone to ossify (5-6 weeks of intrauterine life) but last to complete ossification (~27 years)
- Lies horizontally at the root of the neck
- Has no medullary cavity - ossifies in membrane (intramembranous ossification)
- Narrowest at its middle third - commonest site of fracture
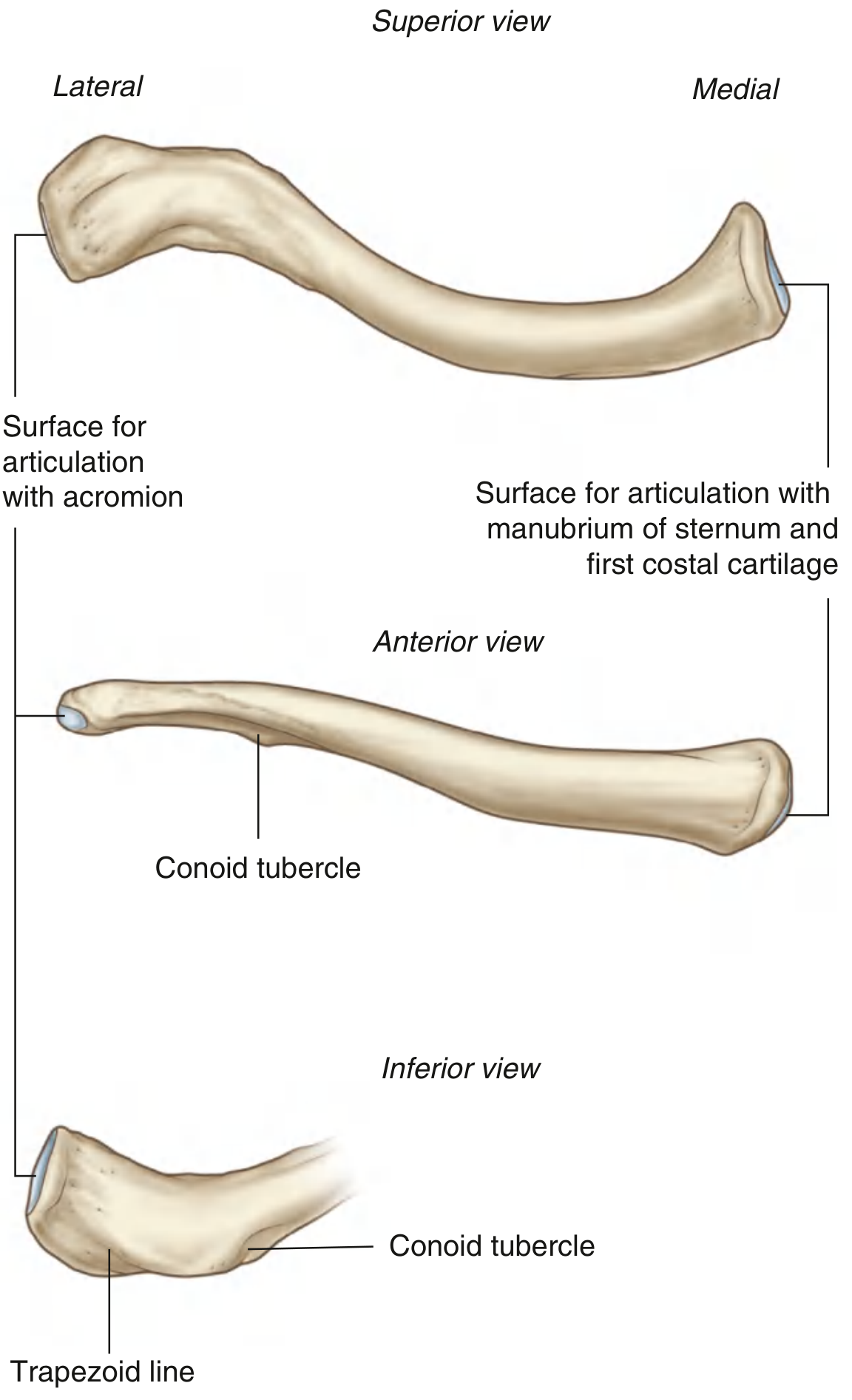
Ends
| Feature | Medial (Sternal) End | Lateral (Acromial) End |
|---|---|---|
| Shape | Enlarged, rounded | Flattened |
| Articulation | Manubrium sterni + 1st costal cartilage (SC joint) | Acromion of scapula (AC joint) |
| Curve | Convex anteriorly | Concave anteriorly |
Surfaces
- Superior surface: smooth, subcutaneous
- Inferior surface: marked by:
- Rhomboid fossa (costoclavicular ligament attachment) - medially
- Conoid tubercle (conoid ligament attachment)
- Trapezoid line/ridge (trapezoid ligament attachment) - laterally
Muscular Attachments
| Muscle | Attachment |
|---|---|
| Sternocleidomastoid | Medial 1/3 - superior surface |
| Pectoralis major (clavicular head) | Medial 2/3 - anterior surface |
| Deltoid | Lateral 1/3 - anterior surface |
| Trapezius | Lateral 1/3 - posterior surface |
| Subclavius | Middle 1/3 - inferior surface (subclavian groove) |
Ligamentous Attachments
- Costoclavicular ligament - to rhomboid fossa (resists lateral, superior and anterior displacement)
- Conoid ligament - medial part of CC ligament, from base of coracoid to conoid tubercle
- Trapezoid ligament - lateral part of CC ligament, from coracoid to trapezoid line
- Interclavicular ligament - runs between both medial ends across the sternal notch
2. SCAPULA
General Features
- A flat, triangular bone lying on the posterior thoracic wall over ribs 2-7
- Has 3 angles, 3 borders, 2 surfaces, and 3 processes
Angles
| Angle | Features |
|---|---|
| Superior angle | Thin, covered by trapezius; levator scapulae inserts |
| Inferior angle | Thick, covered by latissimus dorsi; moves laterally during abduction |
| Lateral angle | Broadened into the glenoid cavity for glenohumeral joint |
Borders
| Border | Description |
|---|---|
| Superior border | Shortest; has suprascapular notch (suprascapular nerve passes through) |
| Medial (vertebral) border | Parallel to vertebral column |
| Lateral (axillary) border | Thickest; from glenoid to inferior angle |
Surfaces
- Costal (anterior/subscapular) surface: concave; subscapular fossa; subscapularis muscle arises from it
- Posterior surface: divided by the spine into:
- Supraspinous fossa (above) - supraspinatus arises
- Infraspinous fossa (below) - infraspinatus arises
Processes
- Spine of scapula - triangular ridge across posterior surface; continuous laterally with acromion
- Trapezius inserts above; deltoid arises below
- Acromion - flat process projecting laterally; articulates with clavicle (AC joint); tip is subcutaneous
- Coracoid process - "bent finger" process projecting anterolaterally; important muscular and ligamentous attachment
