biomechanics of injury . Note on Transportational injuries , md Fmt answer for 20 marks
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Here is the complete, exam-ready 20-mark answer:
BIOMECHANICS OF INJURY - NOTE ON TRANSPORTATIONAL INJURIES
1. INTRODUCTION
Injury is defined as damage to bodily tissues resulting from energy transfer. At its most fundamental level, biomechanics of injury studies the physical forces acting on the human body and the resulting patterns of tissue damage. Mechanisms of injury are broadly categorized as:
- Penetrating - stab wounds, gunshot wounds
- Blunt - motor vehicle collisions (MVCs), falls
- Thermal - flame burns, electrocution
Transportation injuries form the dominant subcategory of blunt trauma and represent one of the leading causes of injury-related mortality worldwide.
2. BASIC PHYSICS OF BLUNT TRAUMA
The foundation for understanding all transportation injuries is the kinetic energy equation:
KE = (M × V²) / 2
Where:
- KE = kinetic energy
- M = mass of the object
- V = velocity
Key implications:
- Velocity has a squared relationship with kinetic energy, meaning even modest increases in speed dramatically increase the destructive potential. A car traveling at 65 mph imparts roughly 4x the energy of one at 32 mph (same mass).
- Two large SUVs (~6,000 lb each) colliding head-on at 65 mph generate enormous forces, much of which is redirected by modern crumple zones and safety systems - but clinicians routinely underestimate the magnitudes involved.
- Blunt trauma causes damage via crush forces (direct compression) or shear forces (differential motion between adjacent structures).
3. TRANSPORTATIONAL INJURIES - CLASSIFICATION BY MECHANISM
3.1 Motor Vehicle Collision (MVC) Patterns
A. Frontal (Head-On) Impact
This is the most common and well-studied crash vector.
- The vehicle decelerates abruptly; unrestrained occupants continue forward by inertia (Newton's 1st Law).
- The body strikes the steering wheel (upper body/thorax/face) or the knees strike the dashboard (lower extremity/pelvis).
Classic injury pattern (unrestrained driver):
| Body Region | Injury |
|---|---|
| Head/face | Facial fractures, traumatic brain injury |
| Neck | Cervical spine fracture/dislocation |
| Chest | Sternal fracture, rib fractures, aortic disruption, pulmonary contusion |
| Abdomen | Liver/spleen laceration (from steering wheel) |
| Knees/lower limb | Patellar fracture, tibial plateau fracture, hip dislocation |
B. Rear Impact
- The stationary (or slower-moving) front vehicle is struck from behind.
- The occupant's torso is thrown forward abruptly while the head lags behind momentarily.
- This creates cervical spine hyperextension - the classic "whiplash" injury.
- The severity depends on the differential velocity between the two vehicles (closing speed).
Classic injuries:
- Cervical ligamentous injury / hyperextension strain
- Cervical facet fractures
- Acceleration-deceleration traumatic brain injury
C. Lateral (Side) Impact
- Rotational and lateral forces are imparted on the occupant.
- The passenger compartment often protrudes significantly into the occupant space.
- These forces are particularly dangerous because:
- Side-door crumple zones are far smaller than front/rear
- Rotational forces cause torsion injuries at junctions of mobile and fixed structures
Classic injuries:
- Aortic laceration (mobile aortic arch vs. fixed ligamentum arteriosum)
- Cervical spinal ligamentous injuries
- Ipsilateral rib fractures with liver/spleen lacerations
- Pelvic fractures
- Contralateral head injury (contrecoup)
D. Rollover Crashes
- Considered the most dangerous crash type because the vehicle is impacted from multiple angles repeatedly.
- Occupants are thrown violently in multiple directions.
- Ejection is common - increases the probability of death by approximately 10-fold compared to occupants who remain inside the vehicle.
- Death of another occupant in the same vehicle is a high-risk surrogate marker for the severity of impact forces.
Classic injuries: Multi-system trauma; head, cervical spine, thoracoabdominal injuries; crush injuries.
4. INJURY MARKERS AND CLINICAL CLUES IN TRANSPORTATION INJURIES
4.1 The Seatbelt Sign
A transverse ecchymotic band across the lower abdomen indicates energy transfer from the lap seatbelt. This must raise suspicion for:
- Bowel injury / mesenteric tear
- Pancreatic laceration (body of pancreas over the spine)
- Lumbar spine fracture (Chance fracture - flexion-distraction injury)
The L1 vertebral wedge fracture in this context mandates exclusion of pancreatic injury, because the pancreatic body drapes directly over the anterior surface of L1.
4.2 Orthopedic Injuries as Energy Surrogates
Fractures serve as markers of kinetic energy transfer and should prompt proactive search for injuries to adjacent organs, nerves, vessels, and tendons.
| Diagnosed Fracture | Associated Injury to Suspect |
|---|---|
| Temporal/parietal skull fracture | Epidural hematoma |
| Maxillofacial fracture | Cervical spine fracture |
| Sternal fracture | Cardiac contusion |
| 1st and 2nd rib fracture | Descending thoracic aortic injury; intra-abdominal bleeding |
| Fractured scapula | Pulmonary contusion |
| Ribs 8-12 (right) | Liver laceration |
| Ribs 8-12 (left) | Splenic laceration |
| Pelvic fracture | Ruptured bladder; urethral transection |
| Fractured humerus | Radial nerve injury |
(Source: Mulholland & Greenfield's Surgery, 7e, Table 19.2)
5. PEDESTRIAN INJURIES
Pedestrian-vehicle impacts follow a predictable three-phase pattern (Waddell's triad):
- Phase 1 - Primary impact: The vehicle bumper strikes the lower extremities (tibia/fibula fractures, knee ligament injuries). In children, the bumper is at a higher level relative to body height, causing abdominal/thoracic impact.
