Give a detail explanation on anatomy, examination, investigations, rehabilitation exercises & add PROMS with treatment including ayurveda part
"knee osteoarthritis"[MeSH Terms] AND "rehabilitation"[MeSH Terms]
knee joint Ayurveda treatment Janu Basti Panchakarma osteoarthritis 2024
"knee"[MeSH Terms] AND "patient reported outcome"[MeSH Terms] AND "exercise"[MeSH Terms]
"knee osteoarthritis" AND "exercise therapy"
KOOS WOMAC Oxford Knee Score patient reported outcome measures knee joint physiotherapy
https://pmc.ncbi.nlm.nih.gov/articles/PMC12444219
knee rehabilitation exercises phases ACL meniscal OA physiotherapy protocol 2024
The Knee Joint - A Complete Clinical Reference
1. ANATOMY
1.1 Joint Type & Compartments
- Medial tibiofemoral compartment
- Lateral tibiofemoral compartment
- Patellofemoral compartment
1.2 Osseous Structures
| Structure | Key Points |
|---|---|
| Distal Femur | Medial and lateral condyles; intercondylar notch houses the cruciate ligaments |
| Proximal Tibia | Medial and lateral tibial plateaus; tibial tuberosity (insertion of patellar tendon); Gerdy's tubercle (IT band insertion) |
| Patella | Largest sesamoid bone; acts as a pulley for quadriceps; has the thickest articular cartilage in the body (designed for loads up to 20x body weight) |
| Fibular Head | Provides attachment for the LCL and biceps femoris |
1.3 Articular Cartilage
1.4 Menisci
| Feature | Medial Meniscus | Lateral Meniscus |
|---|---|---|
| Shape | C-shaped (more open) | O-shaped (more circular) |
| Mobility | Less mobile (attached to MCL & capsule) | More mobile |
| Blood supply | Outer 1/3 (red zone) only | Outer 1/3 |
| Injury frequency | More commonly torn | Less commonly torn |
1.5 Ligaments
- ACL - runs from posterior lateral femoral condyle to anterior intercondylar area of tibia; primary restraint to anterior tibial displacement; also resists internal rotation
- PCL - stronger than ACL; runs from anterior medial femoral condyle to posterior tibia; primary restraint to posterior tibial displacement
- MCL (Medial Collateral Ligament) - has superficial and deep components plus the posterior oblique ligament (POL); resists valgus and external rotation forces
- LCL (Lateral Collateral Ligament) - resists varus forces; runs from lateral femoral epicondyle to fibular head
- Popliteus tendon, popliteofibular ligament, arcuate ligament - resist varus, external rotation, and posterior tibial translation
1.6 Joint Capsule & Bursae
- Suprapatellar bursa - communicates with joint cavity (fills with effusion)
- Prepatellar bursa - "housemaid's knee" when inflamed
- Infrapatellar bursa (superficial & deep)
- Pes anserine bursa - medial, between MCL and pes anserine tendons
- Baker's cyst (popliteal cyst) - posterior, communicates with joint via an opening between medial gastrocnemius and semimembranosus
1.7 Extensor Mechanism
1.8 Dynamic Stabilizers (Muscles)
| Group | Muscles | Function |
|---|---|---|
| Extensors | Quadriceps | Knee extension; stabilize patella |
| Flexors/Rotators | Hamstrings (biceps femoris, semimembranosus, semitendinosus) | Flexion; tibial rotation |
| Pes Anserinus | Sartorius, gracilis, semitendinosus | Medial stabilizers; attach on proximal medial tibia |
| IT Band | TFL + gluteus maximus | Lateral stabilizer via Gerdy's tubercle |
| Popliteus | Popliteus | "Unlocks" knee from full extension; resists posterolateral rotation |
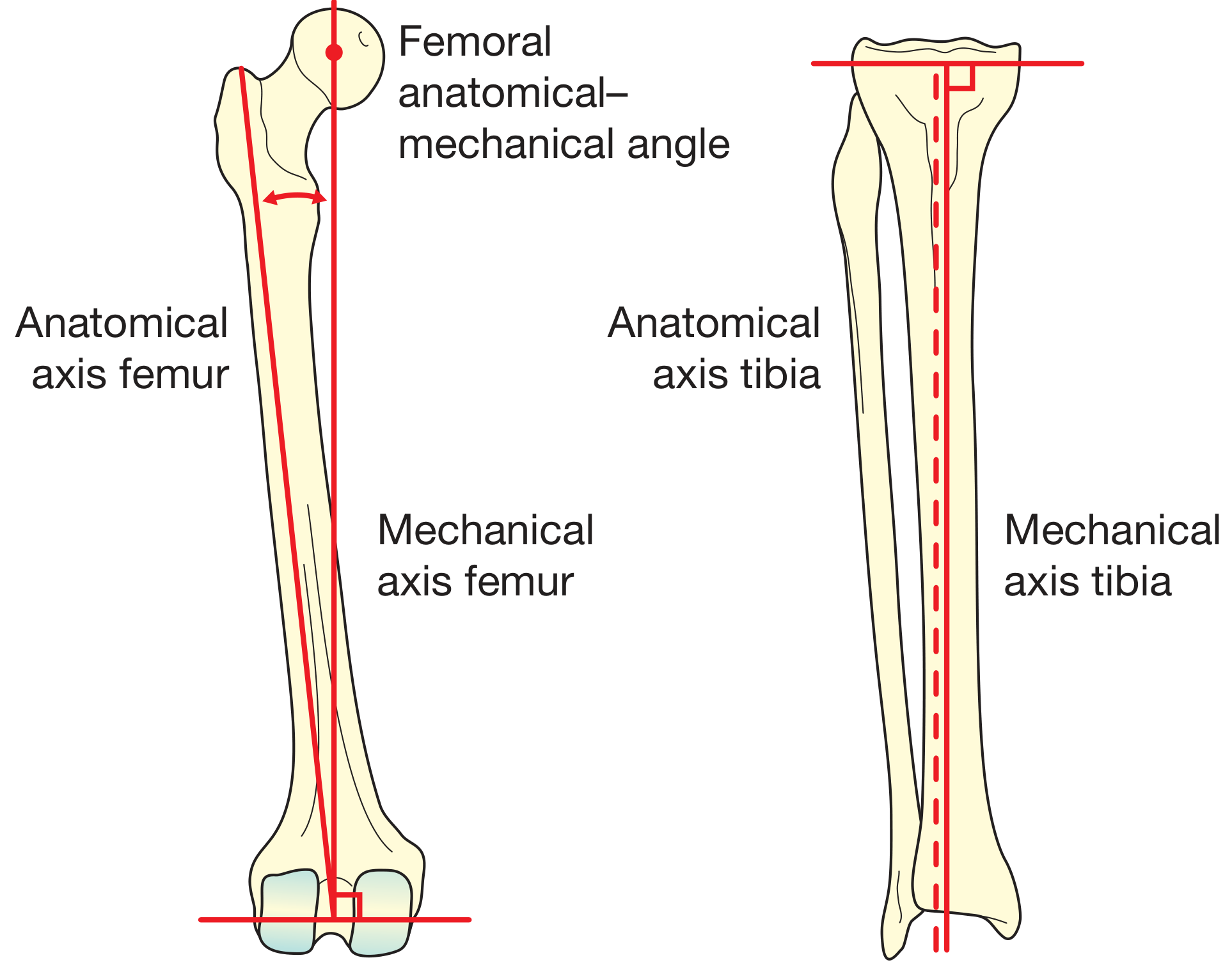
1.9 Biomechanics & Axes
2. CLINICAL EXAMINATION
2.1 Look (Inspection)
- Alignment: Varus (bow-legs) or valgus (knock-knees) deformity
- Measure intermalleolar distance for valgus; intermédial knee distance for varus
- Muscle bulk: Quadriceps wasting (compare sides)
- Side view: Fixed flexion deformity or recurvatum (hyperextension)
- Back: Popliteal swelling, hamstring bulk
- Antalgic gait - shortened stance phase on painful limb (OA)
- Varus thrust - dynamic collapse into varus during stance (medial compartment OA)
- High-stepping gait - foot drop
- Skin, scars, sinuses
- Swelling (prepatellar, suprapatellar, popliteal)
- Deformity
2.2 Feel (Palpation)
- Temperature: Use dorsum of hand; warmth = inflammation/infection
- Effusion: Patellar tap test (large effusion) / Bulge/sweep test (small effusion)
- Joint lines: Medial and lateral joint line tenderness (meniscal pathology, OA)
- Bony landmarks: Tibial tuberosity (Osgood-Schlatter), fibular head, femoral condyles, Gerdy's tubercle
- Soft tissues: Quadriceps tendon, patellar tendon, collateral ligaments, popliteal fossa (Baker's cyst)
- Muscle: Hamstrings, calf
2.3 Move (Range of Motion)
- Active ROM: Ask patient to fully flex and extend
- Passive ROM: Assessor moves joint; note end-feel (firm = normal, springy = meniscal block, empty = pain)
- Normal: 0° extension (some hyperextension normal) to 135° flexion
- Fixed flexion test: Sit patient upright with knees hanging over edge; if flexion deformity persists, it is in the knee (not hip)
2.4 Special Tests
Collateral Ligaments
- Valgus stress test at 30° flexion - tests MCL (at 0° full extension, also tests posterior capsule/PCL)
- Varus stress test at 10-30° flexion - tests LCL
Cruciate Ligaments
- Lachman test (most sensitive for ACL) - 20-30° flexion, anterior tibial drawer; firm vs. soft end-feel
- Anterior drawer test - 90° flexion, anterior tibial pull
- Pivot shift test (most specific for ACL functional instability) - internal rotation + valgus stress while extending; a clunk = positive
- Posterior drawer test - 90° flexion, posterior tibial push (PCL)
- Posterior sag sign (Godfrey's test) - PCL rupture causes tibia to sag posteriorly with hip and knee at 90°
Meniscal Tests
- McMurray's test - flex knee fully, then extend with external rotation (medial meniscus) or internal rotation (lateral meniscus); click = positive
- Thessaly test - single-leg stance at 20° flexion, rotate body; joint line pain = positive (reported higher sensitivity than McMurray's)
- Apley's grind test (compression/distraction) - prone, knee at 90°; compression + rotation tests meniscus; distraction tests ligaments
Patellofemoral Tests
- Patellar tap test - large effusion
- Patellar grind (Clarke's test) - compress patella into trochlea, patient contracts quads; pain = chondromalacia
- Patellar apprehension (Fairbank's test) - lateral patellar displacement at 30° flexion; apprehension/contraction = instability
- Patellar tracking ('J' sign) - sit, legs hanging at 90°, slowly extend; lateral jump near full extension = maltracking
Other
- Ober's test - IT band tightness
- Thomas test - hip flexor tightness
- Trendelenburg test - hip abductor weakness
3. INVESTIGATIONS
3.1 Imaging
| Investigation | Indications | Key Findings |
|---|---|---|
| Plain X-ray (weight-bearing AP, lateral, skyline) | First-line for OA, fractures, alignment | OA: joint space narrowing, subchondral sclerosis, osteophytes, subchondral cysts; Always do weight-bearing to show true joint space |
| MRI | Soft tissue pathology - first choice for meniscal tears, ligament injuries, cartilage defects, bone marrow oedema | Not routinely needed pre-TKR; most sensitive for ACL, meniscal, chondral assessment |
| CT scan | Complex intra-articular fractures, tibial plateau fractures, rotational alignment, pre-op planning | Bony detail; CT arthrogram when MRI contraindicated |
| Ultrasound | Soft tissue - Baker's cyst, popliteal vessels, tendon assessment; guided injections | Dynamic assessment of tendon; effusion aspiration guidance |
| Bone scan (SPECT/CT) | Occult fractures, stress fractures, osteonecrosis, infection | Increased uptake in active bone pathology |
3.2 X-Ray Views
- AP (weight-bearing): Kellgren-Lawrence grading of OA; alignment
- Lateral (30° flexion): Patella height (Insall-Salvati ratio), posterior condyle, tibial slope
- Skyline (Merchant/axial): Patellofemoral compartment, trochlear dysplasia
- Long-leg alignment (scanogram): Mechanical axis; varus/valgus correction planning
- Rosenberg view (posteroanterior at 45°): Most sensitive plain X-ray view for joint space in early OA
3.3 Kellgren-Lawrence Grading (OA)
| Grade | Description |
|---|---|
| 0 | Normal |
| 1 | Doubtful narrowing; possible osteophyte |
| 2 | Definite osteophyte; possible joint space narrowing |
| 3 | Multiple osteophytes; definite narrowing; some sclerosis |
| 4 | Large osteophytes; marked narrowing; severe sclerosis; possible bony deformity |
3.4 Blood Investigations
| Test | Purpose |
|---|---|
| FBC, CRP, ESR | Infection, inflammatory arthritis |
| Rheumatoid factor, anti-CCP | Rheumatoid arthritis |
| Uric acid | Gout (though normal during acute attack) |
| ANA, dsDNA | SLE |
| HLA-B27 | Seronegative spondyloarthropathy |
| Blood cultures | Septic arthritis |
| Coagulation | Pre-operative |
3.5 Synovial Fluid Analysis (Aspiration)
| Parameter | Normal | OA | Inflammatory | Septic |
|---|---|---|---|---|
| Appearance | Clear | Yellow, clear | Yellow, turbid | Purulent, opaque |
| WBC/mm³ | < 200 | < 2,000 | 2,000-50,000 | > 50,000 |
| PMN% | < 25% | < 25% | > 50% | > 75% |
| Glucose | = serum | = serum | ↓ | << serum |
| Culture | Negative | Negative | Negative | Positive |
| Crystals | None | None | Gout (urate), CPPD (pyrophosphate) | None |
3.6 Arthroscopy (Diagnostic)
4. COMMON CONDITIONS, DIAGNOSIS & TREATMENT
4.1 Knee Osteoarthritis (OA)

- Weight loss, exercise, patient education, self-management
- Analgesics: topical NSAIDs (first-line), oral NSAIDs, paracetamol
- Walking aids, offloader brace, orthotics
- Intra-articular corticosteroid injection (short-term relief in flares; not long-term)
- Hyaluronic acid - not recommended by AAOS
- Oral narcotics - not recommended
- High tibial osteotomy (HTO) - younger patients with unicompartmental OA + malalignment; realigns mechanical axis to offload diseased compartment
- Unicompartmental knee replacement (UKR) - single compartment disease; shorter recovery
- Total knee replacement (TKR) - end-stage disease; traditional goal = restore mechanical axis to neutral
- Arthrodesis - last resort; young patient with failed TKR or infection
4.2 ACL Injury
- Conservative: Physiotherapy, bracing - for low-demand, older, sedentary patients
- Surgical (ACL reconstruction): Recommended for young, active patients; pivot sport athletes; associated meniscal/chondral injuries. Graft options: patellar tendon (BTB), hamstring (gracilis + semitendinosus), quadriceps tendon, allograft
4.3 Meniscal Tears
- Conservative: Degenerative tears in older patients without mechanical symptoms
- Arthroscopic partial meniscectomy: Unstable tears with mechanical symptoms
- Meniscal repair: Younger patients, early presentation, vascular outer 1/3, stable tear pattern, concomitant ACL reconstruction - Bailey & Love's, 28th Ed.
