Hi, I am a final year MBBS student in dr..mgr tamilnadu medical University. Tell me about necrotising enterocolitis in neonates
Reading File
Finding Sources
Finding Sources
Searching PubMed
"necrotizing enterocolitis"[MeSH Terms] AND neonates
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Necrotising Enterocolitis (NEC) in Neonates
NEC is the most common gastrointestinal emergency in the neonatal period and a devastating complication of prematurity. Here is a complete breakdown for your MBBS finals.
Definition & Epidemiology
- NEC is characterized by intestinal inflammation that can progress to transmural necrosis and perforation.
- Affects 1-5% of all NICU admissions overall; 4-13% of very low birth weight (VLBW) infants (<1500 g).
- Incidence is inversely proportional to gestational age - the more premature the infant, the higher the risk; peak incidence at ~32 weeks corrected gestational age.
- Mortality: 10-30% overall; up to 50% in infants requiring surgery.
- 80% of cases occur in the first month of life, typically after enteral feeds are initiated.
(Creasy & Resnik's Maternal-Fetal Medicine; Sabiston Textbook of Surgery)
Pathogenesis (Multifactorial)
Three core mechanisms interact:
| Mechanism | Detail |
|---|---|
| Intestinal immaturity | Abnormal bowel motility, immature vascular supply, poor epithelial barrier function, immature mucosal immune defense |
| Gut microbiome disruption | Abnormal colonization by pathogenic bacteria; prolonged antibiotic use disturbs normal flora; infectious clusters occur in NICUs |
| Exaggerated inflammatory response | Cytokine/chemokine release; platelet-activating factor (PAF) promotes enterocyte apoptosis and compromises tight junctions, increasing mucosal permeability; TLR4 activation increases gut ischemia in response to pathogenic bacteria |
- NEC is almost exclusively seen in infants who have received enteral feeds, suggesting postnatal bacterial introduction triggers the cascade.
- In term neonates, NEC is often associated with congenital heart disease, perinatal asphyxia, and hypoxia/low-flow states (so-called "term-NEC").
(Robbins Basic Pathology; Fischer's Mastery of Surgery; Grainger & Allison Diagnostic Radiology)
Risk Factors
Antenatal:
- Prematurity and low birth weight (most significant)
