
17804702361192067793071469085959.jpg
Explain the site sizeshape edges marginsfloor depth discharge and surrounding area of this ulcers
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Now I have everything needed. Here is the full systematic analysis of the ulcer in the image, applied feature by feature using the framework from S Das - A Manual on Clinical Surgery, 13th Edition.
Systematic Examination of the Ulcer
Looking at the image, this is a large fungating/malignant ulcer over the breast/anterior chest wall, most likely carcinoma of the breast that has ulcerated through the skin. Measurement arrows are drawn across it indicating its dimensions are being recorded. Here is the full clinical description:
1. Site
The ulcer is situated over the anterior chest wall, centred on the breast (most likely left breast based on orientation). It involves the skin and soft tissues of the breast mound. This is a classic site for ulcerated carcinoma of the breast or a fungating breast tumour.
2. Size
From the arrows visible in the image (cross-measurement technique), the ulcer appears to be approximately 8-10 cm in its largest diameter - it occupies a large proportion of the breast surface. Size is recorded as two perpendicular measurements (length x breadth), and depth separately.
3. Shape
The shape is irregular and lobulated - it does not conform to any geometric pattern. The surface is uneven with nodular projections, which is characteristic of a fungating (proliferative-ulcerative) malignant growth. A fungating ulcer grows outward (exophytic) while simultaneously ulcerating, producing this characteristic cauliflower-like appearance.
4. Edges
The edges are everted (rolled out) - this is the hallmark of a squamous cell carcinoma or ulcerated adenocarcinoma. As described in S Das:
"Rolled out (Everted) edge is a characteristic feature of squamous-celled carcinoma or an ulcerated adenocarcinoma. This ulcer is caused by fast growing cellular disease, the growing portion at the edge of the ulcer heaps up and spills over the normal skin to produce an everted edge."
In the image, the edges are raised, irregular, and appear to heap outward over surrounding skin - consistent with everted/rolled edges.
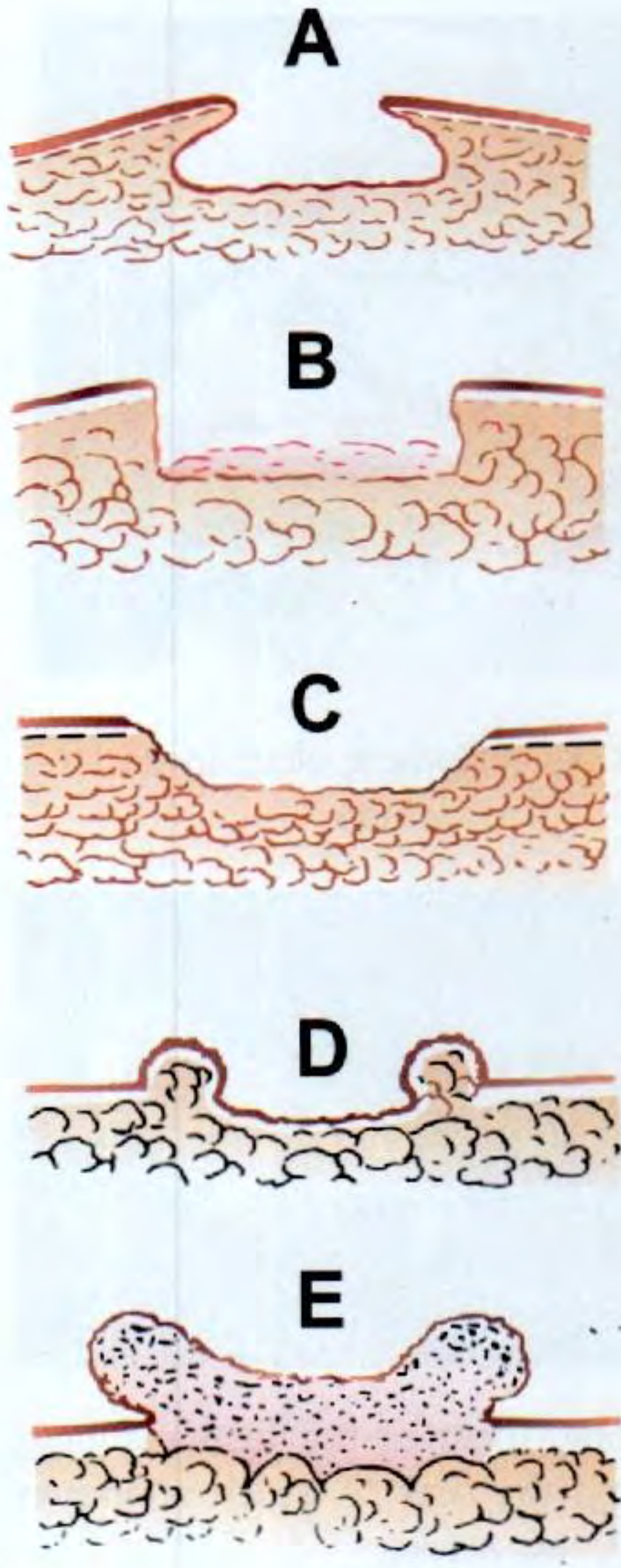
(Type E above corresponds to this ulcer's edge)
5. Margins
The margins are indurated (hard), irregular, and ill-defined. There is no sharp demarcation between the ulcer and surrounding skin. The margins infiltrate into the surrounding tissues, which is a feature of malignant infiltration. On palpation (if examined clinically), the margins would feel hard and nodular due to tumour infiltration.
