Local anaesthetics
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to deliver a detailed, well-structured answer. Let me compile it.
Local Anaesthetics
1. The Local Anaesthetic Molecule
A typical local anaesthetic molecule has three parts:
- Hydrophobic aromatic ring - gives lipophilicity, membrane penetration
- Intermediate chain - either an ester (—C—O) or amide (—NHC—) linkage
- Hydrophilic tertiary amine - partially protonated at physiologic pH, bearing positive charge
This gives rise to the two major classes:
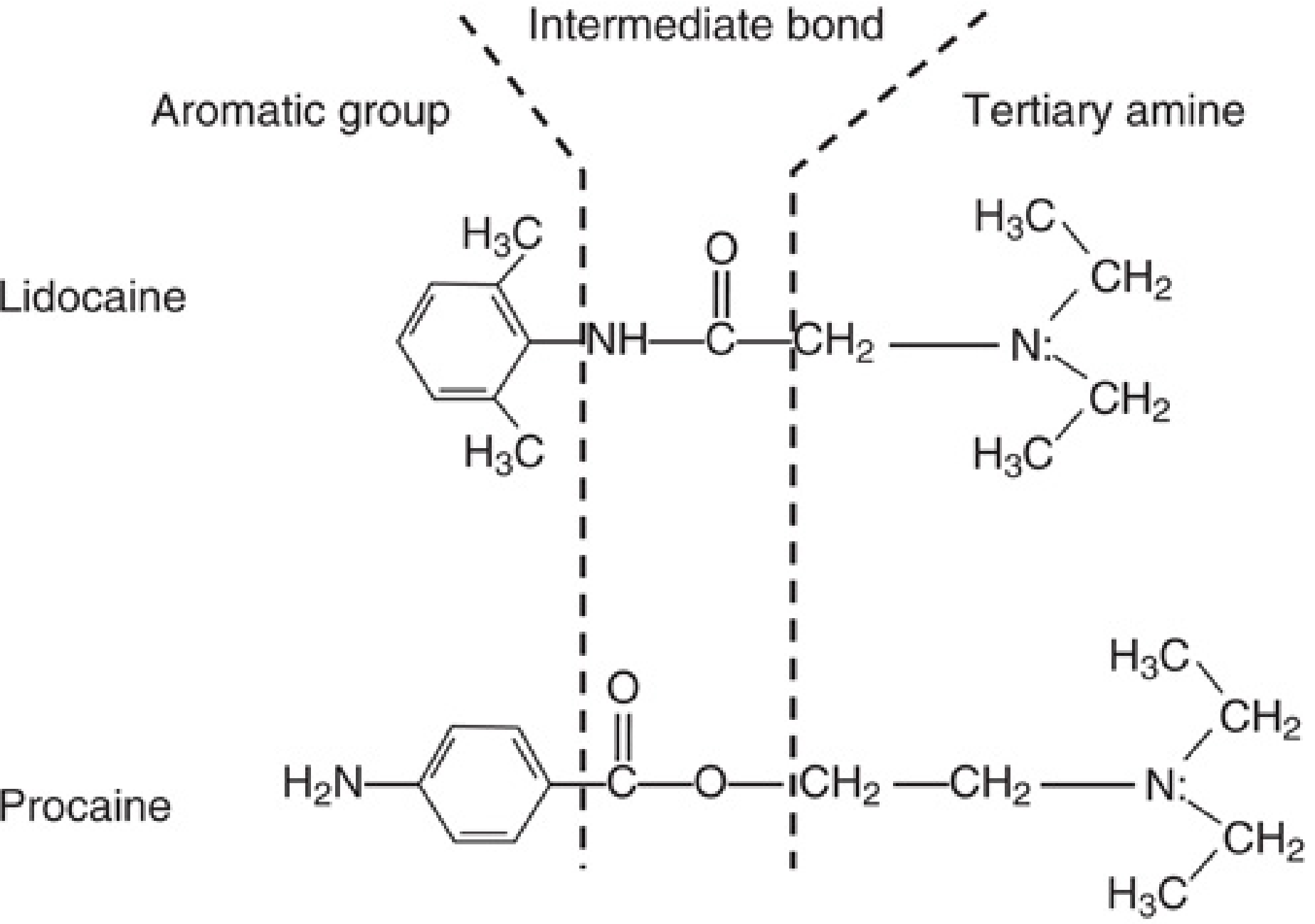
FIG. 25.1 - Miller's Anesthesia, 10e: Lidocaine (aminoamide) vs Procaine (aminoester)
2. Classification
| Class | Linkage | Examples | Metabolism |
|---|---|---|---|
| Aminoesters | Ester (-CO-O-) | Cocaine, Procaine, Chloroprocaine, Tetracaine, Benzocaine | Plasma pseudocholinesterase (rapid) |
| Aminoamides | Amide (-NH-CO-) | Lidocaine, Bupivacaine, Ropivacaine, Prilocaine, Levobupivacaine, Mepivacaine | Hepatic microsomal enzymes (slower) |
Memory aid: Amides have two "i"s in their generic names (lidocaine, bupivacaine); esters have one.