- Phase 2 - Secondary impact: The pedestrian's torso is thrown onto the bonnet (hood) of the vehicle - causing thoracic, abdominal, and head injuries.
- Phase 3 - Tertiary impact: The pedestrian is thrown off and strikes the ground - causing further head, cervical spine, and extremity injuries.
Waddell's Triad (classic in children): Head injury + thoracoabdominal injury + contralateral lower limb fracture.
6. MOTORCYCLE INJURIES
Motorcycle riders lack the protective metal frame of a car. Injury patterns depend on the direction of impact:
- Frontal impact: Rider is thrown forward over the handlebars - head, neck, and bilateral femur fractures.
- Lateral impact: Leg is caught between the motorcycle and the vehicle - crush injuries, tibia/fibula fractures.
- Ejection: Rider is thrown clear - similar to car ejection, markedly increases severity.
- Laying the bike down: A protective maneuver - rider slides along the road - friction abrasions ("road rash"), but avoids the worst impact forces.
Helmets reduce the risk of fatal head injury by approximately 37%.
7. BICYCLE AND OTHER TRANSPORTATION INJURIES
Cyclists suffer similar injury patterns to motorcyclists but at lower velocities. Typical patterns:
- Head injury (most common cause of cyclist fatality)
- Clavicular fractures (outstretched hand landing)
- Handlebar injuries: upper abdominal solid organ lacerations (liver, spleen, duodenum)
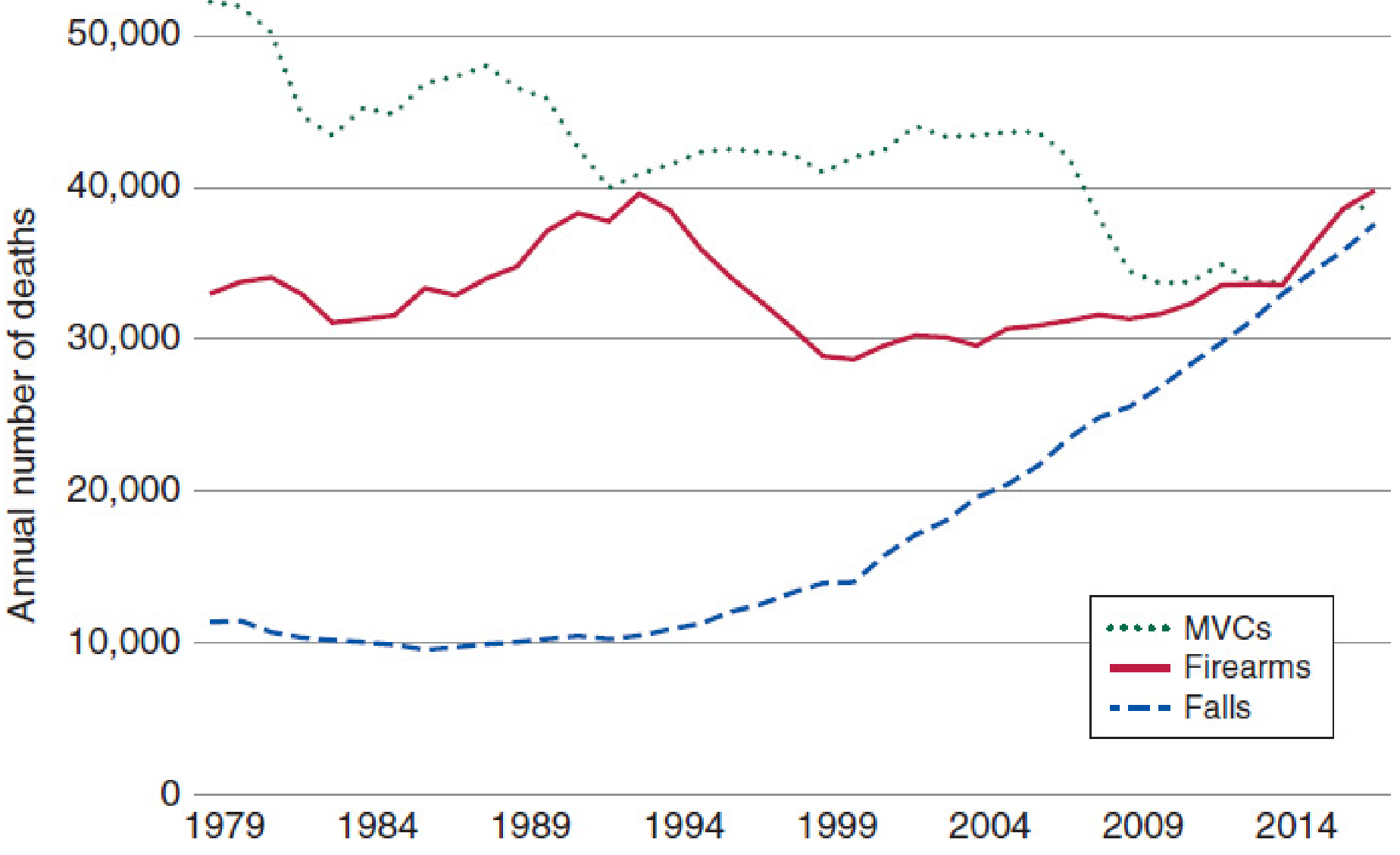
All forms of transportation - including bicycle accidents, skateboarding, and motorcycle crashes - are well-recognized causes of traumatic brain injury (TBI), second only to falls in frequency.
