Clinical toxicology subject
Asking for Preferences
Introduction
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough introduction to Clinical Toxicology drawn from authoritative textbooks:
Introduction to Clinical Toxicology
1. Definition and Scope
Toxicology is the science dealing with the properties, actions, toxicity, fatal dose, detection and estimation of, interpretation of toxicological analysis results, and treatment of poisons. - The Essentials of Forensic Medicine and Toxicology, 36th ed.
The major branches are:
| Branch | Focus |
|---|---|
| Clinical Toxicology | Human diseases caused by, or associated with, abnormal exposure to chemical substances |
| Forensic Toxicology | Medical and legal aspects of harmful effects of chemicals on human beings |
| Occupational/Environmental Toxicology | Recognition, prevention, and treatment of adverse effects from workplace or environmental chemical exposures |
| Toxinology | Toxins produced by living organisms (plants, snakes, spiders, bacteria, fungi) |
2. Definition of Poison
A poison is a substance (solid, liquid, or gaseous) which, if introduced into the living body or brought into contact with any part thereof, produces ill-health or death by its constitutional (systemic) or local effects, or both. - Essentials of Forensic Medicine and Toxicology
Paracelsus (16th century) - Father of Modern Toxicology: "All things are poison and nothing is without poison. It is the dose that determines the poison."
This is the foundation of the dose-response relationship - the same substance can be therapeutic or toxic depending on the dose. Example: morphine relieves pain at therapeutic doses but causes fatal respiratory depression in overdose.
LD50 = The dose of a toxic substance that kills 50% of a test population. It is the standard measure of acute toxicity.
3. Routes of Exposure
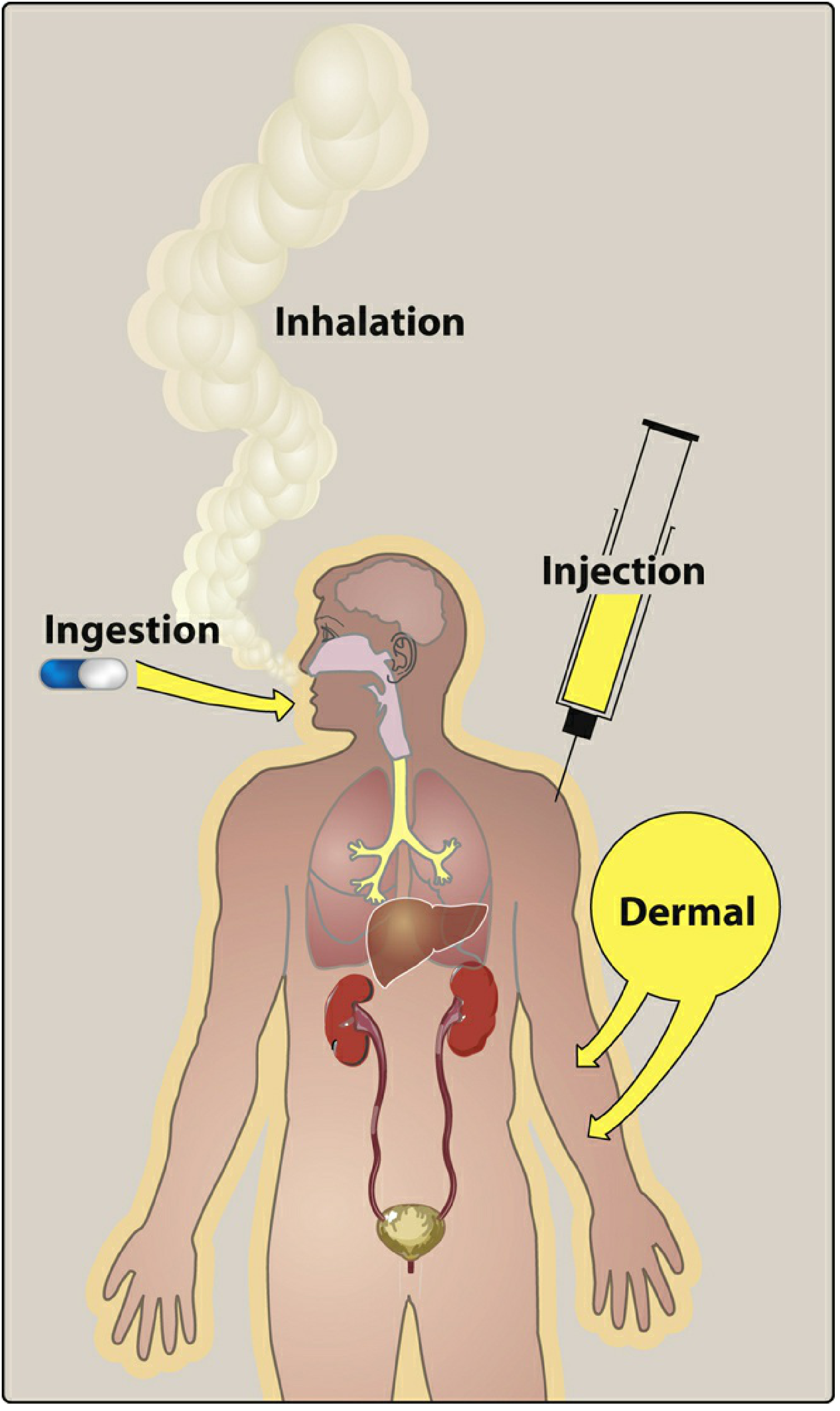
Toxins can enter the body via four major routes - Lippincott Illustrated Reviews: Pharmacology:
- Inhalation - most rapid; directly enters blood via alveoli (e.g. CO, cyanide gas, organophosphate sprays)
- Ingestion - most common route; oral intake; effects are slower onset
- Injection - IV, SC, IM; rapid absorption; bypasses first-pass metabolism
- Dermal absorption - through intact or broken skin (e.g. organophosphate pesticides, corrosives)
- Insufflation (snorting) - nasal mucosa absorption
Speed of action by route: Inhalation > IV injection > IM/SC > Dermal/Ingestion
4. Types of Poisoning
| Type | Description |
|---|---|
| Acute | Large dose taken at once; toxicity manifests immediately |
| Subacute | Intermediate between acute and chronic |
| Chronic | Small amounts repeatedly given over a long period (e.g. lead, mercury, arsenic) |
5. Classification of Poisons
I. Corrosives
- Strong acids: Inorganic (H2SO4, HNO3, HCl); Organic (carbolic acid, oxalic acid, acetic acid)
- Strong alkalis: Hydrates, carbonates of sodium and potassium
- Metallic salts: Zinc chloride, ferric chloride
II. Irritants
- Inorganic - Metallic: Arsenic, lead, mercury, copper, zinc, thallium
- Inorganic - Non-metallic: Phosphorus, chlorine, bromine, iodine
- Organic - Vegetable: Castor oil seeds, croton oil, Abrus precatorius
- Organic - Animal: Cantharides, snake venom, scorpion, spiders
- Mechanical: Powdered glass, diamond dust
III. Neurotoxic
- Cerebral - Somniferous: Opium, barbiturates
- Cerebral - Inebriants: Alcohol, ether, chloroform
- Cerebral - Deliriant: Datura, belladonna, cannabis, cocaine