- Indomethacin tocolysis (especially double-agent tocolytic therapy)
- Protective: antenatal corticosteroid administration
Postnatal:
- Formula feeding (vs. human milk)
- Rapid advancement of feeds
- Prolonged antibiotic use
- Multiple blood transfusions
- Hypoxia/ischaemia (especially in term infants with congenital cardiac disease)
- Exposure to enteric pathogens (cluster outbreaks)
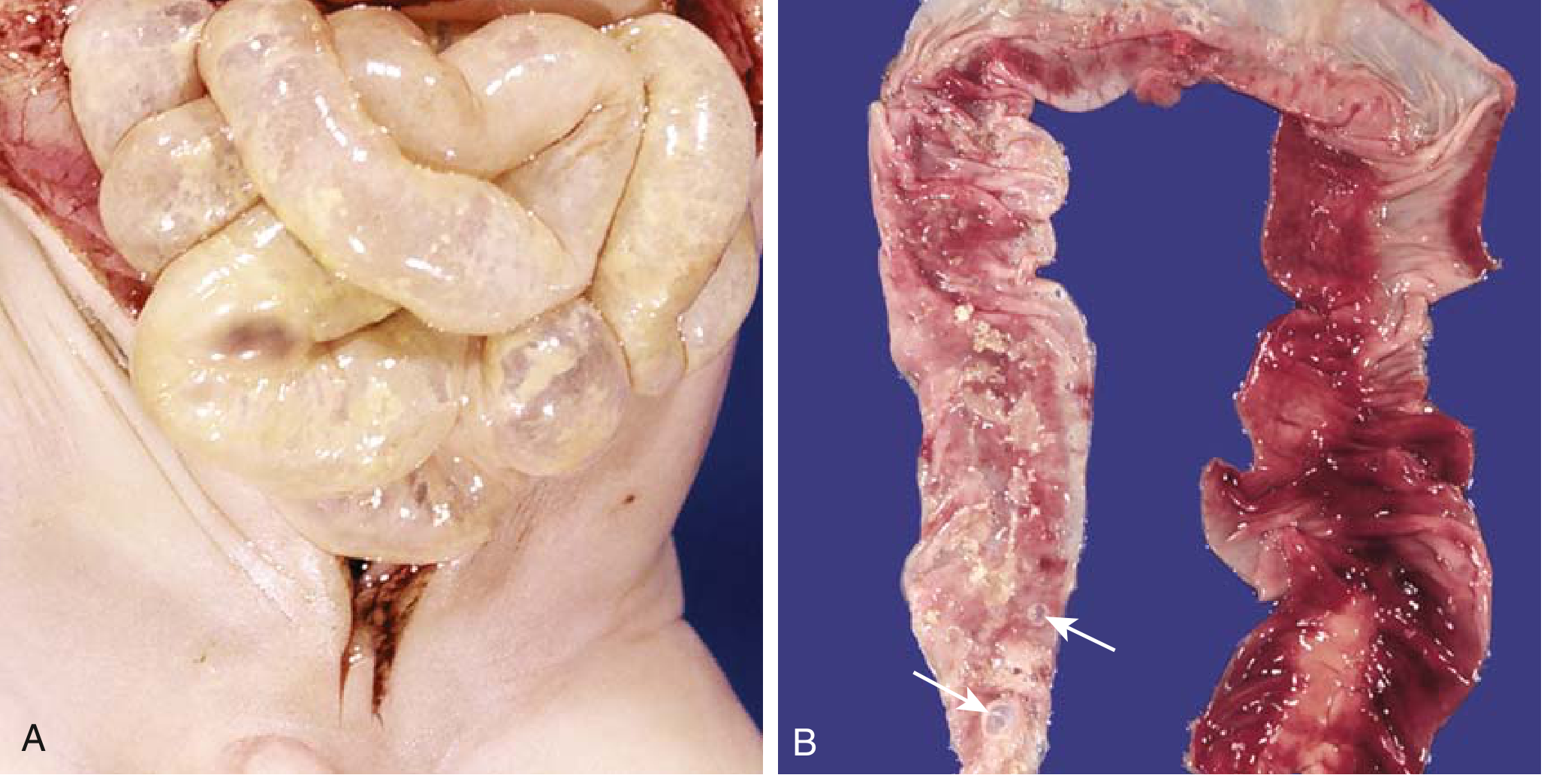
Pathology (Morphology)
Macroscopic:
- Most commonly involves: terminal ileum, cecum, and right colon (any segment can be involved)
- Bowel is distended, friable, congested, or gangrenous
- Perforation and peritonitis may be present
Microscopic:
- Mucosal or transmural coagulative necrosis
- Ulceration
- Bacterial colonization
- Submucosal gas bubbles (pneumatosis intestinalis)
- Granulation tissue and fibrosis (in healing phase)
Clinical Features
Systemic (non-specific early signs):
- Temperature instability
- Lethargy, apnea, bradycardia
- Hypoglycaemia, oxygen desaturation
GI signs (more specific):
- Feeding intolerance, increased gastric residuals
- Abdominal distension and tenderness
- Bloody stools (occult or gross)
- Vomiting, diarrhoea
Advanced signs:
- Abdominal wall erythema and oedema (cellulitis)
- Blue discolouration of the abdomen (perforation)
- Visible dilated bowel loops through thin abdominal wall
- Septic shock, DIC, cardiovascular collapse
Lab findings:
- Thrombocytopenia, leukocytosis or leukopenia
- Elevated CRP, elevated lactate
- Metabolic acidosis, respiratory acidosis
Bell Staging Criteria (Bell et al., 1978 - Ann Surg)
This is the classic clinical staging system used to guide management:
| Stage | Systemic Signs | GI Signs | Radiographic Findings |
|---|---|---|---|
| I - Suspected | Temperature instability, lethargy, apnea, bradycardia | Poor feeding, ↑ gastric residuals, emesis, mild abdominal distension, occult blood in stools | Distension with mild ileus |
| II - Definite | (as above) | Persistent occult or gross GI bleeding, marked abdominal distension | Marked intestinal distension, small bowel separation/oedema, pneumatosis intestinalis, portal venous gas |
| III - Advanced | Deterioration of vital signs, septic shock | - | Pneumoperitoneum (free air) |
(Fischer's Mastery of Surgery, 8th ed.)