8. HIGH-RISK INDICATORS IN TRANSPORTATION INJURIES
The following historical features should trigger a high-risk trauma workup regardless of initial vital signs:
| High-Risk Feature | Clinical Significance |
|---|---|
| Speed > 60 km/h | High kinetic energy transfer |
| Ejection from vehicle | 10x increased mortality risk |
| Death of another occupant | Surrogate for impact severity |
| Intrusion of passenger compartment | Direct force to body |
| Rollover | Multi-directional impact |
| Pedestrian or cyclist struck | No protective frame |
| Seatbelt sign present | Internal abdominal/spinal injury |
9. TORSION AND SHEAR INJURIES IN DECELERATION
High-speed deceleration disproportionately injures regions where mobile structures meet fixed anatomical points. This is because different parts of the body decelerate at different rates:
- Aortic arch laceration at the isthmus (junction with the fixed descending aorta at the ligamentum arteriosum) - most common in lateral impact and severe frontal crashes.
- Mesenteric tears - mobile bowel loops shear off the fixed retroperitoneal mesentery.
- Cervical spinal cord injuries - mobile head shears at the fixed cervicothoracic junction.
- Liver/spleen lacerations - intraperitoneal organs continue moving against their fixed ligamentous attachments (falciform, coronary, splenic ligaments).
10. CLINICAL APPLICATION: MECHANISM-DIRECTED ASSESSMENT
Understanding biomechanics allows the clinician to anticipate injuries even before imaging. Key principles:
- Never assume a "normal" anatomical position at the time of impact - victims often assume protective postures that alter injury vectors.
- Pre-hospital information is critical - crash speed, type of impact, use of seatbelt, airbag deployment, death of another occupant, ejection status.
- Orthopedic injuries are energy markers - always look "beyond the fracture" to adjacent organs, nerves, and vessels.
- Mechanism + physical exam together - a seatbelt sign, steering wheel deformation, and windshield spider-cracking each tell you where energy was deposited.
SUMMARY TABLE: IMPACT TYPE vs. EXPECTED INJURIES
| Impact Type | Primary Force | Classic Injuries |
|---|---|---|
| Frontal (unrestrained) | Anterior deceleration | Head, face, neck, sternum, liver/spleen, bilateral femur, patellar |
| Frontal (restrained) | Lap/shoulder belt | Sternal fracture, cardiac contusion, seatbelt sign injuries |
| Rear | Hyperextension | Whiplash, cervical ligament/facet injuries |
| Lateral | Rotational + shear | Aortic laceration, ipsilateral rib/solid organ, TBI |
| Rollover | Multi-directional | Multi-system, spinal, ejection injuries |
| Pedestrian Phase 1 | Bumper | Lower limb fractures |
| Pedestrian Phase 2 | Hood | Thoracoabdominal, head injuries |
| Pedestrian Phase 3 | Ground | Head, cervical spine, extremity |
CONCLUSION
The biomechanics of transportational injury is governed by the physics of kinetic energy transfer (KE = MV²/2). The direction, speed, and mechanism of impact predict specific and reproducible injury patterns. Ejection, rollover, and high-speed crashes carry the worst prognosis. Clinical assessment must integrate the full mechanism history - seatbelt sign, impact type, ejection status, and orthopedic injuries as surrogate energy markers - to ensure no injury is missed in the primary and secondary surveys.
Source: Mulholland & Greenfield's Surgery: Scientific Principles and Practice, 7th Edition; Harrison's Principles of Internal Medicine, 22nd Edition
Cerebro Vascular Supply
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have all the content needed for a thorough, well-illustrated answer. Let me compile it.
CEREBROVASCULAR SUPPLY
1. INTRODUCTION
The brain receives approximately 15-20% of cardiac output (about 750 mL/min) despite constituting only ~2% of body weight. It has virtually no energy reserves, making an uninterrupted blood supply essential - neuronal death begins within minutes of ischemia. The cerebral circulation is divided into two main systems: the anterior (carotid) circulation and the posterior (vertebrobasilar) circulation, which meet at the base of the brain to form the Circle of Willis.