4.4 Patellofemoral Pain Syndrome (PFPS)
4.5 Septic Arthritis
5. REHABILITATION EXERCISES
5.1 General Principles
5.2 Phase-Based Rehabilitation (OA & General Knee)
Phase 1 - Acute/Early Phase (Week 1-2)
| Exercise | Description | Sets/Reps |
|---|---|---|
| Ankle pumps | Flex/extend ankle; promote circulation | 3 × 20 |
| Quad sets (isometric) | Press back of knee to bed, contract quads | 3 × 10, hold 5s |
| Inner range quads | Knee supported at 30° under roll, extend actively | 3 × 10 |
| Straight leg raise (SLR) | Leg raised to 45°, quads contracted; all 4 planes | 3 × 10 |
| Heel slides | Slide heel to bend knee (flexion ROM) | 3 × 10 |
| Calf raises (seated) | Improve venous return | 3 × 15 |
| Ice + elevation | 20 minutes, 4-6 times/day | - |
Phase 2 - Sub-acute Phase (Week 3-6)
| Exercise | Description | Sets/Reps |
|---|---|---|
| Mini squats (0-30°) | Partial weight-bearing squat, hands on support | 3 × 15 |
| Step-ups (forward & lateral) | Low step 5-10 cm; progress height gradually | 3 × 10 each side |
| Terminal knee extension (TKE) | Resistance band behind knee, extend from 30° to 0° | 3 × 15 |
| Hamstring curls (prone) | Flex knee against gravity/resistance | 3 × 12 |
| Hip abduction (side-lying) | Strengthens glute medius; reduces knee valgus | 3 × 15 |
| Static cycling | Low resistance; ROM & cardiovascular benefit | 15-20 min |
| VMO emphasis squats | Feet slightly externally rotated | 3 × 12 |
Phase 3 - Strengthening Phase (Week 6-12)
| Exercise | Description | Sets/Reps |
|---|---|---|
| Full squats (0-90°) | Bodyweight to loaded; watch for valgus collapse | 3 × 12 |
| Leg press | Controlled full ROM; start low resistance | 3 × 12 |
| Lunges (forward/lateral) | Functional multi-plane movement | 3 × 10 each leg |
| Wall squats (isometric) | Sustained quad + VMO activation | 3 × 30-60s |
| Single-leg balance | Eyes open → eyes closed → unstable surface | 3 × 30s each |
| Nordic hamstring curls | Eccentric hamstring strengthening | 3 × 8 |
| Aquatic exercises | Pool walking, pool squats; offloads joint | 20-30 min |
Phase 4 - Functional/Return-to-Sport Phase (Week 12+)
| Exercise | Description |
|---|---|
| Bulgarian split squats | Single-leg loaded squat |
| Box jumps / Plyometrics | ACL patients only after strength testing clears |
| Lateral band walks | Hip abductor strengthening in functional position |
| Agility ladder drills | Neuromuscular coordination |
| Running progression | Walk-jog intervals → continuous jog → sprint |
| Sport-specific drills | Cutting, pivoting, deceleration |
5.3 Aquatic Exercise (Hydrotherapy)
6. PATIENT-REPORTED OUTCOME MEASURES (PROMs)
6.1 Summary Table of Key Knee PROMs
| PROM | Full Name | Items | Subscales | Best Used For | Score Range | Interpretation |
|---|---|---|---|---|---|---|
| KOOS | Knee Injury & Osteoarthritis Outcome Score | 42 | Pain, Symptoms, ADL, Sport/Rec, QoL | OA, ACL, Meniscal injury, TKR | 0-100 per subscale | Higher = better |
| KOOS-PS | KOOS Physical Function Short Form | 7 | Physical function | Quick functional screen | 0-100 | Higher = better |
| WOMAC | Western Ontario & McMaster Universities OA Index | 24 | Pain (5), Stiffness (2), Function (17) | Knee & hip OA | 0-96 (Likert) or 0-100 (VAS) | Lower = better |
| Oxford Knee Score (OKS) | Oxford Knee Score | 12 | Single score | TKR pre/post-op assessment | 0-48 | Higher = better |
| Lysholm Knee Scale | Lysholm Knee Scoring Scale | 8 | Limp, locking, instability, pain, swelling, stair climbing, squat | ACL, ligament injuries | 0-100 | Higher = better |
| IKDC | Int'l Knee Documentation Committee Subjective Knee Form | 18 | Symptoms, sport activity, function | Ligament/meniscal injury, ACL | 0-100 | Higher = better |
| Tegner Activity Scale | Tegner Activity Level Scale | 1 | Activity level | ACL, sports-related injury | 0-10 (0=sick leave, 10=competitive sport) | Higher = more active |
| VAS / NRS | Visual Analogue / Numeric Rating Scale | 1 | Pain intensity | Any knee condition | 0-10 | Lower = less pain |
| SF-36 / SF-12 | Short Form Health Survey | 36/12 | 8 domains, PCS + MCS | General health-related QoL | 0-100 | Higher = better |
| PROMIS | Patient-Reported Outcomes Measurement Information System | Adaptive | Pain, function, fatigue, mental health | Comprehensive; computer-adaptive | T-score (50 = norm) | Condition dependent |
| KSS | Knee Society Score | Dual | Knee score + Function score | TKR outcomes | 0-100 each | Higher = better |
| ACL-RSI | ACL Return to Sport Index | 12 | Psychological readiness | Post-ACL reconstruction | 0-100 | ≥90 = cleared psychologically |
6.2 Detailed Notes on Key PROMs
- 42 items across 5 subscales: Pain (9), Symptoms (7), ADL (17), Sport/Recreation (5), QoL (4)
- Each item scored 0-4; transformed to 0-100 (0 = extreme problems, 100 = no problems)
- Reliability ICC >0.8 on most subscales
- Validated for ACL reconstruction, meniscal tears, OA; extends and is compatible with WOMAC
- The 2024 KOOS review study confirms it as the most comprehensive functional PROM for the knee
- 24-item self-report; excellent reliability (ICC 0.90 for pain); high concurrent validity with SF-36
- Primarily validated for OA; less sensitive for younger/more active patients
- 12-item questionnaire; 5-point Likert scale; score 0-48
- Excellent reliability and validity especially for TKR
- MCID (Minimum Clinically Important Difference) = 5 points
- 8-item; clinician + patient scored; used widely for ligament injuries
- Categories: Excellent (95-100), Good (84-94), Fair (65-83), Poor (<65)
- Single item, 0-10 ordinal scale of activity
- Pre-injury vs. post-treatment comparison important for return-to-sport decisions
- Often overlooked but critical: psychological readiness is a predictor of re-injury
- Score ≥90 on ACL-RSI is recommended before return to cutting/pivoting sport
| Clinical Scenario | Recommended PROM(s) |
|---|---|
| Knee OA (conservative management) | KOOS or WOMAC + VAS |
| ACL reconstruction | KOOS + IKDC + Lysholm + Tegner + ACL-RSI |
| Meniscal injury | KOOS + Lysholm |
| TKR/UKR | Oxford Knee Score (OKS) + KOOS + KSS |
| Patellofemoral pain | KOOS + VAS (WOMAC less specific for PFPS) |
| Research / general | PROMIS (computer-adaptive, efficient) |
7. TREATMENT SUMMARY
7.1 Pharmacological Treatment
| Drug Class | Examples | Use |
|---|---|---|
| Topical NSAIDs | Diclofenac gel, Ketoprofen | First-line OA; fewer GI/renal side effects |
| Oral NSAIDs | Ibuprofen, Naproxen, Celecoxib | Moderate OA, acute flares |
| Paracetamol (Acetaminophen) | Paracetamol 1g QID | Mild-moderate OA |
| Opioids | Tramadol (weak opioid) | Not recommended by AAOS for knee OA |
| Intra-articular corticosteroids | Triamcinolone, Methylprednisolone | Short-term flare control; max 3-4/year |
| Hyaluronic acid (viscosupplementation) | Synvisc, Ostenil | Evidence conflicting; not recommended by AAOS |
| Duloxetine | 60-120 mg/day | Chronic pain with central sensitization component |
| Supplements | Glucosamine, Chondroitin | Limited evidence (AAOS: limited recommendation only) |
7.2 Physical & Allied Health Interventions
- Physiotherapy (strengthening, manual therapy, taping)
- Occupational therapy (joint protection, aids)
- Weight loss (each 1 kg lost reduces knee load by ~4 kg)
- Orthotics (medial wedge for lateral OA; lateral wedge NOT recommended by AAOS)
- Offloader brace (valgus brace for medial compartment OA)
- TENS, acupuncture (limited evidence; AAOS 2-star)
- PRP (Platelet-rich plasma) - AAOS: limited, may reduce pain (2-star)
7.3 Surgical Treatment
| Procedure | Indication |
|---|---|
| Arthroscopic debridement/washout | NOT recommended for OA (AAOS strong against) |
| Arthroscopic meniscectomy | Symptomatic meniscal tear with mechanical symptoms |
| Meniscal repair | Young patient, vascular zone tear, repairable |
| ACL reconstruction | Active patients with functional instability |
| Chondrocyte transplant (MACI/ACI) | Young patient, full-thickness cartilage defect |
| Osteotomy (HTO/DFO) | Young patient, unicompartmental OA + malalignment |
| Unicompartmental knee replacement (UKR) | Single compartment OA, intact cruciate ligaments |
| Total Knee Replacement (TKR) | End-stage, multi-compartment OA; failed conservative/other surgery |
| Arthrodesis | Failed TKR, chronic septic arthritis |
8. AYURVEDA & INTEGRATIVE APPROACH TO THE KNEE
8.1 Ayurvedic Understanding
8.2 Panchakarma Procedures for the Knee
Janu Basti (Knee Oil Retention Therapy)
- A dough ring (made of black gram flour) is placed over the knee to create a well
- Warm medicated oil (Dhanwantara Taila, Ksheerabala Taila, or Mahanarayan Taila) is poured into the well and retained for 30-45 minutes at therapeutic temperature
- The warmth allows the oil to penetrate deeply into ligaments, cartilage, and synovial membrane
- Benefits: Reduces pain, stiffness, and swelling; nourishes joint tissues; improves ROM
- Indications: OA knee, chronic knee pain, Sandhigatavata
- Contraindications: Acute infection, open wounds, severe acute trauma
Matra Basti (Therapeutic Oil Enema)
- Small-volume medicated oil enema (30-60 mL) using Ksheerabala Taila
- Considered the prime treatment for Vatavyadhi (musculoskeletal/degenerative disorders)
- Rectal absorption provides high bioavailability; lipid-soluble drugs cross rectal mucosa rapidly
- A 2025 RCT protocol (Rai et al., JMIR Protocols 2025) is evaluating Matra Basti + Janu Basti combined with Laksha Guggulu for primary knee OA
Abhyanga (Therapeutic Oil Massage)
- Full-body or localized warm medicated oil massage
- Oils used: Mahanarayan Taila (anti-inflammatory, rejuvenative), Ksheerabala Taila
- Improves circulation, reduces Vata, nourishes joint tissues
- Done before Swedana (fomentation)
Swedana (Heat Fomentation)
- Steam therapy or local fomentation after Abhyanga
- Relieves stiffness; opens channels (Srotas); prepares joint for deeper treatments
- Types: Nadi Sweda (steam pipe), Patra Pinda Sweda (herbal leaf bolus), Jambira Pinda Sweda (lemon bolus)
Upanaha Sweda (Medicated Poultice)
- Herbal paste applied warm over the knee joint overnight
- Herbs: Eranda (castor), sesame, salt, vinegar
- Used for chronic stiffness and degeneration
Mridu Samshodhana (Mild Purgation)
- Mild virechana (purgation) to eliminate Ama
- Indicated when inflammatory/toxic component is present
Lepa (External Medicated Paste)
- Herbal paste applied topically
- Guggulu-based formulations (Yogaraja Guggulu, Trayodashanga Guggulu)
8.3 Ayurvedic Internal Medicines
| Formulation | Key Ingredients | Action |
|---|---|---|
| Yogaraja Guggulu | Guggul, triphala, trikatu, sesame oil | Anti-inflammatory, anti-arthritic; Vata pacifying |
| Trayodashanga Guggulu | Guggul + 13 herbs incl. ashwagandha | Analgesic, anti-rheumatic; Vata-pacifying |
| Laksha Guggulu | Laksha (lac), guggul, ashwagandha, nagabala | Bone and cartilage regeneration; fracture healing |
| Muktashukti Bhasma | Calcined pearl oyster shell | Calcium supplementation; anti-inflammatory |
| Ashwagandha (Withania somnifera) | Alkaloids, withanolides | Adaptogen; muscle and ligament strengthening; reduces stiffness |
| Shallaki / Boswellia serrata | Boswellic acids | Well-evidenced anti-inflammatory; inhibits 5-LOX; reduces knee OA pain |
| Guggulu (Commiphora mukul) | Guggulsterones | Anti-inflammatory; balances Vata & Kapha |
| Triphala | Amalaki, bibhitaki, haritaki | Antioxidant; Ama removal; GI support for drug absorption |
| Shatavari (Asparagus racemosus) | Steroidal saponins | Rejuvenative; anti-inflammatory |
| Punarnava (Boerhavia diffusa) | Punarnavine | Anti-oedematous; reduces joint swelling |
8.4 Dietary Guidelines (Ahara) in Ayurveda
- Avoid: Cold, dry, stale food; excessive raw salads; cold drinks; refined flour; nightshades (in Vata conditions)
- Include: Warm, unctuous, easily digestible food; ghee, sesame oil; root vegetables; ginger, turmeric, black pepper; warm soups
- Turmeric (Haridra): Curcumin has documented anti-inflammatory effects; combine with black pepper for absorption
8.5 Evidence for Ayurveda in Knee OA
9. INTEGRATIVE TREATMENT ALGORITHM
KNEE PAIN PRESENTATION
|
─────────────────
| |
ACUTE INJURY CHRONIC / GRADUAL ONSET
(trauma, sport) (OA, overuse, degeneration)
| |
Imaging (X-ray, Weight-bearing X-ray
MRI) + Special K-L grading
tests |
| |
DIAGNOSE: Grade I-II OA: Grade III-IV OA:
- ACL/PCL Non-operative: Surgical evaluation
- Meniscus Exercise + PT HTO / UKR / TKR
- Ligament NSAIDs (topical)
- Fracture Weight loss
Ayurveda + Physio
| (Janu Basti +
| Strengthening exercises)
Surgical or |
conservative PROM monitoring:
decision KOOS / WOMAC / OKS
|
Rehabilitation
(Phased - Phase 1 to 4)
PROMS at baseline, 6 weeks, 3 months, 6 months, 1 year
Key References
- Bailey & Love's Short Practice of Surgery, 28th Edition - Knee anatomy, examination, OA, ACL, meniscal injuries
- Miller's Review of Orthopaedics, 9th Edition - AAOS evidence-based guidelines for knee OA
- Rockwood & Green's Fractures in Adults, 10th Ed. - Medial and lateral knee anatomy
- Lawford et al., Cochrane 2024 - Exercise for knee OA: systematic review
- Yan et al., BMJ 2025 - Comparative efficacy of exercise modalities in knee OA (network meta-analysis)
- EULAR 2023 Updated Guidelines - Non-pharmacological management of hip and knee OA
- Rai et al., JMIR Protocols 2025 - Multimodal Ayurveda regimen (Janu Basti + Matra Basti + Laksha Guggulu) RCT protocol for primary knee OA
- Kshirsagar et al., Int J Res Orthop 2024 - Panchakarma therapy improving KOOS in OA
- Physio-pedia KOOS - KOOS subscale details
Generate a rehabilitation protocol PDF with exercise progression charts
mkdir -p /home/daytona/workspace/knee-rehab-pdf && ls /home/daytona/workspace/kn…
~/knee-rehab-pdf/generate_pdf.py
#!/usr/bin/env python3
"""
Knee Rehabilitation Protocol PDF Generator
Uses reportlab for PDF creation and matplotlib for charts.