Key Attachments on Coracoid Process
- Pectoralis minor - medial aspect
- Short head of biceps brachii - tip
- Coracobrachialis - tip
- Conoid ligament - base
- Trapezoid ligament - base
- Coracoacromial ligament - lateral border
Glenoid Cavity
- Shallow, comma-shaped; articulates with head of humerus
- Supraglenoid tubercle (superior) - long head of biceps brachii attaches
- Infraglenoid tubercle (inferior) - long head of triceps brachii attaches
Ossification of Scapula
- 8 or more centers:
- 1 large center for the body (appears ~8th week in utero)
- 2-3 centers for coracoid (central at 3 months; base at 8-10 years)
- Multiple centers for acromion (failure of fusion = os acromiale)
- Centers for medial border and inferior angle
3. JOINTS OF THE SHOULDER GIRDLE
A. Sternoclavicular (SC) Joint
- Only true joint connecting upper limb to axial skeleton
- Type: Synovial, saddle joint (functionally acts like a ball-and-socket)
- Has an articular disc (fibrocartilaginous)
- Ligaments: SC capsule, interclavicular ligament, costoclavicular ligament
- Posterior SC capsule = most important stabilizer (resists anterior and posterior displacement)
- Movements: elevation/depression, protraction/retraction, rotation of clavicle
B. Acromioclavicular (AC) Joint
- Type: Synovial, plane joint
- Has an articular disc (variable, often incomplete)
- Main stabilizers:
- AC ligament - resists horizontal translation
- Coracoclavicular (CC) ligament - primary vertical stabilizer (conoid + trapezoid parts)
- Movements: gliding, rotation of clavicle on acromion
C. Scapulothoracic Joint (Physiological joint)
- Not a true synovial joint - scapula glides on serratus anterior over thorax
- Movements coupled with SC and AC joints:
- Protraction (forward): serratus anterior + pectoralis minor
- Retraction (backward): trapezius + rhomboids
- Elevation: trapezius (upper) + levator scapulae
- Depression: trapezius (lower) + serratus anterior (lower)
- Upward rotation (glenoid faces up): serratus anterior + upper trapezius
4. MUSCLES OF THE SHOULDER GIRDLE
Axial (Stabilizer) Muscles - Connect Scapula to Axial Skeleton
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Trapezius | Occipital bone, nuchal ligament, C7-T12 spinous processes | Lateral clavicle, acromion, spine of scapula | Upper: elevates; Middle: retracts; Lower: depresses scapula | Accessory (CN XI) + C3,C4 |
| Serratus anterior | Lateral aspects of ribs 1-10 | Anterior surface of medial border of scapula | Protracts + upward rotation; holds scapula against chest wall | Long thoracic nerve (C5,6,7) |
| Rhomboid major | T2-T5 spinous processes | Medial border of scapula | Retracts + elevates scapula | Dorsal scapular nerve (C4,5) |
| Rhomboid minor | C6-C7 spinous processes, ligamentum nuchae | Medial border at level of scapular spine | Retracts + elevates scapula | Dorsal scapular nerve (C4,5) |