2. ARTERIAL SUPPLY - OVERVIEW
The brain is supplied by four major arteries:
- Right and left Internal Carotid Arteries (ICA) - anterior circulation
- Right and left Vertebral Arteries - posterior circulation
3. ANTERIOR CIRCULATION - INTERNAL CAROTID SYSTEM
3.1 Course of the Internal Carotid Artery
The ICA arises from the common carotid artery at the carotid bifurcation (typically at C4 level). It has four named segments:
| Segment | Location |
|---|---|
| Cervical | Vertical ascent in the neck - no branches |
| Petrous | Enters carotid canal of temporal bone - horizontal course |
| Cavernous | S-shaped "carotid siphon" within the cavernous sinus |
| Supraclinoid (intracranial) | Pierces dura, enters subarachnoid space - gives main branches |
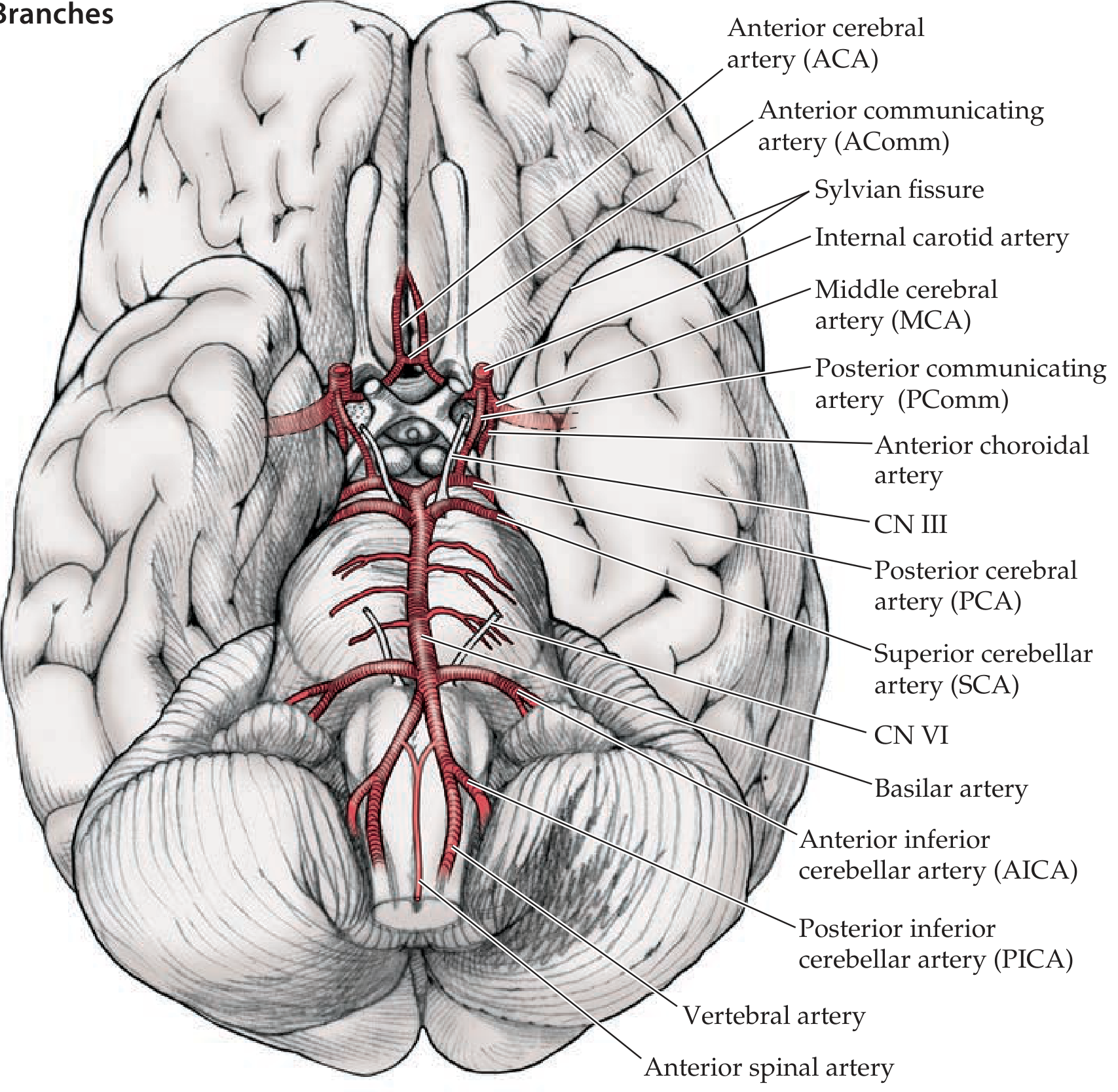
3.2 Branches of the Supraclinoid ICA
Remembered by the mnemonic: OPAAM
| Letter | Artery |
|---|---|
| O | Ophthalmic artery |
| P | Posterior communicating artery (PComm) |
| A | Anterior choroidal artery |
| A | Anterior cerebral artery (ACA) |
| M | Middle cerebral artery (MCA) |
Ophthalmic artery: Enters the optic foramen with the optic nerve; supplies the retina. This is why ICA disease can cause amaurosis fugax (transient monocular blindness).
Posterior communicating artery (PComm): Links the ICA to the posterior cerebral artery, joining anterior and posterior circulations.
Anterior choroidal artery: Supplies the globus pallidus, putamen, part of the thalamus (including the lateral geniculate nucleus), and the posterior limb of the internal capsule (containing corticospinal and corticobulbar tracts). Its occlusion causes contralateral hemiparesis, hemisensory loss, and hemianopia.
4. THE CIRCLE OF WILLIS
The Circle of Willis is an anastomotic ring at the base of the brain, formed by:
- Anteriorly: Two ACAs connected by the Anterior Communicating Artery (AComm)
- Laterally: Two ICAs
- Posteriorly: Two PCAs arising from the tip of the basilar artery
- Linking anterior to posterior: Two Posterior Communicating Arteries (PComm)
A complete, full-caliber Circle of Willis is present in only approximately 34% of individuals - anatomical variants are common.