"""
import matplotlib
matplotlib.use('Agg')
import matplotlib.pyplot as plt
import matplotlib.patches as mpatches
import numpy as np
import os
import io
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import mm, cm
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_RIGHT, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
PageBreak, HRFlowable, Image, KeepTogether
)
from reportlab.platypus.flowables import Flowable
from reportlab.lib.colors import HexColor, white, black
# ── Colour palette ──────────────────────────────────────────────────────────
C_DARK_BLUE = HexColor('#1A3A5C')
C_MID_BLUE = HexColor('#2B6CB0')
C_LIGHT_BLUE = HexColor('#EBF4FF')
C_ACCENT = HexColor('#E53E3E')
C_TEAL = HexColor('#2C7A7B')
C_GREEN = HexColor('#276749')
C_LIGHT_GREEN = HexColor('#F0FFF4')
C_AMBER = HexColor('#C05621')
C_LIGHT_AMBER = HexColor('#FFFAF0')
C_PURPLE = HexColor('#553C9A')
C_LIGHT_GREY = HexColor('#F7FAFC')
C_MID_GREY = HexColor('#718096')
C_BORDER = HexColor('#CBD5E0')
OUTPUT_DIR = '/home/daytona/workspace/knee-rehab-pdf'
os.makedirs(OUTPUT_DIR, exist_ok=True)
# ── Custom styles ────────────────────────────────────────────────────────────
def build_styles():
base = getSampleStyleSheet()
styles = {}
styles['cover_title'] = ParagraphStyle(
'cover_title', parent=base['Title'],
fontSize=32, textColor=white, leading=40,
spaceAfter=10, alignment=TA_CENTER, fontName='Helvetica-Bold'
)
styles['cover_sub'] = ParagraphStyle(
'cover_sub', parent=base['Normal'],
fontSize=14, textColor=HexColor('#BEE3F8'), leading=20,
alignment=TA_CENTER, fontName='Helvetica'
)
styles['cover_footer'] = ParagraphStyle(
'cover_footer', parent=base['Normal'],
fontSize=10, textColor=HexColor('#90CDF4'),
alignment=TA_CENTER, fontName='Helvetica-Oblique'
)
styles['section_header'] = ParagraphStyle(
'section_header', parent=base['Heading1'],
fontSize=16, textColor=white, leading=22,
spaceBefore=6, spaceAfter=8,
fontName='Helvetica-Bold', alignment=TA_LEFT
)
styles['subsection'] = ParagraphStyle(
'subsection', parent=base['Heading2'],
fontSize=12, textColor=C_DARK_BLUE, leading=16,
spaceBefore=10, spaceAfter=4,
fontName='Helvetica-Bold'
)
styles['body'] = ParagraphStyle(
'body', parent=base['Normal'],
fontSize=9.5, textColor=HexColor('#2D3748'), leading=14,
spaceAfter=4, fontName='Helvetica', alignment=TA_JUSTIFY
)
styles['body_bold'] = ParagraphStyle(
'body_bold', parent=base['Normal'],
fontSize=9.5, textColor=C_DARK_BLUE, leading=14,
spaceAfter=4, fontName='Helvetica-Bold'
)
styles['bullet'] = ParagraphStyle(
'bullet', parent=base['Normal'],
fontSize=9.5, textColor=HexColor('#2D3748'), leading=14,
spaceAfter=3, leftIndent=14, firstLineIndent=-10,
fontName='Helvetica'
)
styles['table_header'] = ParagraphStyle(
'table_header', parent=base['Normal'],
fontSize=9, textColor=white, leading=12,
fontName='Helvetica-Bold', alignment=TA_CENTER
)
styles['table_cell'] = ParagraphStyle(
'table_cell', parent=base['Normal'],
fontSize=8.5, textColor=HexColor('#2D3748'), leading=12,
fontName='Helvetica'
)
styles['table_cell_bold'] = ParagraphStyle(
'table_cell_bold', parent=base['Normal'],
fontSize=8.5, textColor=C_DARK_BLUE, leading=12,
fontName='Helvetica-Bold'
)
styles['phase_label'] = ParagraphStyle(
'phase_label', parent=base['Normal'],
fontSize=11, textColor=white, leading=14,
fontName='Helvetica-Bold', alignment=TA_CENTER
)
styles['caption'] = ParagraphStyle(
'caption', parent=base['Normal'],
fontSize=8, textColor=C_MID_GREY, leading=11,
fontName='Helvetica-Oblique', alignment=TA_CENTER
)
styles['prom_name'] = ParagraphStyle(
'prom_name', parent=base['Normal'],
fontSize=9, textColor=C_DARK_BLUE, leading=12,
fontName='Helvetica-Bold'
)
styles['footer_text'] = ParagraphStyle(
'footer_text', parent=base['Normal'],
fontSize=8, textColor=C_MID_GREY, leading=10,
fontName='Helvetica', alignment=TA_CENTER
)
return styles
STYLES = build_styles()
# ── Helper: coloured section banner ─────────────────────────────────────────
def section_banner(title, bg_color=C_DARK_BLUE):
data = [[Paragraph(title, STYLES['section_header'])]]
t = Table(data, colWidths=[170*mm])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), bg_color),
('LEFTPADDING', (0,0), (-1,-1), 10),
('RIGHTPADDING', (0,0), (-1,-1), 10),
('TOPPADDING', (0,0), (-1,-1), 7),
('BOTTOMPADDING',(0,0), (-1,-1), 7),
('ROUNDEDCORNERS', [4,4,4,4]),
]))
return t
# ── Helper: phase badge ──────────────────────────────────────────────────────
def phase_badge(text, color):
data = [[Paragraph(text, STYLES['phase_label'])]]
t = Table(data, colWidths=[170*mm])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), color),
('LEFTPADDING', (0,0), (-1,-1), 8),
('RIGHTPADDING', (0,0), (-1,-1), 8),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING',(0,0), (-1,-1), 5),
]))
return t
# ── Helper: exercise table ───────────────────────────────────────────────────
def exercise_table(headers, rows, col_widths, row_colors=None):
header_row = [Paragraph(h, STYLES['table_header']) for h in headers]
data = [header_row]
for i, row in enumerate(rows):
styled = []
for j, cell in enumerate(row):
if j == 0:
styled.append(Paragraph(str(cell), STYLES['table_cell_bold']))
else:
styled.append(Paragraph(str(cell), STYLES['table_cell']))
data.append(styled)
t = Table(data, colWidths=col_widths, repeatRows=1)
style_cmds = [
('BACKGROUND', (0,0), (-1,0), C_DARK_BLUE),
('ROWBACKGROUNDS',(0,1),(-1,-1), [C_LIGHT_GREY, white]),
('GRID', (0,0), (-1,-1), 0.4, C_BORDER),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING',(0,0), (-1,-1), 4),
('LINEABOVE', (0,1), (-1,1), 1, C_MID_BLUE),
]
t.setStyle(TableStyle(style_cmds))
return t
# ── CHART 1: Exercise Progression Overview (Gantt-style) ───────────────────
def make_progression_chart():
fig, ax = plt.subplots(figsize=(11, 5.5))
fig.patch.set_facecolor('#FAFAFA')
ax.set_facecolor('#FAFAFA')
phases = [
('Phase 1: Acute\n(Weeks 1-2)', 0, 2, '#C53030'),
('Phase 2: Sub-acute\n(Weeks 3-6)', 2, 6, '#C05621'),
('Phase 3: Strengthening\n(Wks 7-12)',6, 12, '#276749'),
('Phase 4: Functional\n(Weeks 12+)', 12, 20, '#1A3A5C'),
]
exercises = [
('Ankle Pumps / Isometrics', 0, 6, '#FC8181'),
('Straight Leg Raises', 0, 8, '#FC8181'),
('Heel Slides / ROM exercises', 0, 12, '#F6AD55'),
('Mini Squats (0-30 deg)', 2, 12, '#F6AD55'),
('Step-ups / TKE', 4, 16, '#68D391'),
('Stationary Cycling', 2, 20, '#68D391'),
('Leg Press / Full Squats', 6, 20, '#4299E1'),
('Single-Leg Balance', 6, 20, '#4299E1'),
('Nordic Hamstring Curls', 8, 20, '#9F7AEA'),
('Lunges / Bulgarian Splits', 8, 20, '#9F7AEA'),
('Plyometrics / Agility Drills',12, 20, '#1A3A5C'),
('Return-to-Sport Drills', 14, 20, '#1A3A5C'),
]
n = len(exercises)
bar_height = 0.52
# Phase background shading
phase_colors_bg = ['#FFF5F5', '#FFFAF0', '#F0FFF4', '#EBF4FF']
phase_bounds = [(0,2), (2,6), (6,12), (12,20)]
for (start, end), bg in zip(phase_bounds, phase_colors_bg):
ax.axvspan(start, end, alpha=0.45, color=bg, zorder=0)
# Exercise bars
for i, (name, start, end, color) in enumerate(exercises):
y = n - 1 - i
ax.barh(y, end - start, left=start, height=bar_height,
color=color, alpha=0.88, edgecolor='white', linewidth=0.8, zorder=2)
# Label inside bar if wide enough
bar_len = end - start
if bar_len >= 3:
ax.text(start + bar_len/2, y, name,
va='center', ha='center', fontsize=7.2,
color='white', fontweight='bold', zorder=3)
else:
ax.text(end + 0.1, y, name,
va='center', ha='left', fontsize=7.2,
color='#2D3748', zorder=3)
# Phase header bars at top
for (name, start, end, color) in phases:
width = end - start
ax.barh(n + 0.5, width, left=start, height=0.7,
color=color, alpha=0.92, edgecolor='white', linewidth=1, zorder=2)
ax.text(start + width/2, n + 0.5, name,
va='center', ha='center', fontsize=7.5,
color='white', fontweight='bold', zorder=3)
# Vertical week markers
for w in range(0, 21, 2):
ax.axvline(x=w, color='#CBD5E0', linewidth=0.5, linestyle='--', zorder=1)
ax.set_xlim(0, 20)
ax.set_ylim(-0.7, n + 1.2)
ax.set_xlabel('Weeks', fontsize=10, color='#2D3748', fontweight='bold')
ax.set_xticks(range(0, 21, 2))
ax.set_xticklabels([f'Wk {w}' for w in range(0, 21, 2)], fontsize=8)
ax.set_yticks([])
ax.set_title('Knee Rehabilitation - Exercise Progression Timeline', fontsize=13,
fontweight='bold', color='#1A3A5C', pad=10)
ax.spines['top'].set_visible(False)
ax.spines['right'].set_visible(False)
ax.spines['left'].set_visible(False)
ax.tick_params(axis='x', colors='#4A5568')
plt.tight_layout()
buf = io.BytesIO()
plt.savefig(buf, format='png', dpi=160, bbox_inches='tight',
facecolor='#FAFAFA')
plt.close(fig)
buf.seek(0)
return buf
# ── CHART 2: PROM Score Progression ──────────────────────────────────────────
def make_prom_chart():
fig, axes = plt.subplots(1, 2, figsize=(11, 4.5))
fig.patch.set_facecolor('#FAFAFA')
weeks = [0, 6, 12, 24, 52]
labels = ['Baseline', 'Wk 6', 'Wk 12', 'Wk 24\n(6 mo)', 'Wk 52\n(1 yr)']
# Chart A - KOOS Subscales
ax = axes[0]
ax.set_facecolor('#FAFAFA')
koos_data = {
'Pain': [35, 52, 65, 78, 85],
'Symptoms': [38, 50, 62, 74, 80],
'ADL': [40, 55, 68, 80, 88],
'Sport/Rec': [20, 32, 48, 64, 75],
'QoL': [18, 30, 45, 62, 72],
}
palette = ['#E53E3E','#DD6B20','#38A169','#3182CE','#805AD5']
for (label, vals), color in zip(koos_data.items(), palette):
ax.plot(weeks, vals, marker='o', markersize=5, linewidth=2,
color=color, label=label)
ax.fill_between(weeks, vals, alpha=0.08, color=color)
ax.axhline(y=70, color='#718096', linewidth=1, linestyle=':', alpha=0.7)
ax.text(50.5, 71, 'Good outcome\nthreshold (70)', fontsize=7,
color='#718096', va='bottom')
ax.set_title('KOOS Subscale Progression', fontsize=11,
fontweight='bold', color='#1A3A5C')
ax.set_xlabel('Weeks post-treatment', fontsize=9)
ax.set_ylabel('Score (0-100, higher = better)', fontsize=9)
ax.set_xlim(-2, 55)
ax.set_ylim(0, 105)
ax.set_xticks(weeks)
ax.set_xticklabels(labels, fontsize=8)
ax.legend(fontsize=7.5, loc='upper left', framealpha=0.85)
ax.spines['top'].set_visible(False)
ax.spines['right'].set_visible(False)
ax.grid(axis='y', linestyle='--', alpha=0.4)
# Chart B - Strength Recovery (LSI %)
ax2 = axes[1]
ax2.set_facecolor('#FAFAFA')
weeks2 = [0, 6, 12, 18, 24, 36]
labels2 = ['Pre-op','Wk 6','Wk 12','Wk 18','Wk 24','Wk 36']
quad_lsi = [100, 55, 65, 74, 82, 90]
hamst_lsi = [100, 65, 72, 80, 87, 92]
thresh = [90] * len(weeks2)
ax2.plot(weeks2, quad_lsi, marker='s', markersize=5, linewidth=2,
color='#3182CE', label='Quadriceps LSI %')
ax2.plot(weeks2, hamst_lsi, marker='^', markersize=5, linewidth=2,
color='#38A169', label='Hamstring LSI %')
ax2.plot(weeks2, thresh, linewidth=1.5, linestyle='--',
color='#E53E3E', label='Return-to-sport threshold (90%)')
ax2.fill_between(weeks2, quad_lsi, 90,
where=[q < 90 for q in quad_lsi],
alpha=0.12, color='#3182CE')
ax2.set_title('Limb Symmetry Index (LSI) - ACL Rehab', fontsize=11,
fontweight='bold', color='#1A3A5C')
ax2.set_xlabel('Weeks post-reconstruction', fontsize=9)
ax2.set_ylabel('LSI % vs. contralateral limb', fontsize=9)
ax2.set_xlim(-2, 38)
ax2.set_ylim(40, 105)
ax2.set_xticks(weeks2)
ax2.set_xticklabels(labels2, fontsize=8)
ax2.legend(fontsize=7.5, loc='lower right', framealpha=0.85)
ax2.spines['top'].set_visible(False)
ax2.spines['right'].set_visible(False)
ax2.grid(axis='y', linestyle='--', alpha=0.4)
plt.tight_layout(pad=2)
buf = io.BytesIO()
plt.savefig(buf, format='png', dpi=160, bbox_inches='tight',
facecolor='#FAFAFA')
plt.close(fig)
buf.seek(0)
return buf
# ── CHART 3: Load Progression Pyramid ────────────────────────────────────────
def make_load_pyramid():
fig, ax = plt.subplots(figsize=(7, 5))
fig.patch.set_facecolor('#FAFAFA')
ax.set_facecolor('#FAFAFA')
ax.set_xlim(0, 10)
ax.set_ylim(0, 10)
ax.axis('off')
ax.set_title('Exercise Load Progression Pyramid', fontsize=12,
fontweight='bold', color='#1A3A5C', pad=8)
levels = [
(1.0, 8.0, 8.0, '#E53E3E', 'RETURN TO SPORT\nAgilty, Plyometrics, Cutting drills'),
(1.5, 6.8, 7.0, '#DD6B20', 'FUNCTIONAL TRAINING\nSingle-leg press, Lunges, Step-downs'),
(2.0, 5.6, 6.0, '#D69E2E', 'STRENGTHENING\nSquats, Leg press, Nordic curls'),
(2.5, 4.4, 5.0, '#38A169', 'NEUROMUSCULAR CONTROL\nBalance, TKE, Mini-squats'),
(3.0, 3.2, 4.0, '#3182CE', 'EARLY MOBILITY\nHeel slides, Cycling, Quad sets'),
(3.5, 2.0, 3.0, '#1A3A5C', 'FOUNDATION\nIsometrics, SLR, Ankle pumps, Ice/Elevation'),
]
for (left, y, width, color, text) in levels:
bar_w = width
rect = mpatches.FancyBboxPatch(
(5 - bar_w/2, y - 0.55), bar_w, 0.95,
boxstyle='round,pad=0.05', linewidth=0,
facecolor=color, alpha=0.9
)
ax.add_patch(rect)
lines = text.split('\n')
ax.text(5, y, lines[0], ha='center', va='center',
fontsize=7.5, color='white', fontweight='bold')
if len(lines) > 1:
ax.text(5, y - 0.25, lines[1], ha='center', va='center',
fontsize=6.5, color='#E2E8F0')
# Arrow
ax.annotate('', xy=(0.5, 9.2), xytext=(0.5, 1.5),
arrowprops=dict(arrowstyle='->', color='#718096', lw=1.5))
ax.text(0.1, 5.5, 'PROGRESSION', fontsize=7, color='#718096',
rotation=90, va='center', ha='center')
plt.tight_layout()
buf = io.BytesIO()