- Spinal: Nux vomica, gelsemium (strychnine)
- Peripheral: Curare, conium
IV. Cardiotoxic
- Aconite, quinine, digitalis, oleander, nicotine, hydrocyanic acid
V. Asphyxiants
- Irrespirable gases: CO2, carbon monoxide (CO), H2S, coal gas
6. Factors Modifying Toxicity
The action of a poison is modified by:
- Quantity (Dose) - Every drug becomes toxic at a sufficient dose; paradoxically, very large doses may induce vomiting, reducing net absorption (e.g. copper sulphate)
- Route of administration - Inhaled > parenteral > ingested; faster onset on empty stomach
- Age and physical state - Children, elderly, debilitated persons are more susceptible
- Idiosyncrasy - Abnormal (allergic/anaphylactic) reaction at a dose that is safe for most people
- Tolerance - Reduced effect after repeated exposure (e.g. an alcoholic tolerating higher morphine doses)
- Cumulative action - Slow excretion leads to toxic accumulation with repeated dosing (e.g. lead, digitalis)
7. Manner of Poisoning
| Type | Description | Common Examples |
|---|---|---|
| Accidental | Unintentional; often due to improper storage or occupational exposure | CO from charcoal burners, pesticide exposure |
| Suicidal | Self-administered for self-killing | Aluminium phosphide, organophosphates, barbiturates |
| Homicidal | Administered by another person with intent to kill | Arsenic, aconite, strychnine, organophosphates |
8. Brief History of Toxicology
- 3000 BC - Menes Pharaoh I studied poisons
- 1500 BC - Ebers Papyrus listed hemlock, aconite, opium, lead; Atharva Veda described poisons
- 350 BC - Susruta described how poisons were mixed with food, water, perfumes, medicines
- 2nd century BC - Kautilya's Arthashastra documented poisoning as offensive/defensive strategy
- 82 BC - Sulla issued Lex Cornelia in Rome - the first law against poisoning
- 16th century - Paracelsus established the dose-response concept
9. Emergency Treatment of the Poisoned Patient - Overview
The first principle: Treat the patient, not the poison. - Lippincott Illustrated Reviews: Pharmacology
Initial ABCs:
- Airway, Breathing, Circulation
- Address life-threatening changes in BP, HR, respiratory rate, temperature, or cardiac arrhythmias
Empirical Antidote Triad for altered mental status:
- Dextrose - treat hypoglycemia
- Naloxone - reverse opioid/clonidine toxicity
- Thiamine - prevent/treat Wernicke encephalopathy (in ethanol exposure)
Decontamination:
- Ocular: flush with saline to neutral pH
- Dermal: rinse skin
- GI: gastric lavage, activated charcoal, or whole bowel irrigation - ideally within 1 hour of ingestion
- Note: Activated charcoal does NOT bind lead, iron, lithium, potassium, or alcohols
Elimination enhancement:
- Hemodialysis for: methanol, ethylene glycol, salicylates, theophylline, phenobarbital, lithium (low protein binding, small Vd, water soluble)
- Urinary alkalinization (NaHCO3, target urine pH 7.5-8) for: salicylates, phenobarbital
- Multiple-dose activated charcoal for: theophylline, phenobarbital, digoxin, carbamazepine, quinine
Sources:
- Lippincott Illustrated Reviews: Pharmacology (Ch. 46 - Clinical Toxicology)
- The Essentials of Forensic Medicine and Toxicology, 36th Edition (Ch. on Introduction to Toxicology)
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology (Classification, Factors, Manner of Poisoning)
- Katzung's Basic and Clinical Pharmacology, 16th Ed. (Ch. 56 - Occupational & Environmental Toxicology)
This is a shared conversation. Sign in to Orris to start your own chat.