Function of the Circle: Under normal conditions, blood from anterior and posterior circulations does not mix (pressures are equal). In pathological states (arterial occlusion), it acts as an anteroposterior or side-to-side collateral shunt, redistributing blood to ischemic regions.
5. THE THREE MAIN CEREBRAL ARTERIES AND THEIR TERRITORIES
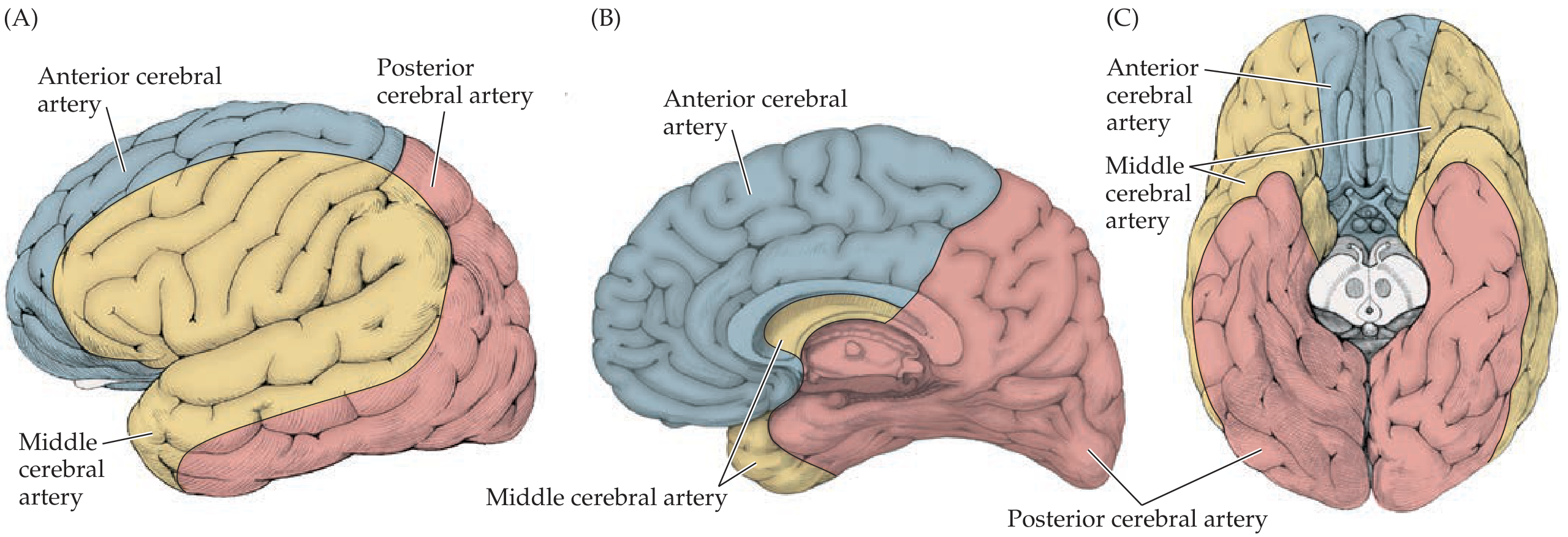
5.1 Anterior Cerebral Artery (ACA)
Origin: Terminal branch of ICA; the two ACAs are joined anteriorly by the AComm.
Course: Runs anteriorly and medially, then curves up and over the corpus callosum in the interhemispheric fissure.
Territory - Superficial (cortical):
- Medial surface of the frontal and parietal lobes
- The leg and foot area of the motor and sensory cortex (in the interhemispheric fissure)
Territory - Deep:
- Recurrent artery of Heubner (off A1 segment): head of the caudate nucleus, anterior putamen, globus pallidus, anterior limb of internal capsule
ACA occlusion deficits:
- Contralateral leg/foot weakness and sensory loss (leg area of motor strip is in interhemispheric fissure)
- Relatively spared arm and face
- Urinary incontinence (medial frontal lobe)
- Abulia (frontal lobe involvement)
5.2 Middle Cerebral Artery (MCA)
Origin: Larger terminal branch of the ICA; most commonly affected in stroke.
Course: Turns laterally into the Sylvian fissure (lateral sulcus), usually bifurcates into:
- Superior division - supplies cortex above the Sylvian fissure (lateral frontal lobe, peri-Rolandic cortex)
- Inferior division - supplies cortex below the Sylvian fissure (lateral temporal lobe, variable parietal lobe)
Territory - Superficial: Most of the dorsolateral convexity of the cerebral hemisphere - the face and arm areas of motor/sensory cortex, Broca's area (dominant inferior frontal gyrus), Wernicke's area (dominant superior temporal gyrus), parietal association cortex.
Territory - Deep (Lenticulostriate arteries): Small penetrating vessels arising from the proximal MCA before it enters the Sylvian fissure, penetrating the anterior perforated substance to supply:
- Basal ganglia (caudate, putamen, globus pallidus)
- Posterior limb of internal capsule
These vessels are particularly prone to lacunar infarction and hypertensive hemorrhage.