6. Floor
The floor is covered with necrotic slough and unhealthy granulation tissue, appearing as:
- Yellowish-white necrotic material (the pale/cream-coloured areas seen on the surface)
- Areas of red granulation mixed with the slough
- A dark necrotic/eschar area (the dark black spot visible centrally - likely an area of deep necrosis or a draining sinus)
This mixed floor of necrosis + unhealthy granulation is typical of a spreading/malignant ulcer. In S Das:
"Spreading ulcer, when the surrounding skin of the ulcer is inflamed and the floor is covered with profuse and offensive slough without any evidence of granulation tissue."
7. Depth
The ulcer appears deep, penetrating through the skin and subcutaneous tissue into the breast parenchyma. In advanced carcinoma, it may reach the pectoral fascia or even the chest wall muscles. The depth cannot be fully assessed from inspection alone but the raised everted edges and the necrotic floor suggest significant depth.
8. Discharge
The discharge is likely:
- Sero-sanguinous to purulent - a mixture of blood, serum, and infected necrotic material
- Offensive/foul-smelling - due to anaerobic bacterial colonisation of necrotic tissue
- The dressing/gauze visible at the bottom of the image appears stained, confirming active discharge
In S Das: "Discharge from a malignant ulcer is usually thin, watery and blood-stained, with an offensive smell due to secondary infection and necrosis."
9. Surrounding Area
The surrounding skin and tissues show:
- Peau d'orange appearance (skin dimpling) - visible on the upper chest area adjacent to the ulcer, due to dermal lymphatic oedema from tumour invasion
- Oedema and induration of the surrounding skin - the skin around the ulcer appears thickened and inflamed
- Erythema (redness/discolouration) of the perilesional skin indicating inflammatory reaction or tumour infiltration
- Skin tethering - the skin appears fixed to the underlying tumour
- The axillary region appears full, suggesting possible axillary lymph node involvement/metastasis
Summary Table
| Feature | Finding | Significance |
|---|---|---|
| Site | Anterior chest wall / breast | Breast carcinoma |
| Size | ~8-10 cm (large) | Advanced disease |
| Shape | Irregular, fungating, lobulated | Malignant proliferative growth |
| Edges | Everted / rolled out | Carcinoma (SCC or adenocarcinoma) |
| Margins | Indurated, irregular, ill-defined | Malignant infiltration |
| Floor | Necrotic slough + unhealthy granulation, areas of eschar | Spreading/malignant ulcer |
| Depth | Deep, penetrating | Advanced local invasion |
| Discharge | Sero-sanguinous, offensive, purulent | Secondary infection + necrosis |
| Surrounding | Peau d'orange, oedema, erythema, axillary fullness | Dermal lymphatic invasion, nodal spread |
Most likely diagnosis: Advanced/fungating carcinoma of the breast (T4b or T4d - locally advanced)
This is consistent with Stage III-IV breast carcinoma with skin involvement, ulceration, and likely regional nodal metastasis. The clinical features correlate with a spreading malignant ulcer as classified by S Das.
- S Das - A Manual on Clinical Surgery, 13th Edition, Chapter 4: Examination of an Ulcer
This is a shared conversation. Sign in to Orris to start your own chat.