plt.savefig(buf, format='png', dpi=160, bbox_inches='tight',
facecolor='#FAFAFA')
plt.close(fig)
buf.seek(0)
return buf
# ── CHART 4: PROM Selection Matrix (heatmap) ─────────────────────────────────
def make_prom_matrix():
conditions = ['OA\nConservative', 'Post-\nTKR/UKR', 'ACL\nRehab',
'Meniscal\nInjury', 'PFPS']
proms = ['KOOS', 'WOMAC', 'Oxford KS', 'Lysholm', 'IKDC', 'Tegner',
'VAS/NRS', 'ACL-RSI', 'SF-36']
# 1=Recommended, 0.5=Useful, 0=Not applicable
matrix = np.array([
[1, 1, 0.5, 1, 0.5], # KOOS
[1, 0.5, 0, 0, 0.5], # WOMAC
[0.5, 1, 0, 0, 0 ], # Oxford KS
[0, 0, 1, 1, 0.5], # Lysholm
[0, 0, 1, 1, 1 ], # IKDC
[0, 0, 1, 0.5, 0.5], # Tegner
[1, 1, 1, 1, 1 ], # VAS/NRS
[0, 0, 1, 0, 0 ], # ACL-RSI
[0.5, 1, 0.5, 0.5, 0.5], # SF-36
])
fig, ax = plt.subplots(figsize=(8, 5.5))
fig.patch.set_facecolor('#FAFAFA')
from matplotlib.colors import LinearSegmentedColormap
cmap = LinearSegmentedColormap.from_list('rehab',
['#FFFFFF', '#BEE3F8', '#2B6CB0'])
im = ax.imshow(matrix, cmap=cmap, aspect='auto', vmin=0, vmax=1)
ax.set_xticks(range(len(conditions)))
ax.set_xticklabels(conditions, fontsize=9)
ax.set_yticks(range(len(proms)))
ax.set_yticklabels(proms, fontsize=9, fontweight='bold')
for i in range(len(proms)):
for j in range(len(conditions)):
val = matrix[i, j]
if val == 1:
txt, col = 'REC', 'white'
elif val == 0.5:
txt, col = 'USE', '#1A3A5C'
else:
txt, col = '-', '#CBD5E0'
ax.text(j, i, txt, ha='center', va='center',
fontsize=8, fontweight='bold', color=col)
# Legend patches
from matplotlib.patches import Patch
legend_elements = [
Patch(facecolor='#2B6CB0', label='Recommended (REC)'),
Patch(facecolor='#BEE3F8', label='Useful (USE)'),
Patch(facecolor='white', edgecolor='#CBD5E0', label='Not Applicable (-)'),
]
ax.legend(handles=legend_elements, loc='upper right', bbox_to_anchor=(1.38, 1.02),
fontsize=8, framealpha=0.9)
ax.set_title('PROM Selection Matrix by Clinical Condition', fontsize=11,
fontweight='bold', color='#1A3A5C', pad=8)
ax.tick_params(top=True, bottom=False, labeltop=True, labelbottom=False)
ax.tick_params(axis='x', which='both', length=0)
ax.tick_params(axis='y', which='both', length=0)
for spine in ax.spines.values():
spine.set_visible(False)
ax.set_xticks(np.arange(len(conditions)) - 0.5, minor=True)
ax.set_yticks(np.arange(len(proms)) - 0.5, minor=True)
ax.grid(which='minor', color='#E2E8F0', linewidth=0.8)
plt.tight_layout()
buf = io.BytesIO()
plt.savefig(buf, format='png', dpi=160, bbox_inches='tight',
facecolor='#FAFAFA')
plt.close(fig)
buf.seek(0)
return buf
# ══════════════════════════════════════════════════════════════════════════════
# COVER PAGE builder
# ══════════════════════════════════════════════════════════════════════════════
class CoverBackground(Flowable):
def draw(self):
w, h = A4
c = self.canv
# Deep blue gradient background
c.setFillColor(C_DARK_BLUE)
c.rect(0, 0, w, h, fill=1, stroke=0)
# Teal accent band
c.setFillColor(C_MID_BLUE)
c.rect(0, h*0.30, w, h*0.42, fill=1, stroke=0)
# Bottom dark band
c.setFillColor(HexColor('#0F2336'))
c.rect(0, 0, w, h*0.15, fill=1, stroke=0)
# Decorative circles
c.setFillColor(HexColor('#2C5282'))
c.circle(w*0.85, h*0.85, 80, fill=1, stroke=0)
c.setFillColor(HexColor('#2A4365'))
c.circle(w*0.1, h*0.2, 60, fill=1, stroke=0)
c.circle(w*0.9, h*0.1, 40, fill=1, stroke=0)
# ══════════════════════════════════════════════════════════════════════════════
# PAGE TEMPLATE with header/footer
# ══════════════════════════════════════════════════════════════════════════════
def on_page(canvas, doc):
canvas.saveState()
w, h = A4
page_num = doc.page
if page_num > 1:
# Header
canvas.setFillColor(C_DARK_BLUE)
canvas.rect(0, h - 22*mm, w, 22*mm, fill=1, stroke=0)
canvas.setFillColor(white)
canvas.setFont('Helvetica-Bold', 10)
canvas.drawString(15*mm, h - 14*mm,
'KNEE REHABILITATION PROTOCOL')
canvas.setFont('Helvetica', 9)
canvas.drawRightString(w - 15*mm, h - 14*mm,
'Clinical Reference Guide 2026')
# Footer
canvas.setFillColor(C_LIGHT_GREY)
canvas.rect(0, 0, w, 12*mm, fill=1, stroke=0)
canvas.setFillColor(C_DARK_BLUE)
canvas.rect(0, 12*mm, w, 0.5*mm, fill=1, stroke=0)
canvas.setFont('Helvetica', 8)
canvas.setFillColor(C_MID_GREY)
canvas.drawString(15*mm, 4*mm,
'Evidence-based protocol | EULAR 2024 | AAOS Guidelines | Ayurveda integrated')
canvas.drawRightString(w - 15*mm, 4*mm, f'Page {page_num}')
canvas.restoreState()
# ══════════════════════════════════════════════════════════════════════════════
# MAIN BUILD FUNCTION
# ══════════════════════════════════════════════════════════════════════════════
def build_pdf():
output_path = os.path.join(OUTPUT_DIR, 'Knee_Rehabilitation_Protocol.pdf')
doc = SimpleDocTemplate(
output_path,
pagesize=A4,
leftMargin=18*mm,
rightMargin=18*mm,
topMargin=28*mm,
bottomMargin=18*mm,
title='Knee Rehabilitation Protocol',
author='Orris Clinical Reference',
subject='Knee Rehabilitation, PROMs, Ayurveda'
)
story = []
PW = 174*mm # usable page width
# ── PAGE 1: COVER ─────────────────────────────────────────────────────────
story.append(Spacer(1, 55*mm))
cover_title_data = [[Paragraph(
'KNEE JOINT<br/>REHABILITATION PROTOCOL',
STYLES['cover_title']
)]]
ct = Table(cover_title_data, colWidths=[PW])
ct.setStyle(TableStyle([('BACKGROUND',(0,0),(-1,-1),C_DARK_BLUE)]))
story.append(ct)
story.append(Spacer(1, 8*mm))
story.append(Paragraph(
'Comprehensive Clinical Reference: Anatomy | Examination | Investigations<br/>'
'Rehabilitation Exercises | PROMs | Treatment | Ayurveda Integration',
STYLES['cover_sub']
))
story.append(Spacer(1, 18*mm))
# Info boxes on cover
info_rows = [[
Paragraph('<b>Evidence Base</b><br/>AAOS 2023 | EULAR 2024<br/>Cochrane 2024', STYLES['table_cell']),
Paragraph('<b>Target Conditions</b><br/>OA | ACL | Meniscal<br/>PFPS | TKR/UKR', STYLES['table_cell']),
Paragraph('<b>Includes</b><br/>KOOS | WOMAC | OKS<br/>Lysholm | IKDC | ACL-RSI', STYLES['table_cell']),
Paragraph('<b>Ayurveda</b><br/>Janu Basti | Matra Basti<br/>Herbs | Panchakarma', STYLES['table_cell']),
]]
info_t = Table(info_rows, colWidths=[PW/4]*4)
info_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), HexColor('#EBF4FF')),
('BOX', (0,0), (-1,-1), 1, C_MID_BLUE),
('INNERGRID', (0,0), (-1,-1), 0.5, C_BORDER),
('TOPPADDING', (0,0), (-1,-1), 8),
('BOTTOMPADDING',(0,0),(-1,-1), 8),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
]))
story.append(info_t)
story.append(Spacer(1, 10*mm))
story.append(Paragraph('Generated July 2026 | Orris Clinical Reference System', STYLES['cover_footer']))
story.append(Spacer(1, 6*mm))
story.append(Paragraph(
'For clinical use by qualified healthcare professionals. Not a substitute for individual patient assessment.',
STYLES['caption']
))
story.append(PageBreak())
# ── PAGE 2-3: PHASE OVERVIEW + PROGRESSION CHART ─────────────────────────
story.append(section_banner('REHABILITATION PHASES - OVERVIEW'))
story.append(Spacer(1, 4*mm))
# Phase cards
phases_info = [
(C_ACCENT, 'PHASE 1: ACUTE / PROTECTION', 'Weeks 1-2',
['Control pain and swelling (RICE principle)',
'Restore early range of motion (ROM)',
'Prevent quadriceps atrophy',
'Minimize effusion through elevation + ice (20 min, 4-6x/day)',
'Weight-bearing: partial (crutches post-op) or as tolerated (OA)']),
(C_AMBER, 'PHASE 2: SUB-ACUTE / MOBILITY', 'Weeks 3-6',
['Restore full passive ROM (0-135 deg)',
'Begin closed-chain weight-bearing exercises',
'Normalize gait pattern',
'Initiate proprioception and neuromuscular training',
'Stationary cycling: low resistance for ROM']),
(C_GREEN, 'PHASE 3: STRENGTHENING', 'Weeks 7-12',
['Progressive resistance training for quads, hamstrings, glutes',
'Closed and open kinetic chain exercises',
'Advanced balance and proprioception (unstable surfaces)',
'Aquatic exercise (especially OA/TKR patients)',
'Nordic hamstring curls, leg press, lunges introduced']),
(C_DARK_BLUE,'PHASE 4: FUNCTIONAL / RETURN', 'Week 12+',
['Sport-specific training and agility drills (ACL patients)',
'Plyometrics when LSI >85% and pain-free',
'Criteria-based return-to-sport (LSI >90%, KOOS-sports >90%)',
'Psychological readiness assessed (ACL-RSI >/= 90)',
'OA patients: maintain exercise as lifestyle activity']),
]
for color, title, timing, bullets in phases_info:
header_data = [[
Paragraph(title, STYLES['phase_label']),
Paragraph(timing, ParagraphStyle('timing', parent=STYLES['phase_label'],
alignment=TA_RIGHT))
]]
ht = Table(header_data, colWidths=[PW*0.7, PW*0.3])
ht.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), color),
('LEFTPADDING', (0,0), (-1,-1), 8),
('RIGHTPADDING', (0,0), (-1,-1), 8),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING',(0,0), (-1,-1), 5),
]))
bullet_paras = [Paragraph(f'<bullet>\u2022</bullet> {b}', STYLES['bullet']) for b in bullets]
content_data = [[bullet_paras]]
ct2 = Table([[ht], bullet_paras[0:2] + bullet_paras[2:]], colWidths=[PW])
# Build as stacked
for bp in bullet_paras:
pass
story.append(KeepTogether([
ht,
Table([[Paragraph(f' \u2022 {b}', STYLES['bullet'])] for b in bullets],
colWidths=[PW],
style=TableStyle([
('BACKGROUND', (0,0), (-1,-1), C_LIGHT_GREY),
('LEFTPADDING', (0,0), (-1,-1), 14),
('RIGHTPADDING', (0,0), (-1,-1), 8),
('TOPPADDING', (0,0), (-1,-1), 2),
('BOTTOMPADDING',(0,0), (-1,-1), 2),
])),
Spacer(1, 3*mm),
]))
story.append(Spacer(1, 4*mm))
story.append(Paragraph('Exercise Progression Timeline Chart', STYLES['subsection']))
chart1_buf = make_progression_chart()
img1 = Image(chart1_buf, width=PW, height=PW*0.45)
story.append(img1)
story.append(Paragraph(
'Figure 1. Gantt-style exercise progression chart showing introduction and continuation of exercises across rehabilitation phases.',
STYLES['caption']
))
story.append(PageBreak())
# ── PAGE 4: PHASE 1 & 2 EXERCISE TABLES ───────────────────────────────────
story.append(section_banner('PHASE 1 & 2 - DETAILED EXERCISE PRESCRIPTION', C_ACCENT))
story.append(Spacer(1, 3*mm))
story.append(phase_badge('PHASE 1: ACUTE / PROTECTION | Weeks 1-2', C_ACCENT))
story.append(Spacer(1, 2*mm))
p1_headers = ['Exercise', 'Technique', 'Sets x Reps', 'Frequency', 'Precaution']
p1_rows = [
['Ankle Pumps', 'Flex/point foot rhythmically; supine', '3 x 20', 'Hourly', 'None'],
['Quad Sets (Isometric)', 'Press back of knee to bed; tighten quads; hold 5s', '3 x 10', '4-6x/day', 'Pain-free only'],
['Inner Range Quads', 'Towel roll under knee (30 deg); actively extend', '3 x 10', '3x/day', 'Avoid if swollen'],
['Straight Leg Raise (SLR)', 'Quads contracted; lift to 45 deg; 4 planes', '3 x 10', '3x/day', 'No lag allowed'],
['Heel Slides', 'Supine; slide heel toward buttock; ROM only', '3 x 10', '3x/day', 'No forcing'],
['Supine Hip Abduction', 'Straight leg; abduct to 40 deg; side-lying alt.', '3 x 12', '2x/day', 'None'],
['Terminal Knee Extension (TKE)', 'Band behind knee; extend from 30 to 0 deg', '3 x 15', '3x/day', 'ACL: avoid early post-op'],
['Patella Mobilization', 'Passive superior-inferior + medial-lateral glides', '2 min', '2x/day', 'Post-op only after wound healed'],
['Cryotherapy', 'Ice pack over towel; knee elevated', '20 min', '4-6x/day', 'No direct skin contact'],
]
p1_cols = [38*mm, 50*mm, 25*mm, 25*mm, 32*mm]
story.append(exercise_table(p1_headers, p1_rows, p1_cols))
story.append(Spacer(1, 4*mm))
story.append(phase_badge('PHASE 2: SUB-ACUTE / MOBILITY | Weeks 3-6', C_AMBER))
story.append(Spacer(1, 2*mm))
p2_rows = [
['Mini Squats (0-30 deg)', 'Bilateral; hands on surface for balance; progress to unsupported', '3 x 15', 'Daily', 'No valgus collapse'],
['Step-Ups (Forward)', 'Low step (5 cm); controlled ascent/descent; progress height', '3 x 10 each', 'Daily', 'Pain < 3/10'],
['Stationary Cycling', 'Low resistance; saddle high; pedal smoothly', '15-20 min', '5x/week', 'Stop if sharp pain'],
['Calf Raises (Standing)', 'Bilateral; progress to single-leg', '3 x 15', 'Daily', 'None'],
['Hip Abduction (Resistance Band)', 'Standing; band at ankle; lift laterally', '3 x 15', '3x/week', 'None'],
['VMO Emphasis Squat', 'Feet 30 deg external rotation; drop into squat focusing medial quad', '3 x 12', 'Daily', 'Patella tracking'],
['Hamstring Curls (Prone)', 'Gravity or light resistance; full ROM', '3 x 12', '3x/week', 'ACL: check protocol'],
['Single-Leg Balance', 'Eyes open; 30s; progress to eyes closed / foam pad', '3 x 30s', 'Daily', 'Stand near wall'],
['Prone Hip Extension', 'Squeeze glutes; lift leg 15 cm; hold 3s', '3 x 12', '3x/week', 'None'],
]
story.append(exercise_table(p1_headers, p2_rows, p1_cols))
story.append(Spacer(1, 3*mm))
# Load pyramid
pyramid_buf = make_load_pyramid()
img_pyr = Image(pyramid_buf, width=PW*0.55, height=PW*0.40)
pyr_table = Table([[img_pyr]], colWidths=[PW])
pyr_table.setStyle(TableStyle([('ALIGN',(0,0),(-1,-1),'CENTER')]))
story.append(pyr_table)
story.append(Paragraph(
'Figure 2. Exercise load progression pyramid - build from the base upwards.',
STYLES['caption']
))
story.append(PageBreak())
# ── PAGE 5: PHASE 3 & 4 EXERCISE TABLES ───────────────────────────────────
story.append(section_banner('PHASE 3 & 4 - STRENGTHENING & FUNCTIONAL RETURN', C_GREEN))