MCA occlusion deficits (left side - dominant hemisphere):
| Region | Deficit |
|---|---|
| Superior division | Contralateral face + arm weakness and sensory loss; Broca's aphasia (nonfluent) |
| Inferior division | Wernicke's aphasia (fluent); superior quadrantanopia |
| Deep territory | Contralateral hemiparesis (face + arm + leg) - internal capsule |
| Complete MCA (stem) | All of the above; dense contralateral hemiplegia, hemisensory loss, hemianopia, aphasia (dominant) or hemineglect (non-dominant) |
5.3 Posterior Cerebral Artery (PCA)
Origin: Arises from the tip of the basilar artery (posterior circulation). In fetal variant (~20-30% of people), it may arise directly from the ICA ("fetal PCA").
Course: Curves posteriorly and inferiorly around the midbrain, sending branches over the inferior and medial temporal lobes and the medial occipital cortex.
Territory - Superficial:
- Inferior and medial temporal lobes (including hippocampus)
- Medial occipital cortex (primary visual cortex along the calcarine fissure)
Territory - Deep:
- Thalamoperforator arteries (from proximal PCA): thalamus, posterior limb of internal capsule
- Thalamogeniculate arteries: thalamus
- Posterior choroidal arteries: thalamus and choroid plexus
PCA occlusion deficits:
- Contralateral homonymous hemianopia (most common) - with macular sparing (dual supply from MCA)
- Memory impairment (if hippocampus involved)
- Visual agnosia, alexia without agraphia (dominant PCA)
- Contralateral hemisensory loss (if thalamus involved)
6. POSTERIOR CIRCULATION - VERTEBROBASILAR SYSTEM
6.1 Vertebral Arteries
- Arise from the subclavian arteries bilaterally
- Ascend through the foramina transversaria of cervical vertebrae C1-C6
- Enter the skull via the foramen magnum
- Unite at the pontomedullary junction to form the basilar artery
Main branches of the vertebral arteries:
- Posterior inferior cerebellar artery (PICA): Supplies the lateral medulla and inferior cerebellum. Occlusion = Lateral Medullary (Wallenberg) Syndrome.
- Anterior spinal artery: Formed by contributions from both vertebral arteries; supplies the anterior two-thirds of the spinal cord.
- Posterior spinal arteries
6.2 Basilar Artery
Runs along the ventral surface of the pons in the basilar sulcus.
Branches:
| Branch | Territory |
|---|---|
| Anterior Inferior Cerebellar Artery (AICA) | Inferior cerebellum, lateral lower pons, inner ear (via labyrinthine artery) |
| Pontine perforators | Pons (multiple small branches) |
| Superior Cerebellar Artery (SCA) | Superior cerebellum, upper pons, midbrain |
| Posterior Cerebral Arteries (PCA) | Terminal branches; occipital lobes, medial temporal lobes, thalamus |
"Top of the basilar" syndrome: Occlusion of the rostral basilar artery causes bilateral PCA + SCA territory infarction with severe visual disturbances, altered consciousness, and oculomotor deficits.
7. DEEP CEREBRAL STRUCTURES - PENETRATING VESSELS SUMMARY
| Artery | Deep Structures Supplied |
|---|---|
| Lenticulostriate aa. (from MCA) | Caudate, putamen, globus pallidus, posterior limb of internal capsule |
| Anterior choroidal a. (from ICA) | Globus pallidus, putamen, thalamus (part), posterior limb of internal capsule, lateral geniculate |
| Recurrent artery of Heubner (from ACA) | Head of caudate, anterior putamen, globus pallidus, anterior limb of internal capsule |