3. Mechanism of Action
Local anaesthetics block voltage-gated Na+ channels, preventing the propagation of action potentials.
The resting nerve:
- The membrane maintains a resting potential of -60 to -90 mV
- At rest it is relatively impermeable to Na+ but selectively permeable to K+
- The Na+/K+ ATPase pump sustains ion gradients
How blockade occurs:
- Local anaesthetics bind to Site 9 on the alpha subunit of the Na+ channel (distinct from the tetrodotoxin binding site, Site 1)
- The neutral (uncharged) form of the drug crosses the lipid membrane; the charged (cationic) form binds to the receptor inside the channel
- Binding reduces Na+ conductance, slows the rate of depolarization, and eventually abolishes the action potential
Use-dependent (phasic) blockade:
- Both the open and inactivated states of the channel bind local anaesthetics more avidly than the resting state
- Repeated depolarization (high-frequency firing) increases drug binding and deepens the block - clinically useful because rapidly firing nociceptive fibers are blocked preferentially
- This is explained by the modulated receptor model
The role of pH and pKa:
- Most local anaesthetics have a pKa of 7.6-9.1, so at physiologic pH (7.4) the majority of molecules are in the charged (ionized) form
- The uncharged form penetrates the nerve sheath; the charged form blocks the channel
- Lower pKa → more uncharged drug at pH 7.4 → faster onset (e.g., lidocaine has a lower pKa than chloroprocaine)
- In infected/acidic tissue: drug remains ionized → reduced efficacy - this explains why local anaesthetics are less effective in inflamed tissue
4. Structure-Activity Relationships
| Property | Clinical Implication |
|---|---|
| ↑ Hydrophobicity (larger alkyl groups) | ↑ Potency, ↑ Duration of action |
| ↑ Protein binding | ↑ Duration of action |
| Lower pKa | Faster onset |
| Enantiomers | S(-) enantiomers (ropivacaine, levobupivacaine) have less cardiotoxicity than racemic mixtures |
5. Differential Nerve Block
Nerve fibers are blocked in a specific order:
| Fiber Type | Modality | Diameter | Myelination | Blocked First? |
|---|---|---|---|---|
| C | Pain, temperature, autonomic | <1 µm | Unmyelinated | Yes |
| Aδ | Sharp pain, temperature | 1-4 µm | Thinly myelinated | Early |
| Aβ | Touch, pressure | 6-12 µm | Myelinated | Later |
| Aα | Motor, proprioception | 12-20 µm | Heavily myelinated | Last |
Clinical sequence: autonomic block → pain/temperature → touch/pressure → proprioception → motor
6. Common Drugs and Dosing
(Bailey and Love's Short Practice of Surgery, 28e; Pye's Surgical Handicraft, 22e)
| Drug | Max Dose (plain) | Max Dose (+adrenaline) | Key Features |
|---|---|---|---|
| Lidocaine | 3 mg/kg (200 mg) | 7 mg/kg (500 mg) | Rapid onset, good tissue diffusion, most popular |
| Bupivacaine | 2 mg/kg | 2 mg/kg | Long-acting, highly cardiotoxic - NEVER use IV |
| Prilocaine | 6 mg/kg | 9 mg/kg | Least systemic toxicity; causes methaemoglobinaemia |
| Ropivacaine | 3-4 mg/kg | - | Less cardiotoxic than bupivacaine; sensory > motor separation |
| Levobupivacaine | 2 mg/kg | - | S(-) isomer of bupivacaine; fewer cardiotoxic properties |
| Chloroprocaine | - | - | Ester; very short-acting, fastest onset |
Lidocaine dosage table (Pye's Surgical Handicraft):
| Concentration | Max volume (plain) | Max volume (+adrenaline 1:200,000) |
|---|---|---|
| 0.5% (5 mg/mL) | 40 mL | 100 mL |
| 1% (10 mg/mL) | 20 mL | 50 mL |
| 2% (20 mg/mL) | 10 mL | 25 mL |
| 4% (40 mg/mL) | 5 mL (topical only) | - |
7. Additives: Adrenaline (Epinephrine)
Adding adrenaline to a local anaesthetic solution:
- Hastens onset (vasoconstriction reduces systemic absorption, so more drug remains locally)
- Prolongs duration of block