story.append(Spacer(1, 3*mm))
story.append(phase_badge('PHASE 3: STRENGTHENING | Weeks 7-12', C_GREEN))
story.append(Spacer(1, 2*mm))
p3_rows = [
['Full Squats (0-90 deg)', 'Bodyweight to loaded; feet shoulder-width; neutral spine', '3-4 x 12', '3x/week', 'Valgus watch'],
['Leg Press', 'Low seat; full ROM; progressive load increase', '3-4 x 12', '3x/week', 'No locking out'],
['Lunges (Forward/Lateral)', 'Controlled descent; knee tracks over 2nd toe', '3 x 10 each', '3x/week', 'Pain-free'],
['Wall Squats (Isometric)', 'Sustained hold at 60-90 deg; VMO focused', '3 x 30-60s', 'Daily', 'Bilateral only initially'],
['Nordic Hamstring Curls', 'Eccentric; partner holds ankles; slow lowering', '3 x 6-8', '2x/week', 'High intensity - progress carefully'],
['Aquatic Exercises', 'Pool walking; pool squats; resistance with floats', '20-30 min', '3x/week', 'Wound healed (post-op)'],
['Lateral Band Walks', 'Band at ankles; side-step maintaining hip neutral', '3 x 15 each', '3x/week', 'None'],
['Step-Downs (Eccentric)', '20 cm step; single-leg controlled descent; hip neutral', '3 x 8-10 each', '3x/week', 'Pain < 3/10'],
['Open Chain Knee Extension', '90 to 40 deg only (protect ACL graft); resistance machine', '3 x 12', '3x/week', 'ACL: no full extension'],
]
story.append(exercise_table(p1_headers, p3_rows, p1_cols))
story.append(Spacer(1, 4*mm))
story.append(phase_badge('PHASE 4: FUNCTIONAL / RETURN TO SPORT | Week 12+', C_DARK_BLUE))
story.append(Spacer(1, 2*mm))
p4_rows = [
['Bulgarian Split Squats', 'Rear foot elevated; loaded; single-leg strength', '3 x 8 each', '3x/week', 'LSI >80% before starting'],
['Box Jumps', 'Two-foot takeoff and landing; soft knees; progress height', '3 x 8', '2x/week', 'ACL: >12 weeks post-op'],
['Lateral Bounding', 'Single-leg lateral hops; stick landing; 3-4 bounds', '3 x 5 each side', '2x/week', 'Land mechanics'],
['Agility Ladder Drills', 'In-out, lateral shuffle, carioca; speed progression', '3 x 30s', '3x/week', 'Pain-free only'],
['Change of Direction Drills', 'T-test, 5-10-5 shuttle; progress to unplanned', '3 x 3', '2x/week', 'ACL: 16+ weeks'],
['Running Progression', 'Walk 5 min -> jog 2 min alternating -> continuous jog', 'Protocol', '3x/week', 'No limp; no pain'],
['Perturbation Training', 'Therapist-applied unexpected perturbations on unstable surface', '10-15 min', '2x/week', 'Therapist supervised'],
['Sport-Specific Drills', 'Position-specific movements; reactive activities', 'As tolerated', '3x/week', 'Match intensity to sport'],
]
p4_cols = [42*mm, 50*mm, 23*mm, 22*mm, 33*mm]
story.append(exercise_table(p1_headers, p4_rows, p4_cols))
story.append(Spacer(1, 4*mm))
# Return-to-sport criteria box
rts_data = [[
Paragraph('<b>RETURN-TO-SPORT CRITERIA (ACL)</b>', STYLES['body_bold']),
],[
Paragraph(
u'\u2022 LSI \u2265 90% on single-leg hop tests (single, triple, crossover, 6-metre timed)\n'
u'\u2022 Hamstring:Quadriceps ratio \u2265 66%\n'
u'\u2022 Full pain-free ROM and no effusion\n'
u'\u2022 KOOS-Sports subscale \u2265 90\n'
u'\u2022 IKDC score \u2265 93\n'
u'\u2022 ACL-RSI score \u2265 90 (psychological readiness)\n'
u'\u2022 Minimum 9 months post-reconstruction (reduces re-rupture risk)',
STYLES['body']
)
]]
rts_t = Table(rts_data, colWidths=[PW])
rts_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,0), C_DARK_BLUE),
('BACKGROUND', (0,1), (0,1), C_LIGHT_BLUE),
('LEFTPADDING', (0,0), (-1,-1), 10),
('RIGHTPADDING', (0,0), (-1,-1), 10),
('TOPPADDING', (0,0), (-1,-1), 6),
('BOTTOMPADDING',(0,0), (-1,-1), 6),
('BOX', (0,0), (-1,-1), 1, C_MID_BLUE),
]))
story.append(rts_t)
story.append(PageBreak())
# ── PAGE 6: PROMs ─────────────────────────────────────────────────────────
story.append(section_banner('PATIENT-REPORTED OUTCOME MEASURES (PROMs)', C_TEAL))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(
'PROMs are standardized, patient-completed questionnaires that capture the patient\'s perspective on pain, '
'function, and quality of life. They are essential for monitoring rehabilitation progress, surgical decision-making, '
'and clinical audit. Administer at: Baseline, 6 weeks, 3 months, 6 months, and 12 months.',
STYLES['body']
))
story.append(Spacer(1, 3*mm))
prom_headers = ['PROM', 'Items', 'Subscales / Score Range', 'Best Use', 'MCID']
prom_rows = [
['KOOS', '42', '5 subscales; 0-100 each\n(higher = better)', 'OA, ACL, Meniscal, TKR', '8-10 pts'],
['KOOS-PS', '7', 'Physical function; 0-100', 'Quick functional screen', '8 pts'],
['WOMAC', '24', 'Pain/Stiffness/Function; 0-96', 'OA (hip & knee)', '10-15 pts'],
['Oxford Knee Score', '12', '0-48 (higher = better)', 'TKR/UKR pre & post-op', '5 pts'],
['Lysholm Scale', '8', '0-100; Excellent:95-100', 'Ligament / ACL injuries', '10 pts'],
['IKDC Subjective', '18', '0-100 (higher = better)', 'ACL, meniscal, ligament', '9-11 pts'],
['Tegner Activity', '1', '0-10 ordinal activity scale', 'Return-to-sport baseline', '1 level'],
['VAS / NRS Pain', '1', 'VAS 0-100mm / NRS 0-10', 'All conditions; daily monitoring', '1.5-2 pts'],
['ACL-RSI', '12', '0-100 psychological readiness', 'Post-ACL reconstruction', '17 pts'],
['SF-36 / SF-12', '36/12', '8 domains; PCS + MCS', 'General health-related QoL', '5-10 pts'],
['PROMIS', 'Adaptive', 'T-score (50 = population norm)', 'Research; multi-domain', 'Domain-specific'],
['KSS (Knee Society)', 'Dual', 'Knee score + Function score (0-100 each)', 'TKR outcomes', '10 pts'],
]
prom_cols = [32*mm, 12*mm, 48*mm, 42*mm, 20*mm]
story.append(exercise_table(prom_headers, prom_rows, prom_cols))
story.append(Spacer(1, 4*mm))
# PROM charts
story.append(Paragraph('PROM Outcome Tracking & PROM Selection Matrix', STYLES['subsection']))
prom_chart_buf = make_prom_chart()
img_prom = Image(prom_chart_buf, width=PW, height=PW*0.38)
story.append(img_prom)
story.append(Paragraph(
'Figure 3. Left: Expected KOOS subscale trajectory in OA rehabilitation over 12 months. '
'Right: ACL reconstruction - Limb Symmetry Index (LSI) recovery curve for quad and hamstring strength.',
STYLES['caption']
))
story.append(Spacer(1, 4*mm))
prom_matrix_buf = make_prom_matrix()
img_matrix = Image(prom_matrix_buf, width=PW*0.70, height=PW*0.42)
matrix_wrap = Table([[img_matrix]], colWidths=[PW])
matrix_wrap.setStyle(TableStyle([('ALIGN',(0,0),(-1,-1),'CENTER')]))
story.append(matrix_wrap)
story.append(Paragraph(
'Figure 4. PROM selection matrix - recommended instruments by clinical condition.',
STYLES['caption']
))
story.append(PageBreak())
# ── PAGE 7: TREATMENT INCLUDING AYURVEDA ──────────────────────────────────
story.append(section_banner('TREATMENT - CONVENTIONAL & AYURVEDA INTEGRATION', C_PURPLE))
story.append(Spacer(1, 3*mm))
# Conventional treatment table
story.append(Paragraph('Conventional Treatment by Evidence Level (AAOS 2023)', STYLES['subsection']))
conv_headers = ['Treatment', 'AAOS Strength', 'Recommendation']
conv_rows = [
['Patient Education Programs', '4-Star (Strong)', 'Recommended - first-line'],
['Exercise (supervised / unsupervised / aquatic)', '4-Star (Strong)', 'Recommended - cornerstone of management'],
['Self-Management Programs', '4-Star (Strong)', 'Recommended'],
['Topical NSAIDs (e.g., Diclofenac gel)', '4-Star (Strong)', 'Recommended - preferred over oral for local OA'],
['Oral NSAIDs (e.g., Ibuprofen, Naproxen)', '4-Star (Strong)', 'Recommended - with GI protection'],
['Sustained Weight Loss', '3-Star (Moderate)', 'Recommended - each 1 kg loss reduces load by ~4 kg'],
['Brace Treatment / Walking Aids', '3-Star (Moderate)', 'Recommended - offloader for medial OA'],
['Intraarticular Corticosteroids', '3-Star (Moderate)', 'Short-term relief only; max 3-4x/year'],
['PRP (Platelet-rich Plasma)', '2-Star (Limited)', 'May reduce pain; not standard care'],
['Acupuncture / TENS', '2-Star (Limited)', 'May improve pain; adjunct use'],
['Hyaluronic Acid (Viscosupplementation)', '3-Star AGAINST', 'NOT Recommended (AAOS)'],
['Arthroscopy with lavage/debridement', '4-Star AGAINST', 'NOT Recommended for OA'],
]
conv_cols = [58*mm, 32*mm, 80*mm]
story.append(exercise_table(conv_headers, conv_rows, conv_cols))
story.append(Spacer(1, 4*mm))
# Ayurveda section
story.append(section_banner('AYURVEDA INTEGRATION - JANU SANDHI (KNEE JOINT)', HexColor('#553C9A')))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(
'In Ayurveda, knee conditions are classified as <b>Sandhigatavata</b> (degenerative, Vata-dominant) '
'or <b>Amavata</b> (inflammatory, with Ama toxins). Treatment is individualized based on Dosha and disease stage.',
STYLES['body']
))
story.append(Spacer(1, 3*mm))
# Panchakarma table
story.append(Paragraph('Panchakarma Procedures for Janu Sandhi', STYLES['subsection']))
pk_headers = ['Procedure', 'Description', 'Oils / Materials', 'Duration', 'Evidence Level']
pk_rows = [
['Janu Basti', 'Warm medicated oil retained in dough ring over knee joint',
'Dhanwantara Taila, Ksheerabala Taila, Mahanarayan Taila',
'30-45 min; 7-14 days', 'Clinical studies; RCT in progress (2025)'],
['Matra Basti', 'Small-volume medicated oil enema (30-60 mL)',
'Ksheerabala Taila', 'Daily x 7-14 days', 'Promising RCTs; prime Vatavyadhi Rx'],
['Abhyanga', 'Therapeutic full or localized warm oil massage',
'Mahanarayan Taila, Ksheerabala Taila', '45-60 min', 'Standard pre-Panchakarma'],
['Swedana', 'Heat fomentation / herbal steam after Abhyanga',
'Herbal decoction steam', '15-20 min', 'Standard; relieves stiffness'],
['Patra Pinda Sweda', 'Herbal leaf bolus massage (hot compress)',
'Eranda, Nirgundi leaves, sesame oil', '30-45 min', 'Case series evidence'],
['Upanaha Sweda', 'Medicated poultice applied overnight to knee',
'Eranda, salt, sesame, vinegar paste', 'Overnight', 'Traditional; widely used'],
['Lepa (External paste)', 'Herbal anti-inflammatory paste applied topically',
'Guggulu-based formulations', '30-60 min', 'Traditional use'],
]
pk_cols = [28*mm, 40*mm, 40*mm, 24*mm, 38*mm]
story.append(exercise_table(pk_headers, pk_rows, pk_cols))
story.append(Spacer(1, 3*mm))
story.append(Paragraph('Internal Ayurvedic Medicines', STYLES['subsection']))
herb_headers = ['Formulation / Herb', 'Key Ingredients', 'Primary Action', 'Indication']
herb_rows = [
['Yogaraja Guggulu', 'Guggul, triphala, trikatu, sesame', 'Anti-inflammatory; Vata-pacifying', 'OA, joint pain, stiffness'],
['Trayodashanga Guggulu', 'Guggul + 13 herbs incl. ashwagandha', 'Analgesic; anti-rheumatic', 'Sandhigatavata'],
['Laksha Guggulu', 'Lac, guggul, ashwagandha, nagabala', 'Bone & cartilage regeneration', 'OA with bone loss; fractures'],
['Muktashukti Bhasma', 'Calcined pearl oyster shell', 'Calcium; anti-inflammatory', 'OA; osteoporosis component'],
['Shallaki (Boswellia serrata)', 'Boswellic acids (AKBA)', 'Inhibits 5-LOX; reduces cartilage breakdown', 'Strong RCT evidence for knee OA'],
['Ashwagandha (Withania somnifera)', 'Withanolides', 'Adaptogen; muscle/ligament strengthening', 'Stiffness, weakness, degeneration'],
['Guggulu (Commiphora mukul)', 'Guggulsterones', 'Anti-inflammatory; lipid-lowering', 'OA, rheumatoid arthritis'],
['Punarnava (Boerhavia diffusa)', 'Punarnavine', 'Anti-oedematous; renal support', 'Knee swelling/effusion'],
]
herb_cols = [42*mm, 40*mm, 42*mm, 46*mm]
story.append(exercise_table(herb_headers, herb_rows, herb_cols))
story.append(Spacer(1, 3*mm))
# Evidence note
evidence_data = [[
Paragraph('<b>Evidence Note:</b> A 2024 prospective study (Kshirsagar et al., Int J Res Orthop 2024) demonstrated '
'statistically significant improvement in <b>KOOS subscores</b> (pain, sport, function, QoL) over 90 days '
'with Panchakarma therapy (p<0.001). Boswellia serrata has multiple RCTs showing pain reduction in '
'knee OA comparable to NSAIDs. A multimodal RCT (Rai et al., JMIR Protocols 2025) is evaluating '
'Matra Basti + Janu Basti + Laksha Guggulu for primary knee OA.',
STYLES['body'])
]]
ev_t = Table(evidence_data, colWidths=[PW])
ev_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), HexColor('#FAF5FF')),
('BOX', (0,0), (-1,-1), 1, C_PURPLE),
('LEFTPADDING', (0,0), (-1,-1), 10),
('RIGHTPADDING', (0,0), (-1,-1), 10),
('TOPPADDING', (0,0), (-1,-1), 7),
('BOTTOMPADDING',(0,0), (-1,-1), 7),
]))
story.append(ev_t)
story.append(PageBreak())
# ── PAGE 8: MONITORING & REFERENCES ──────────────────────────────────────
story.append(section_banner('MONITORING, ASSESSMENT SCHEDULE & REFERENCES'))
story.append(Spacer(1, 3*mm))
story.append(Paragraph('Recommended PROM Assessment Schedule', STYLES['subsection']))
sched_headers = ['Timepoint', 'PROM(s)', 'Clinical Assessment', 'Notes']
sched_rows = [
['Baseline (pre-treatment)', 'KOOS / WOMAC / OKS\nVAS / Tegner', 'Full examination\nX-ray (weight-bearing)', 'Set goals; document deformity'],
['6 Weeks', 'KOOS / VAS / Lysholm', 'ROM; Effusion; Strength\nGait assessment', 'Phase 2 progression check'],
['3 Months (12 weeks)', 'KOOS / IKDC / VAS\nACL-RSI (ACL patients)', 'Single-leg squat; Hop tests\nLSI measurement', 'Phase 3-4 criteria check'],