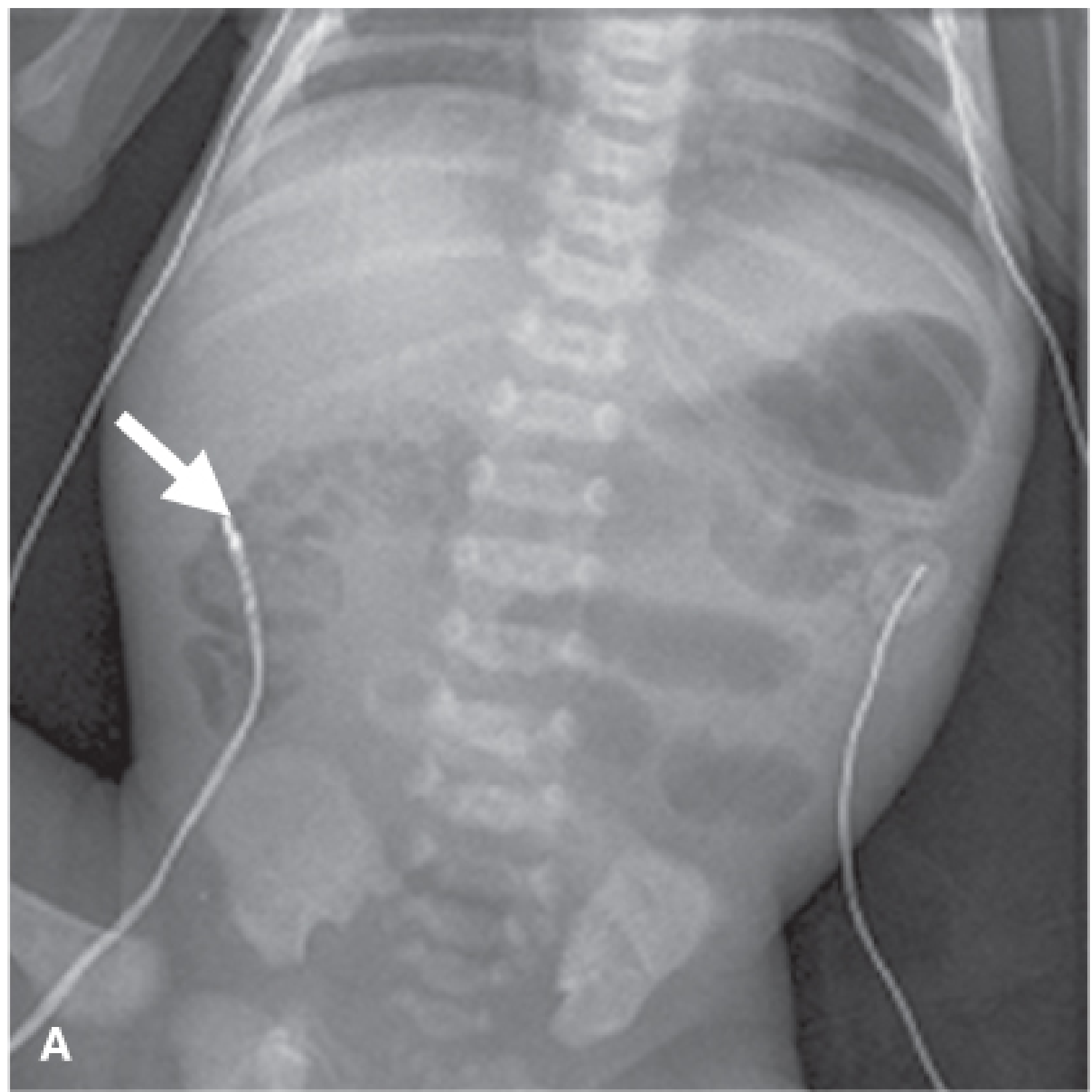
Radiological Features
Four key X-ray signs (in order of significance):
- Non-specific global bowel dilatation - earliest, non-specific
- Persistent/fixed bowel loop - on serial X-rays, same loop doesn't change position - poor prognostic sign
- Pneumatosis intestinalis - pathognomonic; intramural gas (hydrogen from bacterial fermentation); seen as bubbly or linear lucencies in the bowel wall
- Portal venous gas - branching linear lucencies over liver radiating from porta hepatis; seen in ~30%, indicates severe disease
- Pneumoperitoneum (free air) - indicates perforation; absolute indication for surgery
Ultrasound may reveal: portal venous gas, bowel wall thickening, complex ascites (indicating perforation).
Management
Medical (>50% of cases can be managed without surgery)
- Nil per mouth (NPO) - stop all enteral feeds
- Orogastric tube decompression
- IV fluid resuscitation
- Broad-spectrum antibiotics (covering gram-negative organisms and anaerobes)
- Serial abdominal X-rays (every 6-8 hours initially)
- Close monitoring for surgical indications
Surgical Indications
| Absolute | Relative |
|---|---|
| Pneumoperitoneum (free air) | Clinical deterioration |
| Persistent metabolic acidosis | |
| Abdominal wall cellulitis | |
| Palpable abdominal mass (matted ischemic bowel) | |
| Persistent fixed bowel loop on X-ray | |
| Portal venous gas |
Surgical Options
- Exploratory laparotomy - resection of all nonviable segments; preserving maximum intestinal length
- Ostomy creation - common; allows bowel rest and later anastomosis
- Second-look laparotomy - at 24-48 hours for marginally viable bowel