- Allows a higher total dose (reduces rate of absorption)
- Provides a haemostatic dry field (wait at least 5 minutes before incision)
Contraindications to adrenaline:
- End-arterial locations (digits, nose, penis, ear lobes) - risk of ischaemic necrosis
- Cardiovascular disease
- Patients on tricyclic antidepressants or MAO inhibitors
8. Local Anaesthetic Systemic Toxicity (LAST)
LAST occurs with accidental intravascular injection or overdose.
CNS toxicity (appears first, at lower plasma levels):
- Prodromal: circumoral numbness/tingling, metallic taste, light-headedness, tinnitus, visual disturbances
- Excitatory: slurred speech, disorientation, muscle twitching, seizures
- CNS depression: unconsciousness, respiratory arrest
Cardiovascular toxicity (requires higher plasma levels):
- Na+ channel blockade in cardiac tissue → conduction disturbances, arrhythmias
- Negative inotropy → cardiovascular collapse
- Bupivacaine is particularly dangerous: cardiac Na+ channels unbind it very slowly ("fast in, slow out"), and toxicity is resistant to resuscitation
- Ropivacaine and levobupivacaine were developed specifically to reduce this risk
Treatment of LAST:
- Stop injection immediately
- Call for help; 100% O2
- Secure airway; benzodiazepine/propofol for seizures (20-50 mg propofol or 1-2 mg midazolam)
- If cardiac arrest: CPR + 20% lipid emulsion (Intralipid) - the cornerstone of treatment
- Bolus: 1.5 mL/kg over 1 minute, then 0.25 mL/kg/min infusion
- Acts as a "lipid sink," sequestering the hydrophobic drug from cardiac tissue
- Small doses of epinephrine (0.5-1 mcg/kg increments)
- Amiodarone for bupivacaine-induced ventricular tachyarrhythmias
- Avoid vasopressin, calcium channel blockers, beta-blockers
9. Specific Toxicity Concerns
| Drug | Special Toxicity |
|---|---|
| Prilocaine | Methaemoglobinaemia (due to o-toluidine metabolite) - treat with methylene blue |
| Bupivacaine | Refractory ventricular arrhythmia and cardiac arrest |
| Cocaine | Vasoconstriction + sympathomimetic effects; only LA with intrinsic vasoconstrictive action |
| Benzocaine | Methaemoglobinaemia (topical use) |
10. Clinical Techniques
Topical anaesthesia: EMLA cream (lidocaine + prilocaine), cocaine 4-10% (nasal/ENT), benzocaine sprays
Infiltration: Direct injection into tissues; use dilute solutions (0.5%) for large areas
Peripheral nerve block: Higher concentrations (1-2%) for faster, denser block
Neuraxial:
- Spinal (subarachnoid): small volumes, hyperbaric or isobaric solutions; rapid dense block
- Epidural: larger volumes, slower onset; used for surgical anaesthesia and labour analgesia
IV regional anaesthesia (Bier's block): Prilocaine 0.5% is the drug of choice; bupivacaine is absolutely contraindicated due to cardiac risk if tourniquet fails
Additives to enhance block:
- Adrenaline (epinephrine)
- Clonidine (α2-agonist): prolongs and intensifies block; may be added epidurally, intrathecally, or with peripheral nerve blocks
- Dexamethasone: prolongs peripheral nerve blocks
11. Conditions Reducing Max Safe Dose
Reduce doses in:
- Low body weight / children
- Elderly / debility
- Hepatic disease (impaired amide metabolism)
- Renal impairment
- Epilepsy
- Heart block
Key references:
- Miller's Anesthesia, 10e, Chapter 25 - The Local Anesthetic Molecule; Mechanism of Action
- Sabiston Textbook of Surgery - Local Anesthetic Drugs, p.1552-1560
- Bailey and Love's Short Practice of Surgery, 28e, Table 23.2
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Local Anesthetic Overdose
Skeletal muscle relaxants
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive data from Miller's Anesthesia, Katzung's Pharmacology, Rosen's Emergency Medicine, and Forensic Medicine. Let me compile the full answer.