['6 Months', 'KOOS / IKDC / OKS\nSF-12 / ACL-RSI', 'Functional assessment\nReturn-to-sport battery', 'Surgical review if indicated'],
['12 Months (1 Year)', 'All relevant PROMs\n+ Patient Satisfaction', 'Full functional review', 'Annual thereafter for OA'],
]
sched_cols = [32*mm, 42*mm, 50*mm, 46*mm]
story.append(exercise_table(sched_headers, sched_rows, sched_cols))
story.append(Spacer(1, 4*mm))
# Red flags
story.append(Paragraph('Red Flags - When to Stop Exercise & Seek Urgent Review', STYLES['subsection']))
rf_data = [
[Paragraph(u'\u26a0 RED FLAGS - STOP EXERCISE AND REFER URGENTLY', ParagraphStyle(
'rf', parent=STYLES['body_bold'], textColor=white, fontSize=10))],
[Paragraph(
u'\u2022 Sudden severe pain unrelated to exertion\n'
u'\u2022 Significant new swelling / hot red joint (consider septic arthritis / DVT)\n'
u'\u2022 Inability to weight-bear that was not present before\n'
u'\u2022 New neurological symptoms (numbness, tingling, weakness in foot)\n'
u'\u2022 Locking of the knee that cannot be resolved with gentle movement\n'
u'\u2022 Post-op: wound dehiscence, discharge, fever > 38.5 C\n'
u'\u2022 Chest pain, calf swelling or breathlessness (possible PE/DVT)',
STYLES['body']
)]
]
rf_t = Table(rf_data, colWidths=[PW])
rf_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,0), C_ACCENT),
('BACKGROUND', (0,1), (0,1), HexColor('#FFF5F5')),
('BOX', (0,0), (-1,-1), 1, C_ACCENT),
('LEFTPADDING', (0,0), (-1,-1), 10),
('RIGHTPADDING', (0,0), (-1,-1), 10),
('TOPPADDING', (0,0), (-1,-1), 6),
('BOTTOMPADDING',(0,0), (-1,-1), 6),
]))
story.append(rf_t)
story.append(Spacer(1, 4*mm))
# References
story.append(Paragraph('Key References', STYLES['subsection']))
refs = [
'1. Bailey & Love\'s Short Practice of Surgery, 28th Edition - Knee anatomy, examination, OA, ACL.',
'2. Miller\'s Review of Orthopaedics, 9th Edition - AAOS evidence-based guidelines for knee OA.',
'3. Rockwood & Green\'s Fractures in Adults, 10th Ed. - Medial and lateral knee anatomy.',
'4. Lawford BJ et al. Exercise for osteoarthritis of the knee. Cochrane Database Syst Rev. 2024 Dec.',
'5. Yan L et al. Comparative efficacy and safety of exercise modalities in knee OA. BMJ. 2025 Oct.',
'6. Moseng T et al. EULAR recommendations for non-pharmacological management of hip/knee OA: 2023 update. Ann Rheum Dis. 2024.',
'7. Rai AK et al. Efficacy of a Multimodal Ayurveda Regimen in knee OA. JMIR Protocols. 2025.',
'8. Kshirsagar J et al. Impact of Ayurvedic Panchakarma therapy on osteoarthritis (KOOS). Int J Res Orthop. 2024;10(6).',
'9. Collins NJ et al. Measures of knee function (KOOS, WOMAC, OKS, IKDC, Lysholm, Tegner). Arthritis Care Res. 2011.',
'10. AAOS. Management of Osteoarthritis of the Knee (Non-Arthroplasty) Evidence-Based CPG. 2023.',
]
for ref in refs:
story.append(Paragraph(ref, STYLES['bullet']))
story.append(Spacer(1, 4*mm))
# Disclaimer
disc_data = [[Paragraph(
'<b>Disclaimer:</b> This protocol is a clinical reference guide for use by qualified healthcare professionals. '
'All rehabilitation programs should be individualized to the patient\'s specific condition, fitness level, '
'and surgical status. This document does not replace clinical judgement or direct patient examination. '
'Ayurvedic treatments should be administered by qualified Ayurvedic practitioners.',
STYLES['caption']
)]]
disc_t = Table(disc_data, colWidths=[PW])
disc_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), C_LIGHT_GREY),
('BOX', (0,0), (-1,-1), 0.5, C_BORDER),
('LEFTPADDING', (0,0), (-1,-1), 8),
('RIGHTPADDING', (0,0), (-1,-1), 8),
('TOPPADDING', (0,0), (-1,-1), 6),
('BOTTOMPADDING',(0,0), (-1,-1), 6),
]))
story.append(disc_t)
# Build
doc.build(story, onFirstPage=on_page, onLaterPages=on_page)
print(f"PDF generated: {output_path}")
return output_path
if __name__ == '__main__':
path = build_pdf()
print(f"SUCCESS: {path}")
cd /home/daytona/workspace/knee-rehab-pdf && python3 generate_pdf.py 2>&1
ls -lh /home/daytona/workspace/knee-rehab-pdf/Knee_Rehabilitation_Protocol.pdf &…
Knee Rehabilitation Protocol
PDF Document · PDF
What's inside the PDF (13 pages, 420 KB)
| Page(s) | Content |
|---|---|
| 1 | Cover page with condition overview, evidence base summary, and Ayurveda note |
| 2-3 | 4-phase rehabilitation overview cards + Figure 1: Gantt-style exercise progression timeline (12 exercises mapped across 20 weeks) |
| 4 | Phase 1 & 2 detailed exercise prescription tables (sets/reps/frequency/precautions) + Figure 2: Load Progression Pyramid |
| 5 | Phase 3 & 4 exercise tables + Return-to-Sport criteria box (LSI, KOOS, ACL-RSI thresholds) |
| 6 | Full PROM reference table (12 PROMs) + Figure 3: KOOS subscale trajectory chart & LSI recovery curve + Figure 4: PROM selection matrix heatmap |
| 7 | Conventional treatment table (AAOS evidence star ratings) + Panchakarma procedures table + Ayurvedic internal medicines table + evidence note |
| 8 | PROM assessment schedule, Red Flag warnings, 10 key references, disclaimer |
Charts included
- Exercise Progression Timeline - Gantt chart showing when each exercise is introduced across Weeks 1-20
- Load Progression Pyramid - Visual pyramid from foundation exercises up to return-to-sport
- KOOS Subscale Trajectory - Expected improvement curve over 12 months
- Limb Symmetry Index (LSI) Chart - ACL rehab quadriceps and hamstring recovery with 90% return-to-sport threshold line
- PROM Selection Matrix - Heatmap showing recommended/useful/not-applicable for each PROM across OA, TKR, ACL, Meniscal, and PFPS
make a pdf together for both the above generate one & add images for the examination part
give it in a textform
KNEE JOINT — COMPLETE CLINICAL REFERENCE
Anatomy | Examination | Investigations | Conditions | Rehabilitation | PROMs | Treatment | Ayurveda
PART 1: ANATOMY
1.1 Joint Type & Compartments
- Static stabilizers: joint capsule, menisci, cruciate ligaments, collateral ligaments
- Dynamic stabilizers: quadriceps, hamstrings, popliteus, IT band, pes anserine muscles
1.2 Osseous Structures
1.3 Articular Cartilage
1.4 Menisci
1.5 Ligaments
Cruciate Ligaments (Intracapsular, Extrasynovial)
Collateral Ligaments
Posterolateral Corner (PLC)
1.6 Joint Capsule and Bursae
- Suprapatellar bursa: Located between the quadriceps tendon and femur; communicates freely with the joint cavity and fills with fluid in effusions.
- Prepatellar bursa: Lies over the anterior patella. Inflamed in "housemaid's knee" (chronic kneeling).
- Superficial infrapatellar bursa: Over the patellar tendon insertion. Inflamed in "clergyman's knee."
- Deep infrapatellar bursa: Between patellar tendon and tibia.
- Pes anserine bursa: Between the MCL and the pes anserine tendons on the medial tibia. Often inflamed in OA, especially obese patients.
- Baker's cyst (popliteal cyst): A posterior outpouching of the joint capsule, typically between the medial gastrocnemius and semimembranosus tendons. It communicates with the joint and fills with synovial fluid in the presence of chronic effusion or OA. May rupture, mimicking a DVT.
1.7 Extensor Mechanism
1.8 Dynamic Muscle Stabilizers
1.9 Biomechanics and Axes
PART 2: CLINICAL EXAMINATION
2.1 Look (Inspection)
Standing
Gait
- Antalgic gait: Short stance phase on the painful limb; the patient spends minimal time loading it. Classic in knee OA.
- Varus thrust: A dynamic collapse of the knee into greater varus during the stance phase as body weight is applied. Indicates medial compartment structural failure.
- High-stepping gait: Suggests foot drop from peroneal nerve palsy — a potential complication of lateral knee injury or proximal fibula fracture.
Supine
2.2 Feel (Palpation)
- Bulge (sweep) test for small effusions: Stroke fluid from the medial side up into the suprapatellar pouch with your hand, then push it inferiorly while watching the medial gutter. A ripple or refilling of the medial gutter indicates a small effusion (positive bulge sign).
- Patellar tap test for large effusions: Compress the suprapatellar pouch to push fluid under the patella, then tap the patella downward with one finger. A ballotable patella (bouncing sensation) confirms a tense large effusion.
2.3 Move (Range of Motion)
- Firm, springy end-feel in flexion = normal
- Hard end-feel = bony block (loose body, severe OA)
- Springy block = meniscal tear (bucket handle with locked knee)
- Empty end-feel = pain prevents full range testing
2.4 Special Tests
Tests for Effusion
- Bulge sign (sweep test): As described above. Detects small effusions (5-10 mL).
- Patellar tap: Detects large effusions (>30 mL).
Tests for Collateral Ligaments
Tests for the Anterior Cruciate Ligament
Tests for the Posterior Cruciate Ligament
Tests for the Menisci
Tests for the Patellofemoral Joint
PART 3: INVESTIGATIONS
3.1 Imaging
- AP (weight-bearing): assesses tibiofemoral compartments, overall alignment, Kellgren-Lawrence OA grading
- Lateral (30 degrees flexion): patellar height (Insall-Salvati ratio normal = 0.8-1.2), tibial posterior slope
- Skyline / Merchant / Axial view: patellofemoral compartment, trochlear shape, patellar tilt
- Rosenberg view (PA at 45 degrees): the most sensitive plain X-ray for early joint space narrowing
- Full-length (scanogram): mechanical axis assessment for osteotomy planning
3.2 Kellgren-Lawrence Grading of OA (Plain X-ray)
- Grade 0: Normal
- Grade 1: Doubtful narrowing; possible small osteophyte
- Grade 2: Definite osteophyte; possible joint space narrowing
- Grade 3: Multiple osteophytes; definite joint space narrowing; some sclerosis and possible deformity
- Grade 4: Large osteophytes; marked narrowing; severe sclerosis; definite bony deformity
3.3 Blood Investigations
3.4 Synovial Fluid Analysis
PART 4: COMMON CONDITIONS
4.1 Knee Osteoarthritis
4.2 ACL Injury
4.3 Meniscal Tears
4.4 Patellofemoral Pain Syndrome (PFPS)
4.5 Septic Arthritis
PART 5: REHABILITATION EXERCISES
5.1 Principles
5.2 Phase 1 — Acute / Protection Phase (Weeks 1-2)
5.3 Phase 2 — Sub-acute / Mobility Phase (Weeks 3-6)
5.4 Phase 3 — Strengthening Phase (Weeks 7-12)
5.5 Phase 4 — Functional / Return-to-Sport Phase (Week 12+)
5.6 Return-to-Sport Criteria (ACL Reconstruction)
- Limb Symmetry Index (LSI) of 90% or greater on all four hop tests
- Hamstring-to-quadriceps ratio of 66% or greater (isokinetic testing)
- Full pain-free range of motion with no effusion
- KOOS-Sports subscale score of 90 or greater
- IKDC Subjective Knee Form score of 93 or greater
- ACL-RSI (psychological readiness) score of 90 or greater
- Minimum 9 months from date of reconstruction (earlier return dramatically increases re-rupture risk)
PART 6: PATIENT-REPORTED OUTCOME MEASURES (PROMs)
KOOS — Knee Injury and Osteoarthritis Outcome Score
WOMAC — Western Ontario and McMaster Universities Osteoarthritis Index
Oxford Knee Score (OKS)
Lysholm Knee Scoring Scale
IKDC — International Knee Documentation Committee Subjective Knee Evaluation Form
Tegner Activity Scale
VAS / NRS Pain Scales
ACL-RSI — ACL Return to Sport after Injury Scale
SF-36 / SF-12
PROMIS — Patient-Reported Outcomes Measurement Information System
Recommended PROM Use by Condition
PART 7: TREATMENT
7.1 Non-Pharmacological Treatment (All Knee Conditions)
7.2 Pharmacological Treatment
7.3 Surgical Treatment
PART 8: AYURVEDA AND INTEGRATIVE TREATMENT
8.1 Ayurvedic Conceptual Framework
8.2 Panchakarma Procedures
Janu Basti
Matra Basti
Abhyanga
Swedana (Heat Fomentation)
Upanaha Sweda
Mridu Samshodhana (Gentle Cleansing)
8.3 Internal Ayurvedic Medicines
8.4 Dietary Recommendations (Ahara)
8.5 Evidence Summary
PART 9: INTEGRATED TREATMENT ALGORITHM
KEY REFERENCES
- Bailey & Love's Short Practice of Surgery, 28th Edition — Knee anatomy, clinical examination, OA, ACL, meniscal conditions.
- Miller's Review of Orthopaedics, 9th Edition — AAOS 2023 evidence-based guidelines for knee OA management.
- Rockwood & Green's Fractures in Adults, 10th Edition — Medial, lateral, and posterior knee anatomy.
- Lawford BJ et al. Exercise for osteoarthritis of the knee. Cochrane Database of Systematic Reviews. 2024.
- Yan L et al. Comparative efficacy and safety of exercise modalities in knee osteoarthritis: systematic review and network meta-analysis. BMJ. 2025.
- Moseng T et al. EULAR 2023 updated recommendations for the non-pharmacological core management of hip and knee OA. Annals of the Rheumatic Diseases. 2024.
- Rai AK et al. Efficacy of a Multimodal Ayurveda Regimen in the Management of Primary Knee Osteoarthritis: Protocol for an Open-Label RCT. JMIR Research Protocols. 2025.
- Kshirsagar J et al. Impact of Ayurvedic Panchakarma therapy on osteoarthritis (KOOS score). Int J Res Orthop. 2024;10(6):1364-1369.
- Collins NJ et al. Measures of knee function (KOOS, WOMAC, OKS, IKDC, Lysholm, Tegner). Arthritis Care & Research. 2011.
- Gibbs AJ et al. Recommendations for the management of hip and knee osteoarthritis: systematic review of CPGs. Osteoarthritis & Cartilage. 2023.