- Peritoneal drainage (bedside) - for extremely low birth weight (<1500 g) infants with perforated NEC; effective as temporizing or definitive treatment; outcomes comparable to laparotomy in VLBW infants (established by multicenter RCT)
- Primary anastomosis - only in rare, very stable infants with focal, isolated perforation
Prevention
- Human breast milk - fourfold decrease in NEC risk (RR 0.25; meta-analysis of RCTs); all mothers of at-risk infants (<32 weeks) should be encouraged strongly
- Antenatal corticosteroids - protective
- Gradual, protocol-based feeding advancement
- Probiotics - evidence is low; not yet standard of care
Complications & Prognosis
- Short bowel syndrome (SBS) - after extensive bowel resection
- Post-NEC strictures - in ~10% of infants (most commonly at the splenic flexure); develop after both medical and surgical management; a contrast enema should be done before ostomy reversal
- Adhesions - may cause late intestinal obstruction
- High mortality, especially in surgical cases (up to 50%)
- NEC totalis (involvement of entire GI tract) - near-universally fatal
Key Points to Remember for Exams
- Most common GI emergency in neonates; most significant risk factor = prematurity
- Pathognomonic finding: pneumatosis intestinalis on X-ray
- Absolute surgical indication: pneumoperitoneum
- Bell staging classifies disease into I (suspected), II (definite), III (advanced)
- Human breast milk is the single most important preventive measure
- Terminal ileum and right colon are most commonly affected
- Portal venous gas is a poor prognostic indicator
- ~10% develop post-NEC strictures even after conservative management
This is a shared conversation. Sign in to Orris to start your own chat.