Skeletal Muscle Relaxants
Skeletal muscle relaxants divide into two broad categories: (1) Neuromuscular Blocking Drugs (NMBDs) - act at the neuromuscular junction (NMJ), used in anaesthesia; and (2) Centrally Acting Spasmolytic/Antispasmodic Drugs - act in the CNS/spinal cord, used for spasticity and muscle spasm.
Part 1 - Neuromuscular Blocking Drugs (NMBDs)
The Normal Neuromuscular Junction
Before understanding NMBDs, recall how the NMJ works:
- An action potential arrives at the motor nerve terminal
- Ca2+ influx triggers acetylcholine (ACh) release into the synaptic cleft
- ACh diffuses to bind nicotinic ACh receptors (nAChR) on the motor end plate - a pentameric receptor (2α, 1β, 1γ/ε, 1δ subunits)
- Two ACh molecules must bind (at α-β and δ-α subunit interfaces) to open the ion channel
- Na+/K+ flux produces an end plate potential; if large enough, a muscle action potential propagates along the entire fiber
- Released ACh is rapidly hydrolyzed by acetylcholinesterase (AChE) in ~80-100 μs
NMBDs are quaternary ammonium compounds - highly water-soluble, so they do not cross the blood-brain barrier or placenta.
Classification of NMBDs
| Category | Mechanism | Example |
|---|---|---|
| Depolarizing | Binds nAChR as ACh agonist; sustained depolarization → flaccid paralysis | Succinylcholine (suxamethonium) |
| Non-depolarizing - Aminosteroids | Competitive antagonism at nAChR | Rocuronium, Vecuronium, Pancuronium |
| Non-depolarizing - Benzylisoquinolines | Competitive antagonism at nAChR | Atracurium, Cisatracurium, Mivacurium |
A. Depolarizing NMBDs: Succinylcholine (Suxamethonium)
Structure: Two ACh molecules joined together.