Spine
"spinal stenosis" AND "rehabilitation" AND "exercise"
spine Ayurveda treatment Kati Basti Greeva Basti Pristha Basti 2024 evidence
"low back pain"[MeSH Terms] AND "exercise therapy"[MeSH Terms]
"cervical spondylosis" AND "rehabilitation" AND "outcome"
spine rehabilitation exercises cervical lumbar physiotherapy protocol McKenzie Williams flexion 2024
THE SPINE — COMPLETE CLINICAL REFERENCE
All Regions: Cervical | Thoracic | Lumbar | Sacral
Anatomy | Examination | Investigations | Conditions | Rehabilitation | PROMs | Treatment | Ayurveda
PART 1: ANATOMY
1.1 Overview of the Vertebral Column
- Cervical lordosis: Concave posteriorly (normal 20-40 degrees)
- Thoracic kyphosis: Concave anteriorly (normal 20-45 degrees)
- Lumbar lordosis: Concave posteriorly (normal 40-60 degrees)
- Sacral kyphosis: Fixed kyphosis
1.2 A Typical Vertebra
1.3 Regional Vertebral Anatomy
Cervical Vertebrae (C1-C7)
Thoracic Vertebrae (T1-T12)
Lumbar Vertebrae (L1-L5)
1.4 The Intervertebral Disc
1.5 Ligaments of the Spine
1.6 The Spinal Canal and Neural Elements
1.7 Muscles of the Spine
- Iliocostalis (lateral column): runs from the sacrum to the ribs and cervical transverse processes
- Longissimus (intermediate column): the longest muscle; runs from the sacrum to the mastoid process
- Spinalis (medial column): runs between spinous processes
PART 2: CLINICAL EXAMINATION
2.1 General Principles
2.2 Examination of the Cervical Spine
Look
Feel
- Paraspinal muscles bilaterally for spasm, tenderness, or asymmetric tightness
- Spinous processes from C2 downward — tenderness at a specific level suggests local pathology; step-off indicates instability
- C7 (vertebra prominens) — the most prominent palpable process at the base of the neck
- Anterior structures: thyroid cartilage (C4-5), cricoid cartilage (C6), carotid arteries, lymph nodes, supraclavicular fossa
Move
| Movement | Normal Range |
|---|---|
| Flexion (chin to chest) | 45 degrees |
| Extension (look at ceiling) | 55 degrees |
| Lateral bending (ear to shoulder) | 45 degrees each side |
| Rotation (chin to shoulder) | 60-80 degrees each side |
Neurological Examination (Cervical)
| Level | Reflex | Motor | Sensation |
|---|---|---|---|
| C5 | Biceps jerk | Deltoid, biceps (shoulder abduction, elbow flexion) | Lateral upper arm |
| C6 | Brachioradialis jerk | Wrist extensors, biceps | Thumb and index finger |
| C7 | Triceps jerk | Triceps, wrist flexors, finger extensors | Middle finger |
| C8 | None reliable | Finger flexors, intrinsics | Ring and little finger |
| T1 | None reliable | Hand intrinsics | Medial forearm |
Special Tests (Cervical)
2.3 Examination of the Thoracic Spine
Look
Move
| Movement | Normal Range |
|---|---|
| Flexion | 20-45 degrees |
| Extension | 25-45 degrees |
| Lateral bending | 20-40 degrees each side |
| Rotation | 30-45 degrees each side (greatest in the thoracic spine) |
Special Tests (Thoracic)
2.4 Examination of the Lumbar Spine
Look
Feel
- Paraspinal muscles: Bilateral palpation for tenderness and spasm
- Spinous processes: Firm pressure over each — tenderness at a specific level. A "step" on palpation (one spinous process displaced anterior to the one above) indicates spondylolisthesis
- Sacroiliac joints: Posterior dimple at the posterior superior iliac spine; FABER test and sacroiliac compression provocation
- Sciatic nerve: Palpate along the course of the sciatic nerve — posterior gluteal region, posterior thigh, popliteal fossa, posterior calf
Move
| Movement | Normal Range |
|---|---|
| Forward flexion | 40-60 degrees (Schober test: marks placed 10 cm above and 5 cm below L5; should separate to >20 cm in full flexion; <15 cm suggests restriction) |
| Extension | 20-35 degrees |
| Lateral bending | 20-30 degrees each side |
| Rotation | 3-18 degrees each side (least in lumbar spine due to facet orientation) |
Neurological Examination (Lumbar)
| Level | Reflex | Motor | Sensation |
|---|---|---|---|
| L1-L2 | Cremasteric | Hip flexors | Groin / upper medial thigh |
| L3 | None | Quadriceps (weak) | Medial knee |
| L4 | Knee jerk | Quadriceps, tibialis anterior | Medial shin / medial foot |
| L5 | Hamstring jerk | Great toe extension (EHL), hip abduction | Dorsum of foot / big toe |
| S1 | Ankle jerk | Plantarflexion, eversion | Lateral foot / little toe |
| S2-S4 | Bulbocavernosus | Bladder/bowel/perianal | Perianal / perineum |
Special Tests (Lumbar)
PART 3: INVESTIGATIONS
3.1 Plain Radiographs
- Cervical: AP, lateral, open-mouth (odontoid peg view for C1-C2), oblique views (foraminal stenosis), flexion-extension dynamic views (instability assessment)
- Thoracic: AP and lateral for scoliosis (full-length standing), fractures, Scheuermann's disease
- Lumbar: AP and lateral (weight-bearing), oblique views (pars defect, spondylolysis — the "Scottie dog" with the collar sign), Ferguson view for L5-S1
- Full-length spine (EOS/scanogram): Scoliosis Cobb angle measurement, global sagittal alignment assessment
- OA/Spondylosis: loss of disc height, end-plate sclerosis, osteophytes (syndesmophytes in AS — flowing, vertical; "bamboo spine")
- Fracture: vertebral body height loss, kyphotic angulation, posterior element fracture
- Spondylolisthesis: forward slip graded I-IV (25% each increment) on lateral X-ray; "Napoleon's hat" sign on AP
- Spondylolysis: pars defect ("Scottie dog collar") on oblique views
- Infection: disc space narrowing with destruction of adjacent end-plates (Andersson lesion in Brucella)
3.2 MRI
- Disc herniation (best visualized on T2 axial and sagittal views)
- Spinal cord compression and signal change (T2 hyperintensity in the cord indicates myelomalacia — poor prognostic sign)
- Cauda equina compression
- Infection (discitis / osteomyelitis — T2 bright disc and end-plates; gadolinium enhancement confirms active infection)
- Tumour (epidural, intradural, intramedullary — gadolinium is essential)
- Nerve root compression in foraminal stenosis
- Ligamentum flavum hypertrophy (causing canal stenosis)
3.3 CT Scan
- Complex fracture assessment (burst fractures, facet fractures, posterior element injuries)
- Bony canal stenosis measurement
- Pre-operative planning (pedicle screw trajectory, deformity correction)
- CT myelogram (CT + intrathecal contrast): when MRI is contraindicated; best assessment of neural element compression at specific levels
- Post-operative assessment of fusion (bony bridging)
3.4 Nuclear Medicine
3.5 Electrophysiology
- Differentiate radiculopathy from peripheral neuropathy or plexopathy
- Identify the specific nerve root level involved
- Assess for evidence of denervation (acute) versus reinnervation (chronic/recovering)
- Useful when MRI findings do not correlate with clinical presentation
3.6 Blood Investigations
- FBC, CRP, ESR (markedly elevated in infection or inflammatory arthritis)
- HLA-B27 (ankylosing spondylitis — present in 90% of affected Caucasians)
- Rheumatoid factor and anti-CCP
- Blood cultures, CRP (spinal infection)
- ALP (Paget's disease of bone)
- Serum calcium, phosphate, ALP (bone metabolic disease)
- Protein electrophoresis / serum free light chains (multiple myeloma)
- PSA (prostate cancer — most common source of spinal metastasis in men)
- Mammography / breast imaging (breast cancer — common in women)
PART 4: COMMON SPINAL CONDITIONS
4.1 Cervical Spondylosis
4.2 Lumbar Disc Herniation
- Cauda equina syndrome (bilateral leg weakness, saddle anaesthesia, urinary retention — surgical emergency, decompression within 24-48 hours)
- Progressive motor weakness
- Signs of significant neurological deficit at presentation
4.3 Lumbar Spinal Stenosis
4.4 Spondylolisthesis
- Isthmic (Type II): Spondylolysis (pars fracture) allows the vertebral body to slip forward. Most common at L5-S1 in young athletes. Presents with low back pain, hamstring tightness, and occasionally L5 radiculopathy.
- Degenerative (Type III): Most common in adults over 50, more common in women, at L4-L5. Facet joint degeneration allows forward slip. Often associated with stenosis.
- Traumatic, Pathological, Dysplastic: Less common types.
4.5 Scoliosis
4.6 Ankylosing Spondylitis
PART 5: REHABILITATION EXERCISES
5.1 General Principles
- Centralization: Pain moves from the periphery (leg, arm) toward the spine with movement — this direction is therapeutic. Most common centralizing direction: extension for disc herniations.
- Peripheralization: Pain moves distally with movement — avoid this direction.
5.2 Cervical Spine Rehabilitation
Acute Phase (Week 1-2)
Sub-acute Phase (Week 3-6)
Strengthening Phase (Week 6-12)
5.3 Lumbar Spine Rehabilitation
McKenzie Extension Exercises (Extension Preference — Most Lumbar Disc Herniations)
Williams Flexion Exercises (Flexion Preference — Stenosis, Facet OA, Spondylolisthesis)
Core Stabilization Exercises
Pilates for the Spine
Aquatic / Hydrotherapy
PART 6: PATIENT-REPORTED OUTCOME MEASURES (PROMs) FOR THE SPINE
6.1 Disease-Specific Spine PROMs
6.2 Condition-Specific and Region-Specific PROMs
6.3 Psychosocial Assessment Tools
6.4 Recommended PROM Schedule for the Spine
| Timepoint | Lumbar Conditions | Cervical Conditions | Myelopathy |
|---|---|---|---|
| Baseline | ODI + NRS + EQ-5D + SBT | NDI + NRS + EQ-5D | mJOA + NDI + NRS |
| 6 Weeks | ODI + NRS | NDI + NRS | mJOA + NDI |
| 3 Months | ODI + NRS + EQ-5D | NDI + NRS + EQ-5D | mJOA + NDI + EQ-5D |
| 6 Months | ODI + NRS + EQ-5D + PGIC | NDI + NRS + EQ-5D + PGIC | mJOA + PGIC |
| 12 Months | Full battery + patient satisfaction | Full battery | Full battery |
PART 7: TREATMENT
7.1 Non-Pharmacological Treatment
7.2 Pharmacological Treatment
7.3 Injections
7.4 Surgical Treatment
Cervical Surgery
- ACDF (Anterior Cervical Discectomy and Fusion): Standard for cervical radiculopathy/myelopathy at 1-3 levels. Highly effective.
- Cervical disc arthroplasty: Motion-preserving alternative to ACDF at 1-2 levels; reduces adjacent segment degeneration long-term.
- Posterior laminectomy ± fusion: For multi-level stenosis or myelopathy; indicated when kyphosis is absent.
- Laminoplasty (Hirabayashi/Kurokawa): Motion-preserving posterior decompression; preferred in multi-level myelopathy with preserved lordosis.
Lumbar Surgery
- Microdiscectomy: For lumbar disc herniation with radiculopathy failing conservative management. 85-90% excellent results.
- Laminectomy (decompression): For lumbar spinal stenosis. Removes the hypertrophic lamina and ligamentum flavum.
- PLIF / TLIF (Posterior Lumbar Interbody Fusion): Instrumented fusion for degenerative spondylolisthesis, recurrent disc herniation, instability, and deformity. Involves pedicle screws, rods, and an interbody cage.
- ALIF (Anterior Lumbar Interbody Fusion): Accessed from the front; better lordosis restoration.
- Lateral approaches (XLIF / LLIF): Minimally invasive lateral approach; excellent for multi-level disease.
- Vertebroplasty / Kyphoplasty: Percutaneous injection of bone cement into osteoporotic compression fractures. Provides rapid pain relief; kyphoplasty also partially restores vertebral body height.
PART 8: AYURVEDA AND INTEGRATIVE TREATMENT FOR THE SPINE
8.1 Ayurvedic Conceptual Framework
- Katigraha / Kati Shoola: Low back pain (lumbar)
- Gridhrasi: Sciatica / lumbar radiculopathy (derived from "giddha" = vulture — the posture of the patient hunched over in pain)
- Manyastambha: Cervical spondylosis / neck stiffness ("manya" = neck; "stambha" = pillar/stiffness)
- Greeva Shoola: Cervical pain / radiculopathy
- Prishtha Shoola: Thoracic / mid-back pain
- Spondylosis: Generally classified as Asthi-Dhatu Kshaya (depletion of bone tissue) combined with Vata Prakopa
8.2 Panchakarma Procedures for the Spine
Kati Basti (Lumbar Oil Retention Therapy)
Greeva Basti (Cervical Oil Retention Therapy)
Pristha Basti (Thoracic / Full Spine Oil Retention)
Matra Basti (Medicated Oil Enema)
Abhyanga (Medicated Oil Massage)
Patra Pinda Sweda (Herbal Leaf Bolus Massage)
Shashtika Shali Pinda Sweda (Navarakizhi)
Kizhi (Podikizhi — Herbal Powder Bolus)
Pizhichil (Oil Drizzle Therapy)
Nasya (Nasal Administration)
8.3 Internal Ayurvedic Medicines for the Spine
8.4 Yoga Therapy for the Spine
- Setu Bandha Sarvangasana (Bridge pose): Strengthens gluteals and paraspinal muscles; opens the anterior hip.
- Marjariasana-Bitilasana (Cat-Cow): Gentle spinal flexion-extension mobilization in four-point kneeling.
- Balasana (Child's pose): Lumbar flexion stretch; relieves posterior element compression.
- Bhujangasana (Cobra): Gentle lumbar extension; the Ayurveda equivalent of McKenzie press-ups; improves disc hydration.
- Trikonasana (Triangle pose): Lateral bending with hip stability; strengthens quadratus lumborum.
- Shavasana (Corpse pose): Relaxation and parasympathetic activation for pain modulation.
- Tadasana (Mountain pose) with chin tucks: Postural correction
- Gomukhasana (Cow face): Shoulder and cervical stretch
- Matsyasana (Fish pose): Cervical extension and thoracic opening; reverses the kyphotic posture
- Viparita Karani (Legs up the wall): Cervical traction effect in the supine position with the legs elevated
8.5 Dietary and Lifestyle Recommendations (Nidan Parivarjana)
PART 9: INTEGRATED TREATMENT ALGORITHM FOR SPINAL CONDITIONS
KEY REFERENCES
- Bailey & Love's Short Practice of Surgery, 28th Edition — Spinal examination (cervical and lumbar), special tests
- Miller's Review of Orthopaedics, 9th Edition — Cervical spondylosis, disc disease, radiculopathy, myelopathy
- Firestein & Kelley's Textbook of Rheumatology — Lumbar spinal stenosis, ankylosing spondylitis
- Li Y et al. Exercise intervention for chronic low back pain: systematic review and network meta-analysis. Front Public Health. 2023.
- Patti A et al. Effectiveness of Pilates exercise on low back pain: systematic review with meta-analysis. Disabil Rehabil. 2024.
- Arslan S et al. Effect of exercise in treatment of lumbar disc herniation: systematic review. Acta Neurol Belg. 2025.
- Comer C et al. Exercise treatments for lumbar spinal stenosis: systematic review. Clin Rehabil. 2024.
- Apeldoorn AT et al. Management of low back pain and lumbosacral radicular syndrome: KNGF guideline. Eur J Phys Rehabil Med. 2024.
- Liu C et al. Effects of health qigong on cervical spondylosis: systematic review. Complement Ther Med. 2025.
- Sezerel B & Yuksel I. Osteopathic muscle energy techniques vs cervical mobilization in cervical spondylosis: RCT. Med Sci Monit. 2024.