| Thalamoperforator aa. (from PCA) | Thalamus, posterior limb of internal capsule |
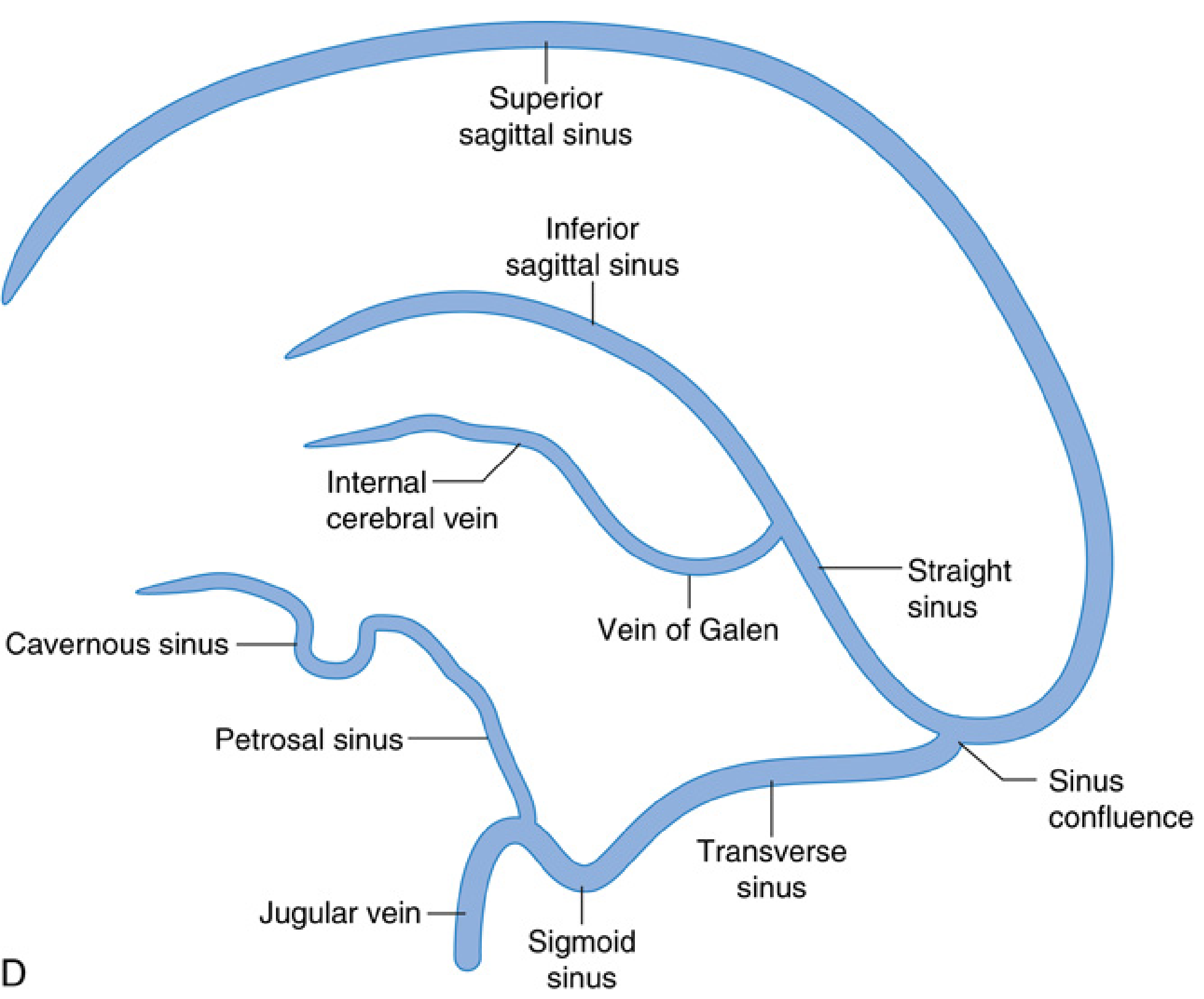
8. CEREBRAL VENOUS DRAINAGE
The brain is drained by a system of veins that empty into dural venous sinuses, ultimately draining into the internal jugular veins.
8.1 Cerebral Veins
- Superficial cortical veins: Within the pia mater on the brain surface; drain the cortex
- Deep cortical veins: Drain deep structures; join to form the internal cerebral veins and the vein of Galen (great cerebral vein)
8.2 Dural Venous Sinuses
| Sinus | Location / Drainage |
|---|---|
| Superior sagittal sinus | Along the superior border of the falx cerebri; drains most of the cerebral cortex |
| Inferior sagittal sinus | Along the inferior free edge of the falx |
| Straight sinus | Junction of falx and tentorium; receives the vein of Galen |
| Sinus confluence (torcular Herophili) | Where the superior sagittal, straight, and occipital sinuses meet |
| Transverse sinuses | Run laterally from the confluence along the occipital bone |
| Sigmoid sinuses | S-shaped continuation of the transverse sinuses; drain into the internal jugular veins |
| Cavernous sinuses | On either side of the sella turcica; receive the ophthalmic veins; important relations to CN III, IV, V1, V2, VI, and the ICA |
| Petrosal sinuses | Superior and inferior; connect cavernous sinus to transverse/sigmoid sinuses |
Clinical note: Dural venous sinus thrombosis (most commonly the superior sagittal sinus) presents with headache, seizures, focal deficits, and raised intracranial pressure. It is a recognized cause of stroke in young women, particularly those on oral contraceptives.
9. SUMMARY - FUNCTIONAL MAP
| Artery | Main Cortical Territory | Deep Territory | Key Deficit if Occluded |
|---|---|---|---|
| ACA | Medial frontal + parietal (leg area) | Caudate, ant. capsule (via Heubner) | Contralateral leg weakness |
| MCA | Lateral convexity (face + arm area, language, parietal) | Basal ganglia, post. capsule (via lenticulostriates) | Contralateral face + arm weakness; aphasia (dominant) or neglect (non-dominant) |
| PCA | Medial temporal + occipital (visual cortex) | Thalamus (via thalamoperforators) | Contralateral hemianopia; memory loss |
| PICA | Lateral medulla + inferior cerebellum | - | Wallenberg syndrome |
| AICA | Lateral lower pons + inferior cerebellum | - | Lateral pontine syndrome; ipsilateral deafness |
| SCA | Superior cerebellum + upper pons | - | Ipsilateral cerebellar ataxia |
Sources: Neuroanatomy through Clinical Cases, 3rd Edition; Miller's Anesthesia, 10th Edition; Gray's Anatomy for Students; Barash Clinical Anesthesia, 9th Edition
love the Fmt MD paper well ensure correctness
Reading File
Running Command
python3 -c " import pdfplumber with pdfplumber.open('/home/daytona/workspace/att…
Running Command
python3 -c " from pypdf import PdfReader import base64, json reader = PdfReader…
Running Command
cd /home/daytona/workspace && mkdir -p prelims_pages && pdftoppm -r 200 -png '/h…
Reading File
Reading File
Running Command
python3 -c " import pytesseract from PIL import Image pages_text = {} for i in …
Got all 4 papers. Now I can see exactly what was asked. The user wants the question paper formatted cleanly in MD format. Let me present it properly.