Mechanism - Phase I (Depolarizing Block):
- Binds nAChR and opens the channel, causing transient muscle fasciculations
- Sustained depolarization keeps the membrane unresponsive to further ACh
- Succinylcholine is NOT metabolized at the synapse (no AChE there) - it stays until it diffuses away
- Systemically, plasma pseudocholinesterase hydrolyzes it to succinylmonocholine, then succinic acid + choline
- Augmented, NOT reversed, by anticholinesterases
Phase II (Desensitization Block):
- With prolonged exposure, the end plate repolarizes but becomes desensitized ("closed-channel block")
- Behaves like a nondepolarizing block - may show sustained fade on tetanus
- Can paradoxically be partially reversed by anticholinesterases at this stage
Pharmacokinetics:
| Parameter | Value |
|---|---|
| Onset | 45-60 seconds |
| Duration | 6-10 minutes (spontaneous respiration); full recovery ~15 min |
| Metabolism | Plasma pseudocholinesterase |
Dose: 1.5 mg/kg IV (based on total body weight, even in obesity)
Why succinylcholine remains the gold-standard for RSI:
- Fastest onset of all NMBDs
- Shortest duration - spontaneous breathing returns if intubation fails
- Complete and reliable paralysis
Adverse Effects:
| Effect | Mechanism | Clinical Note |
|---|---|---|
| Fasciculations | Initial depolarization of all motor units | Pre-treatment with small non-depolarizing dose reduces fasciculations and post-op myalgia |
| Hyperkalaemia | K+ efflux during depolarization; normal rise 0.5-1 mEq/L | Dangerous in burns, crush injury, spinal cord injury, prolonged immobilization (>24 hrs) - can cause cardiac arrest |
| Bradycardia | Cardiac muscarinic receptor stimulation | Esp. in children and with repeat doses; treated with atropine |
| Tachycardia/HTN | Nicotinic ganglionic stimulation | |
| ↑ Intraocular pressure | Extraocular muscle contraction | Caution in open globe injury |
| ↑ Intragastric pressure | Abdominal muscle fasciculations | Offset by ↑ LOS tone; aspiration risk not proven |
| ↑ Intracranial pressure | Controversial; mechanism unclear | |
| Malignant hyperthermia | Triggers abnormal Ca2+ release from sarcoplasmic reticulum | Rare but life-threatening; treat with dantrolene |
| Prolonged block | Pseudocholinesterase deficiency (genetic) | Usually 20-30 min extra; rarely significant in ED |
| Myalgias | Post-fasciculation | Common next-day complaint |
Contraindications:
- Burns/crush injury/denervation/immobilization (>24 hrs) - hyperkalaemia risk
- Personal or family history of malignant hyperthermia
- Myopathies (Duchenne muscular dystrophy - rhabdomyolysis)
- Known pseudocholinesterase deficiency
B. Non-depolarizing NMBDs
Mechanism: Competitive antagonism at the α-subunit binding sites of the nAChR. Block ACh access; prevent channel opening. Characterized by:
- Fade on tetanic/TOF stimulation (vs. no fade with succinylcholine in Phase I)
- Post-tetanic facilitation (brief post-tetanic reversal)
- Reversed by anticholinesterases
Aminosteroid Compounds
| Drug | Onset | Duration | Dose | Elimination | Notes |
|---|---|---|---|---|---|
| Rocuronium | 60-90 s (fast); 1.2 mg/kg → ~60 s | Intermediate (30-60 min) | 0.6-1.2 mg/kg | Hepatic/biliary | Reversal by sugammadex; alternative to succinylcholine for RSI at 1.2 mg/kg |
| Vecuronium | 3-5 min | Intermediate (25-40 min) | 0.1 mg/kg | Hepatic/biliary | No cardiovascular effects; accumulates in ICU |
| Pancuronium | 3-5 min | Long (60-90 min) | 0.1 mg/kg | Renal (70%) | Vagolytic → tachycardia and ↑BP; cheap |
| Pipecuronium | 3-5 min | Long | 0.07-0.085 mg/kg | Renal | Minimal cardiovascular effects |
Benzylisoquinolinium Compounds
| Drug | Onset | Duration | Dose | Elimination | Notes |
|---|---|---|---|---|---|
| Atracurium | 3-5 min | Intermediate (25-35 min) | 0.5 mg/kg | Hofmann elimination + ester hydrolysis (organ-independent) | Releases histamine; laudanosine metabolite (neurotoxic in excess) |
| Cisatracurium | 3-5 min | Intermediate | 0.1-0.2 mg/kg | Hofmann elimination | Isomer of atracurium; no histamine release; preferred in ICU and renal/hepatic failure |