- Rai AK et al. Multimodal Ayurveda Regimen for Knee OA (Janu Basti / Matra Basti): RCT Protocol. JMIR Research Protocols. 2025.
- Kshirsagar J et al. Panchakarma therapy in osteoarthritis. Int J Res Orthop. 2024.
- Heine P et al. Effectiveness of prehabilitation on post-operative recovery from lumbar spinal stenosis surgery. Clin Rehabil. 2026.
upper limb
"shoulder"[MeSH Terms] AND "rotator cuff" AND "rehabilitation"
upper limb Ayurveda treatment shoulder elbow Greeva Basti Pinda Sweda 2024
"frozen shoulder" AND "adhesive capsulitis" AND "treatment"
"elbow" AND "lateral epicondylitis" AND "exercise" AND "treatment"
upper limb rehabilitation exercises shoulder elbow wrist outcome measures DASH ASES QuickDASH 2024
THE UPPER LIMB — COMPLETE CLINICAL REFERENCE
Shoulder | Elbow | Wrist | Hand
Anatomy | Examination | Investigations | Conditions | Rehabilitation | PROMs | Treatment | Ayurveda
PART 1: ANATOMY
1.1 Overview
1.2 Shoulder Girdle
Bones
Joints of the Shoulder Complex
Rotator Cuff
- Supraspinatus (SSP): Arises from the supraspinous fossa; inserts on the superior facet of the greater tuberosity. Initiates abduction (first 15°) and acts throughout the arc. Runs under the acromion in the subacromial space — the most vulnerable tendon to impingement and tearing. Its critical zone, 1 cm from the insertion (the area of relative avascularity), is where most tears begin.
- Infraspinatus (ISP): From the infraspinous fossa; inserts on the middle facet of the greater tuberosity. Primary external rotator of the shoulder (60% of total ER strength).
- Teres minor: Below infraspinatus; inserts on the inferior facet of the greater tuberosity. External rotator and inferior stabilizer. Supplied by the axillary nerve.
- Subscapularis (SSc): Large, multi-pennate muscle from the subscapular fossa; inserts on the lesser tuberosity. The only anterior cuff muscle — the primary internal rotator and the key restraint to anterior instability. A subscapularis tear allows anterior translation of the humeral head.
Subacromial Space
1.3 Elbow
1.4 Wrist and Hand
1.5 Brachial Plexus
| Nerve | Cord | Roots | Motor | Sensory |
|---|---|---|---|---|
| Musculocutaneous | Lateral | C5, C6 | Biceps, brachialis, coracobrachialis | Lateral forearm |
| Axillary | Posterior | C5, C6 | Deltoid, teres minor | Regimental badge area (lateral upper arm) |
| Radial | Posterior | C5-T1 | Triceps, wrist/finger extensors, supinator | Dorsal hand (1st web space) |
| Median | Lateral + Medial | C6-T1 | Pronators, wrist flexors, FDP (index/middle), thenar muscles, lumbricals I+II | Radial 3.5 fingers |
| Ulnar | Medial | C8, T1 | FCU, FDP (ring/little), intrinsics, hypothenar, adductor pollicis | Ulnar 1.5 fingers |
PART 2: CLINICAL EXAMINATION
2.1 General Principles
2.2 Shoulder Examination
Look
Feel
- AC joint for swelling and tenderness
- Sternoclavicular joint
- Greater tuberosity (supraspinatus insertion — "critical zone" tenderness)
- Bicipital groove (biceps tendinopathy / tendon rupture)
- Coracoid process (subscapularis, pectoralis minor)
- Subacromial space (directly below the anterolateral acromion)
- Posterior joint line and axillary recess (posterior capsule tightness, posterior instability)
- Axilla for masses
Move
- Flexion (normal 180°) and extension (60°)
- Abduction (180°) — note painful arc (60-120° suggests subacromial impingement; >120° suggests AC joint pathology)
- Internal rotation — reach up the back (normal: thumb to T7-T8 level)
- External rotation — elbow at side (normal 60-90°) and at 90° abduction
Power Testing
- Supraspinatus (empty can test): Arm at 90° abduction in the scapular plane (30° forward of the coronal plane), thumb pointing down (pronated/empty can position). Examiner applies downward force — pain or weakness indicates supraspinatus pathology.
- Infraspinatus/Teres minor: Elbow at 90°, arm at side — resist external rotation.
- Subscapularis (lift-off test / belly-press test): The patient places the dorsum of the hand against the lumbar spine and lifts it away from the back against resistance (lift-off test). If unable to place hand behind back — belly-press: press the palm into the abdomen with elbow forward; inability to maintain elbow anterior to the body indicates subscapularis weakness.
Special Tests (Shoulder)
2.3 Elbow Examination
Look
Feel
- Medial epicondyle and medial collateral ligament (MCL — valgus stress/throwing injuries)
- Common flexor origin (medial epicondylitis/golfer's elbow)
- Lateral epicondyle and common extensor origin (lateral epicondylitis/tennis elbow)
- Radial head (palpable with pronation/supination, 2-3 cm distal to lateral epicondyle)
- Olecranon and olecranon bursa
- Cubital tunnel — roll the ulnar nerve between finger and medial epicondyle; tenderness = cubital tunnel syndrome; Tinel's sign at the cubital tunnel
Move
Special Tests (Elbow)
2.4 Wrist and Hand Examination
Look
- Dinner fork deformity: Distal radial fracture (Colles' fracture)
- Swan neck deformity: PIP hyperextension + DIP flexion (rheumatoid arthritis, intrinsic tightness)
- Boutonnière deformity: PIP flexion + DIP hyperextension (central slip injury, RA)
- Mallet finger: Flexion of the DIP joint (extensor tendon injury at the DIP level)
- Dupuytren's contracture: Cord-like thickening in the palm (palmar fascia), causing PIP joint flexion contracture of ring and little fingers
- Z-thumb (RA): CMC subluxation + IP hyperextension
- Claw hand: Ring and little finger clawing (ulnar nerve palsy — MCPext + IP flexion); or "intrinsic minus" hand
Feel
Special Tests (Wrist / Hand)
PART 3: INVESTIGATIONS
3.1 Plain Radiographs
3.2 MRI
- Rotator cuff tears: Sensitivity 95-100% for full-thickness tears. Partial-thickness tears are better assessed on MR arthrogram.
- Labral tears (Bankart, SLAP): MR arthrogram (gadolinium injected into joint) dramatically increases sensitivity to 85-95%.
- Frozen shoulder: Thickening and fibrosis of the inferior capsule and axillary recess. Useful when diagnosis is unclear.
- Carpal tunnel syndrome, TFCC tears, scaphoid avascular necrosis (Preiser's disease)
- Elbow: MCL tears, osteochondral lesions (Panner's disease, OCD)
3.3 Ultrasound
- Rotator cuff tears (full-thickness: sensitivity 92%, specificity 94%)
- Biceps tendon rupture, biceps tendinopathy
- AC joint injection guidance
- Bursal aspiration and injection
- Elbow: MCL, extensor/flexor tendons
- Carpal tunnel: median nerve cross-sectional area > 10 mm² is diagnostic for CTS at the pisiform level
3.4 CT
3.5 Nerve Conduction Studies and EMG
- Carpal tunnel syndrome: Slowed median nerve conduction velocity across the wrist (normal > 50 m/s); prolonged distal motor and sensory latencies.
- Cubital tunnel syndrome: Slowed ulnar nerve conduction across the elbow segment.
- Thoracic outlet syndrome: Reduced amplitude of the medial antebrachial cutaneous nerve SNAP.
- EMG detects denervation (fibrillations) and reinnervation (polyphasia) in muscles of the relevant myotome.
PART 4: COMMON CONDITIONS
4.1 Rotator Cuff Pathology
4.2 Adhesive Capsulitis (Frozen Shoulder)
- Painful (freezing) phase: 2-9 months. Intense night pain; progressive loss of ROM.
- Frozen (stiff) phase: 4-12 months. Pain subsides but stiffness persists and is maximal.
- Thawing phase: 12-42 months. Gradual spontaneous recovery of ROM.
4.3 Lateral Epicondylitis (Tennis Elbow)
4.4 Medial Epicondylitis (Golfer's Elbow)
4.5 Carpal Tunnel Syndrome (CTS)
4.6 Cubital Tunnel Syndrome
PART 5: REHABILITATION EXERCISES
5.1 Shoulder Rehabilitation
Phase 1 — Acute / Protection Phase (Weeks 1-3)
Phase 2 — Mobility Phase (Weeks 3-6)
Phase 3 — Strengthening Phase (Weeks 6-12)
- Sidelying external rotation: Lie on the opposite side, elbow bent to 90° at the side, rotate the arm upward against gravity or band resistance. Start 0.5 kg and progress. 3 sets of 15. The most fundamental cuff strengthening exercise.
- Standing external rotation (band): Band anchored medially; pull the arm outward. Elbow at 90°.
- Standing internal rotation (band): Band anchored laterally; pull inward.
- Full can (scapular plane elevation): Arm in scapular plane (30° forward of coronal), thumb pointing up. Elevate to shoulder height against resistance. Better supraspinatus activation than empty can with less subacromial impingement.
- Prone Y-T-W exercises: Prone on a bench. Y = arm overhead in a Y shape; T = arms directly out to the side; W = elbows bent at 90°, arms pulled up and back. These powerfully activate lower trapezius, rhomboids, and posterior cuff with minimal subacromial irritation.
Phase 4 — Functional / Return to Sport
5.2 Elbow Rehabilitation
Lateral Epicondylitis Protocol
Medial Epicondylitis Protocol
Post-Elbow Surgery (MCL Reconstruction — Tommy John)
5.3 Wrist and Hand Rehabilitation
PART 6: PATIENT-REPORTED OUTCOME MEASURES (PROMs)
6.1 Upper Limb General PROMs
6.2 Region-Specific Shoulder PROMs
6.3 Elbow PROMs
6.4 Wrist and Hand PROMs
6.5 PROM Selection Guide for Upper Limb
| Condition | Primary PROM | Secondary PROM |
|---|---|---|
| Shoulder impingement / rotator cuff (conservative) | ASES / SPADI | QuickDASH + VAS |
| Rotator cuff repair (surgical) | ASES + Constant | QuickDASH + OSS |
| Frozen shoulder | SPADI / DASH | Constant + VAS |
| Shoulder instability | ASIS / Rowe score | QuickDASH + OSES |
| Shoulder arthroplasty | OSS / ASES | Constant + QuickDASH |
| Lateral epicondylitis | PREE + VAS | QuickDASH |
| Elbow arthroplasty | MEPS / LES | QuickDASH |
| Carpal tunnel syndrome | BCTQ | QuickDASH + VAS |
| Distal radius fracture | PRWE | QuickDASH + VAS |
| Hand / multiple joints | DASH / QuickDASH | MHQ |
| Any upper limb (general) | DASH or QuickDASH | VAS / PROMIS |
PART 7: TREATMENT
7.1 Non-Pharmacological Treatment
7.2 Pharmacological Treatment
- Subacromial injection for impingement/partial cuff tears — most effective for short-term pain (4-8 weeks); no benefit over physiotherapy at 6 months
- Glenohumeral injection for frozen shoulder — most effective in the painful phase
- Lateral epicondyle injection — excellent short-term, worse long-term vs. physiotherapy
- Carpal tunnel injection — relieves symptoms in 80% at 1 month; 50% maintained at 1 year; delays surgery
7.3 Surgical Treatment
| Condition | Procedure | Approach |
|---|---|---|
| Rotator cuff tear (traumatic/functional deficit) | Arthroscopic cuff repair | Arthroscopic |
| Impingement (failed conservative) | Subacromial decompression (acromioplasty) | Arthroscopic |
| Frozen shoulder (refractory) | Arthroscopic capsular release / MUA | Arthroscopic / GA |
| Shoulder instability (Bankart) | Arthroscopic Bankart repair | Arthroscopic |
| Shoulder instability (bone loss) | Latarjet procedure (coracoid transfer) | Open |
| ACJ dislocation (Grade III-VI) | ACCF ligament reconstruction | Open |
| Shoulder OA | Total shoulder arthroplasty / Reverse TSA | Open |
| Lateral epicondylitis (failed Rx) | ECRB debridement | Open/Arthroscopic |
| MCL reconstruction | Ulnar collateral ligament reconstruction (Tommy John) | Open |
| Cubital tunnel syndrome | In situ decompression / anterior transposition | Open |
| Carpal tunnel syndrome | Carpal tunnel decompression (CTD) | Open / Endoscopic |
| Distal radius fracture | ORIF with volar locking plate | Open |
| Scaphoid non-union | Cancellous bone graft + headless screw (Herbert) | Open |
| Dupuytren's contracture | Fasciectomy / collagenase injection (Xiaflex) | Open |
PART 8: AYURVEDA AND INTEGRATIVE TREATMENT FOR THE UPPER LIMB
8.1 Ayurvedic Framework
8.2 Panchakarma Procedures for the Upper Limb
Greeva Basti
Amsa Basti / Shoulder Basti
Patra Pinda Sweda (Herbal Leaf Bolus Massage)
Shashtika Shali Pinda Sweda (Navarakizhi)
Pizhichil (Oil Bath Drizzle)
Nasya Karma (Nasal Oil Instillation)
Upanaha Sweda (Medicated Poultice)
Murivenna Seka
Sthanika Abhyanga (Local Oil Massage)
8.3 Internal Ayurvedic Medicines for the Upper Limb
8.4 Yoga Therapy for the Upper Limb
- Garudasana (Eagle pose): Wraps the arms across the body, stretching the posterior capsule and rotator cuff; excellent for posterior capsule tightness in impingement.
- Gomukhasana (Cow face arms): One arm overhead and behind, one arm behind the lower back — clasped together. Stretches the full shoulder girdle.
- Sarvangasana (Shoulderstand): Inverted posture; decompresses the shoulder; improves proprioception.
- Utthita Parsvakonasana (Extended side angle): Opens the shoulder; improves ER and lateral rotation.
- Vinyasa (flow) push-ups: Progressive triceps and forearm loading; builds elbow extensor endurance.
- Prayer pose (Namaste) and reverse prayer: Stretches the wrist flexors (reverse prayer, held behind the back) and extensors.
- Downward dog (Adho Mukha Svanasana): Weight-bearing through the hands; progressive carpal stretch and wrist extensor strengthening.
- Fist opening and closing in Dharana mudras: Fine motor nerve coordination training.
8.5 Evidence for Ayurveda in Upper Limb Conditions
PART 9: INTEGRATED TREATMENT ALGORITHM
KEY REFERENCES
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set — Rotator cuff impingement, tendinopathy, calcific tendinitis
- Bailey & Love's Short Practice of Surgery, 28th Edition — Upper limb examination, hand and wrist
- Campbell's Operative Orthopaedics, 15th Edition — Carpal tunnel syndrome, hand anatomy
- Celik D et al. Mulligan's Mobilization with Movement in Shoulder Pathologies: Systematic review and meta-analysis. J Integr Complement Med. 2025.
- Poku D et al. Efficacy of hydrodilatation in frozen shoulder: systematic review and meta-analysis. Br Med Bull. 2023.
- Gupta M et al. Muscle energy and joint mobilisation techniques in frozen shoulder: systematic review. Musculoskeletal Care. 2024.
- Chen Q et al. Long-term effectiveness of conservative management for lateral epicondylitis: meta-analysis. J Plast Surg Hand Surg. 2023.
- See ZH et al. Eccentric exercise therapy for medial epicondylitis: systematic review. Complement Ther Med. 2026.
- Ma X et al. Therapeutic effects of dry needling on lateral epicondylitis: systematic review and meta-analysis. Arch Phys Med Rehabil. 2024.
- Brindisino F et al. DASH psychometric properties in frozen shoulder. BMC Musculoskelet Disord. 2024.
- Salamh P et al. Quality of clinical practice guidelines for frozen shoulder: systematic review. Physiother Theory Pract. 2025.
- PMC3202264 — Laghumasha Taila Nasya in Apabahuka (Frozen Shoulder). Ayurvedic evidence.
- PMC3296342 — Nirgundi Patra Pinda Sweda and Ashwagandhadi Guggulu in OA management.