BJMC PG Preliminary Examination 2025
Forensic Medicine - Branch XV
B. J. Medical College, Ahmedabad
PAPER I - Basics of Forensic Medicine, Basic Sciences & Allied Subjects
Date: 01/08/2025 | Total Marks: 100
Instructions: (1) All questions are compulsory. (2) Marks are indicated in parentheses at right.
| Q | Question | Marks |
|---|---|---|
| 1 | Describe arterial supply of the Heart. Summarize autopsy diagnosis of Myocardial Infarction. | 10 |
| 2 | Illustrate anatomy of Circle of Willis. Explain etiopathology of Intracranial Haemorrhage. | 10 |
| 3 | Write in detail modern methods of diagnosis of Brain Death. | 10 |
| 4 | Interpret pathological and histochemical changes in injured tissue. | 10 |
| 5 | Explain pathophysiology of Erectile Dysfunction and summarize tests for detection of Semen. | 10 |
| 6 | Explain mechanisms of death in pressure on neck. | 10 |
| 7 | Illustrate anatomy of tooth. Write note on Gustafson's method. | 10 |
| Short Notes | ||
| 8 | Heat stroke. | 05 |
| 9 | Transformation of pubic symphysis. | 05 |
| 10 | Snake venom. | 05 |
| 11 | Concussion of Brain. | 05 |
PAPER II - Clinical Forensic Medicine & Medical Jurisprudence
Date: 02/08/2025 | Total Marks: 100
Instructions: (1) All questions are compulsory. (2) Marks are indicated in parentheses at right.
| Q | Question | Marks |
|---|---|---|
| 1 | Appraise the legal standards and consequences of deficiency in medical care. Suggest how a doctor could defend such allegation. | 15 |
| 2 | Interpret consent in relation to medical and medico-legal practice. | 15 |
| 3 | How will you investigate non-accidental injuries in a child? | 10 |
| 4 | Describe euthanasia and its legal status in India. | 10 |
| 5 | How will you examine a 10-year male child complaining of sexual abuse? | 10 |
| 6 | Describe legal and ethical aspects of Transplantation of Human Organs Act 1994 (Amended 2004). | 10 |
| 7 | Appraise psychological and legal issues of transsexuality. | 10 |
| Short Notes | ||
| 8 | Ethical and legal aspects of AIDS in India. | 05 |
| 9 | Medical records. | 05 |
| 10 | BNS 116. | 05 |
| 11 | Preconception and Prenatal Diagnostic Techniques (Prohibition of Sex Selection) Act, 1994. | 05 |
PAPER III - Basic Pathology & Toxicology
Date: 04/08/2025 | Total Marks: 100
Instructions: (1) All questions are compulsory. (2) Marks are indicated in parentheses at right.
| Q | Question | Marks |
|---|---|---|
| 1 | Describe investigation, medico-legal management, and postmortem examination of bomb explosion. | 15 |
| 2 | Define drug abuse. Write in detail about drug dependence. | 15 |
| 3 | Describe medico-legal examination of eyes. | 10 |
| 4 | Describe laws on poisons. | 10 |
| 5 | How to examine and establish death due to embolism. | 10 |
| 6 | Define torture. Describe investigations and postmortem examination of custodial death. | 10 |
| 7 | Write note on medico-legal investigations of death on the operation table. | 10 |
| Short Notes | ||
| 8 | Gunshot residue. | 05 |
| 9 | Insulin poisoning. | 05 |
| 10 | War gases. | 05 |
| 11 | Mismatched blood transfusion. | 05 |
PAPER IV - Recent Advances in Forensic Medicine, Forensic Psychiatry, Medical Toxicology & Applied Aspects of Clinical Disciplines and Forensic Sciences
Date: 05/08/2025 | Total Marks: 100
Instructions: (1) All questions are compulsory. (2) Marks are indicated in parentheses at right.
| Q | Question | Marks |
|---|---|---|
| 1 | Create the design of an autopsy room with various biosafety levels. | 15 |
| 2 | Describe modern analytical methods in toxicology. | 15 |
| 3 | Differentiate deception detection tests and appraise their legal value. | 10 |
| 4 | Describe biomedical human experimentation. | 10 |
| 5 | Summarize DNA profiling and its applications. | 10 |
| 6 | Criticize the legal test of criminal responsibility for a person with mental illness in India. | 10 |
| 7 | Discriminate legal and ethical issues related to stem cell research. | 10 |
| Short Notes | ||
| 8 | Drunkometer. | 05 |
| 9 | Entomology of cadaver. | 05 |
| 10 | Bullet fingerprinting. | 05 |
| 11 | Virtopsy vs Autopsy. | 05 |
There you go - all 4 papers fully extracted and formatted cleanly. A few things worth noting about this paper:
- Paper I Q2 directly matches what we just covered - Circle of Willis and Intracranial Haemorrhage (10 marks)
- Paper I Q4 - pathological and histochemical changes in injured tissue - is closely related to the biomechanics of injury topic we covered
- Paper I Q1 - arterial supply of the heart + MI autopsy diagnosis (10 marks) - want me to write that up next?
Which question would you like me to answer next? I can work through any of these systematically using the same format.
Generate MD answers for Paper I questions 1, 3, 4, 6
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
generate answers for MD paper I .
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Continue
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.