| Mivacurium | 2-3 min | Short (15-20 min) | 0.2 mg/kg | Plasma pseudocholinesterase | Shortest-acting non-depolarizing NMBD |
Pharmacokinetics of nondepolarizing NMBDs:
- All are inactive orally (highly polar, given IV/IM only)
- Volume of distribution ≈ 80-140 mL/kg (slightly larger than blood volume)
- Duration of block correlates with elimination half-life
- Renal-excreted drugs (pancuronium, vecuronium to a degree) → longer action in renal failure
- Liver-metabolized drugs → shorter, but prolonged in hepatic failure
- All steroidal agents metabolized to 3-hydroxy, 17-hydroxy, or 3,17-dihydroxy metabolites (40-80% as potent as parent); accumulation possible in ICU
Factors Affecting Neuromuscular Block
| Factor | Effect |
|---|---|
| Volatile anaesthetics (isoflurane > sevoflurane > desflurane > halothane > N2O) | Potentiate nondepolarizing block (CNS depression + ↑ muscle blood flow + ↓ membrane sensitivity) |
| Aminoglycosides, polymyxins | Enhance block (Ca2+-channel block at presynaptic terminal) |
| Magnesium | Enhances block (competes with Ca2+) |
| Acidosis, hypothermia | Prolong block |
| Myasthenia gravis | Exquisitely sensitive to nondepolarizing NMBDs; resistant to succinylcholine |
| Eaton-Lambert syndrome | Resistant to both classes (impaired presynaptic ACh release) |
| Burns, immobilization | Resistance to nondepolarizing NMBDs (upregulation of extrajunctional receptors) |
Monitoring Neuromuscular Block: Train-of-Four (TOF)
- Four supramaximal stimuli at 2 Hz; compare amplitude of 4th to 1st twitch (TOF ratio)
- TOF ratio <0.9 = clinically significant residual paralysis
- Quantitative monitoring is the current standard; avoid subjective assessment alone
| TOF count | Depth of block |
|---|---|
| 0 twitches | Profound block |
| 1-2 twitches | Deep block |
| 3-4 twitches | Moderate/shallow block |
| TOF ratio ≥0.9 | Adequate recovery |
Reversal of Neuromuscular Block
1. Anticholinesterases (for nondepolarizing NMBDs and Phase II succinylcholine block)
Mechanism: Inhibit AChE → ↑ ACh at NMJ → outcompetes NMBD for receptor binding.
| Drug | Dose | Duration | Notes |
|---|---|---|---|
| Neostigmine | 0.04-0.07 mg/kg IV | 30-60 min | Most commonly used; must give anticholinergic (glycopyrrolate or atropine) to block muscarinic side-effects |
| Edrophonium | 0.5-1 mg/kg IV | Shorter | Not available in the US since 2018 |
| Pyridostigmine | - | Longer | Used in Asia; rarely used in US |
Must co-administer: Glycopyrrolate (0.2 mg per 1 mg neostigmine) or atropine to prevent bradycardia, salivation, bronchospasm, increased gut motility.
Key limitation: Anticholinesterases have a ceiling effect - ineffective when block is profound (TOF count = 0). Also cannot be used to reverse benzylisoquinoliniums with sugammadex.
2. Sugammadex (for rocuronium and vecuronium only)
Mechanism: Modified γ-cyclodextrin - a hollow, doughnut-shaped molecule with a hydrophobic cavity and hydrophilic exterior. Encapsulates rocuronium/vecuronium in a 1:1 tight complex (association:dissociation = 25,000,000:1 for rocuronium). This removes free drug from plasma, creating a concentration gradient that draws drug off the NMJ back into plasma, where it is immediately captured.
No anticholinergic co-administration needed - does not affect cholinergic transmission at all.
| TOF | Sugammadex Dose | Time to Recovery |
|---|---|---|
| Reappearance of T2 (moderate block) | 2 mg/kg | ~2-3 min |
| 1-2 post-tetanic counts (deep block) | 4 mg/kg | ~3-4 min |
| Immediate reversal (e.g., can't intubate, can't oxygenate, 1.2 mg/kg rocuronium given 3 min prior) | 16 mg/kg | ~1.5 min |
Reintubation after sugammadex: If rocuronium (1.2 mg/kg) is re-administered within 5 minutes of sugammadex reversal, a complete block can be re-established. After 5-30 minutes, a higher dose of rocuronium is needed. Succinylcholine can be used for re-intubation at any time.
Part 2 - Centrally Acting Muscle Relaxants (Spasmolytics)
These drugs are used for spasticity (upper motor neuron lesions - stroke, MS, spinal cord injury, cerebral palsy) and acute muscle spasm (musculoskeletal pain). They act on the CNS or directly on muscle, not the NMJ.