| Levator scapulae | Transverse processes C1-C4 | Superior angle of scapula | Elevates + medially rotates scapula | Dorsal scapular nerve + C3,4 |
| Pectoralis minor | 3rd-5th ribs (anterior) | Medial coracoid process | Depresses + protracts scapula | Medial pectoral nerve |
| Subclavius | 1st costochondral junction | Inferior groove of clavicle | Depresses clavicle; protects SC joint | Nerve to subclavius (C5,6) |
5. SCAPULAR MOVEMENTS AND RHYTHM
Scapulohumeral Rhythm
- For every 3° of shoulder abduction: 2° at glenohumeral + 1° at scapulothoracic
- Total 180° abduction = 120° glenohumeral + 60° scapulothoracic
- The clavicle acts as a strut, transmitting forces and enabling scapular movement
Scapular Winging
- Loss of serratus anterior function (long thoracic nerve palsy) - medial border protrudes posteriorly
- Visible on pushing against a wall
6. CLINICAL POINTS (BDC High-Yield)
| Topic | Key Point |
|---|---|
| Fracture clavicle | Most common at junction of middle and outer 1/3; medial fragment pulled up by SCM, lateral fragment pulled down by weight of arm |
| AC joint dislocation | "Shoulder separation"; CC ligament rupture = grade III; treated by coracoclavicular reconstruction |
| Winging of scapula | Long thoracic nerve (C5,6,7) palsy - serratus anterior weakness |
| Suprascapular nerve | Passes through suprascapular notch (under superior transverse ligament); palsy causes supraspinatus + infraspinatus weakness |
| Os acromiale | Failure of fusion of acromial ossification centers; can cause impingement |
| Coracoid process fracture | Rare; may injure musculocutaneous nerve |
| Scapula fracture | High-energy trauma; associated injuries common (pneumothorax, rib fractures) |
| First bone to ossify | Clavicle (intramembranous - no cartilage template) |
| Last bone to fuse | Clavicle medial epiphysis fuses at ~27 years |
7. NERVE SUPPLY SUMMARY
| Structure | Nerve |
|---|---|
| Trapezius | Accessory nerve (CN XI) + C3, C4 |
| Serratus anterior | Long thoracic nerve (C5, C6, C7) - "nerve of Bell" |
| Rhomboids | Dorsal scapular nerve (C4, C5) |
| Levator scapulae | Dorsal scapular nerve + C3, C4 |
| Subclavius | Nerve to subclavius (C5, C6) |
| Supraspinatus, Infraspinatus | Suprascapular nerve (C5, C6) |
| Deltoid, Teres minor | Axillary nerve (C5, C6) |
Sources: Gray's Anatomy for Students (9780323934237), Imaging Anatomy Vol. 3 - Bones, Joints, Vessels and Nerves (9781626239845), Rockwood and Green's Fractures in Adults 10th ed. (9781975211608)
BDC Reference: BD Chaurasia's Human Anatomy, Volume 1 (Upper Limb & Thorax), Chapter 1 - Bones of the Pectoral Girdle, and Chapter related to Pectoral Region and Axilla. The structure above mirrors BDC's typical organization: bone features → joints → muscles → nerve supply → applied anatomy.
This is a shared conversation. Sign in to Orris to start your own chat.