Classification
| Drug | Site of Action | Mechanism |
|---|---|---|
| Baclofen | Spinal cord (presynaptic) | GABA-B agonist |
| Diazepam | Spinal cord + supraspinal | GABA-A positive allosteric modulator |
| Tizanidine | Spinal cord interneurons | α2-adrenergic agonist (↓ excitatory neurotransmitter release) |
| Dantrolene | Skeletal muscle sarcoplasmic reticulum | Blocks ryanodine receptor (RyR1) → ↓ Ca2+ release |
| Carisoprodol / Meprobamate | CNS (nonspecific) | Sedation via GABA-A agonism |
| Cyclobenzaprine | CNS | TCA-like structure; ↓ tonic somatic motor activity |
| Methocarbamol | CNS (polysynaptic inhibition) | Nonspecific |
Key Drugs in Detail
Baclofen
- GABA-B receptor agonist (specifically); structural analogue of GABA
- Inhibits both monosynaptic and polysynaptic reflex transmission in the spinal cord
- Three mechanisms: closure of presynaptic Ca2+ channels, ↑ postsynaptic K+ conductance, ↓ cyclic-AMP synthesis
- Dose: 40-80 mg/day; toxicity at ≥150-200 mg/day
- Intrathecal baclofen pump for severe spasticity
- Side effects: fatigue, dizziness, confusion, weakness, nausea
- Overdose: Agitation, seizures, flaccid paralysis, coma, respiratory depression; treat with physostigmine 1-2 mg slow IV
Diazepam
- Facilitates GABA-A at spinal cord level (also supraspinal)
- Effective even after cord transection (spinal cord mechanism)
- Dose: 4 mg/day titrated to max 60 mg/day
- Main limitation: sedation at effective doses
Tizanidine
- α2-agonist at spinal interneurons - reduces release of excitatory neurotransmitters from descending pathways
- May also have postsynaptic inhibitory effects
- Less sedating than diazepam at equivalent muscle-relaxant doses
Dantrolene
- Unique - acts peripherally on skeletal muscle (not CNS)
- Blocks the ryanodine receptor (RyR1) on the sarcoplasmic reticulum → ↓ Ca2+ release → ↓ excitation-contraction coupling
- Primary use: Malignant hyperthermia (triggered by volatile anaesthetics or succinylcholine)
- IV dantrolene 2.5 mg/kg, repeat until symptoms resolve (max 10 mg/kg)
- Also used for: spasticity, neuroleptic malignant syndrome
- Side effects: muscle weakness (including respiratory muscles), hepatotoxicity (with long-term oral use)
Summary Comparison Table
| Feature | Succinylcholine | Rocuronium | Vecuronium | Atracurium | Cisatracurium |
|---|---|---|---|---|---|
| Class | Depolarizing | Aminosteroid | Aminosteroid | Benzylisoquinoline | Benzylisoquinoline |
| Onset | <1 min | 1-2 min (1.2 mg/kg) | 3-5 min | 3-5 min | 3-5 min |
| Duration | 6-10 min | 30-60 min | 25-40 min | 25-35 min | 25-35 min |
| Reversal | Spontaneous only | Sugammadex | Sugammadex or neostigmine | Neostigmine only | Neostigmine only |
| Metabolism | Pseudocholinesterase | Hepatic/biliary | Hepatic/biliary | Hofmann + ester hydrolysis | Hofmann elimination |
| Safe in renal failure? | Yes | Caution | Caution | Yes | Yes |
| Safe in hepatic failure? | Yes | Caution | Caution | Yes | Yes |
| Histamine release? | No | No | No | Yes | No |
| Cardiovascular effect | Brady/tachy (muscarinic/nicotinic) | Minimal | None | Hypotension (histamine) | None |
Key References:
- Miller's Anesthesia, 10e - Chapter 24 (Reversal, Sugammadex), Chapter 11 (NMJ physiology)
- Katzung's Basic & Clinical Pharmacology, 16e - Chapter 27 (NMBDs, Spasmolytic Drugs)
- Rosen's Emergency Medicine - Neuromuscular Blocking Agents
- Forensic Medicine & Toxicology, 36e - Baclofen toxicity
This is a shared conversation. Sign in to Orris to start your own chat.