
Give answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information needed. Here are detailed answers to all questions in the paper:
Sri Aurobindo Medical College - Physiology Paper 1, Section B
Q1 CASE: 45-year-old male with indigestion, diarrhea, angular stomatitis, peripheral neuropathy; Hb 9 g%, MCV 100 fL, MCH 50 pg, RBC 1 million/cc, S. Iron 170 mcg/dL, macrocytic normochromic PBF with hypersegmented neutrophils
Q.1 What is the diagnosis? [1 mark]
Megaloblastic Anemia due to Vitamin B12 (Cobalamin) Deficiency
This is the classic presentation: macrocytic (MCV 100 fL - elevated), normochromic anemia with Hb 9 g%, hypersegmented neutrophils on PBF, angular stomatitis (glossitis), peripheral neuropathy, and pancytopenia. Normal serum iron rules out iron deficiency.
Q.2 What are the causes of this type of anemia? [1 mark]
The two major causes of megaloblastic anemia are Vitamin B12 deficiency and Folate deficiency.
Causes of Vitamin B12 deficiency specifically:
- Lack of Intrinsic Factor (IF): Pernicious anemia (autoimmune type A gastritis), total gastrectomy, congenital IF defect
- Malabsorption: Atrophic gastritis, ileal disease (Crohn's, resection), pancreatic exocrine insufficiency, bacterial overgrowth, tapeworm (Diphyllobothrium latum)
- Nutritional: Strict vegan/vegetarian diet, breast-fed infant of deficient mother
- Drugs: Metformin, nitrous oxide, proton pump inhibitors
- Congenital errors of B12 metabolism
Causes of Folate deficiency:
- Poor diet (lack of green leafy vegetables, fruits)
- Alcohol abuse
- Malabsorption (celiac, tropical sprue)
- Increased demand (pregnancy, hemolytic anemia)
- Drugs (methotrexate, phenytoin)
(Source: Goldman-Cecil Medicine, Table 150-2)
Q.3 What is the cause of peripheral neuropathy in this type of anemia? [1 mark]
Demyelination of the posterior and lateral columns of the spinal cord - this is called Subacute Combined Degeneration (SCD) of the spinal cord.
Mechanism: Vitamin B12 is required as a cofactor for methionine synthase, which converts homocysteine to methionine. Methionine is needed for S-adenosylmethionine (SAM) synthesis. SAM is the methyl donor required for myelin synthesis. Without B12, methylation of myelin basic proteins is impaired, leading to demyelination. This causes tingling/numbness in hands and feet (peripheral neuropathy) and may progress to spastic paraparesis if untreated.
Note: Folate deficiency does NOT cause peripheral neuropathy - this distinction is clinically important.
Q.4 What do you understand by macrocytic and normochromic RBCs? [1 mark]
-
Macrocytic RBC: RBCs that are larger than normal. Normal MCV = 80-100 fL. In this patient, MCV = 100 fL (borderline macrocytic/macrocytic). In megaloblastic anemia, MCV is often >110 fL in fully developed cases. The increased cell size is due to impaired DNA synthesis while cytoplasmic RNA/protein synthesis continues normally, causing a nuclear-cytoplasmic dyssynchrony - the cell grows in size but cannot divide.
-
Normochromic RBC: RBCs that have normal hemoglobin content per cell. Normal MCH = 27-33 pg. In this patient, MCH = 50 pg (actually elevated/hyperchromic, consistent with larger cells). Normal MCHC means the hemoglobin concentration within the cell is normal - the cell is not pale (not hypochromic), distinguishing this from iron deficiency anemia.
This pattern (macrocytic + normochromic) is the hallmark of megaloblastic anemia and contrasts with microcytic hypochromic anemia seen in iron deficiency.
Q.5 Why do you see large nucleated RBCs (megaloblasts) in PBF in this condition? [1 mark]
Mechanism - Thymidine Trap / DNA Synthesis Failure:
- Vitamin B12 is required to convert methyltetrahydrofolate (methyl-THF) to tetrahydrofolate (THF).
- THF is needed to synthesize thymidylate (thymidine monophosphate) for DNA replication via thymidylate synthase.
- Without B12, folate is trapped as methyl-THF and cannot be converted to active THF - this is the "folate trap" or "thymidine trap."
- DNA synthesis is impaired, so the nucleus cannot undergo normal division and maturation.
- However, RNA and cytoplasmic protein synthesis continue normally (RNA synthesis does not need THF).
- This creates nuclear-cytoplasmic dyssynchrony: the cytoplasm matures and enlarges while the nucleus remains immature and large.
- These abnormal large cells with immature nuclei are called megaloblasts.
- They undergo maturation arrest in the bone marrow and some escape into circulation as large nucleated RBCs.
- They are also destroyed prematurely in the marrow (ineffective erythropoiesis), accounting for the elevated reticulocyte count and raised serum LDH.
(Source: Goldman-Cecil Medicine, Section: Megaloblastic Anemia - Definition)
Q.6 How is the deficient nutrient (Vitamin B12) absorbed and utilized in the body? [1 mark]
Absorption of Vitamin B12:
- Mouth: Dietary B12 (bound to food protein) is released by pepsin and gastric acid in the stomach. It then binds to Haptocorrin (R-protein) secreted in saliva.
- Duodenum: Pancreatic proteases digest the HC-B12 complex, releasing B12 which then binds to Intrinsic Factor (IF) - a glycoprotein secreted by parietal cells of gastric fundus/body.
- Terminal Ileum: The IF-B12 complex binds to the Cubam receptor (cubilin + amnionless protein) on ileal mucosal cells and is internalized into lysosomes.
- Blood Transport: B12 is exported from lysosomes into the cytoplasm and then bound to Transcobalamin (TC) - the physiological delivery protein. The TC-B12 complex enters circulation and is taken up by cells via CD320 receptor.
Utilization:
- Methyl-cobalamin acts as cofactor for methionine synthase (converts homocysteine → methionine; regenerates THF for DNA synthesis)
- Adenosyl-cobalamin acts as cofactor for L-methylmalonyl-CoA mutase (converts methylmalonyl-CoA → succinyl-CoA; important in fatty acid and amino acid metabolism)
(Source: Goldman-Cecil Medicine, Section: Cobalamin Absorption)
Q.7 Why is this type of anemia seen in patients with gastric atrophy? [1 mark]
In gastric atrophy (autoimmune - Pernicious Anemia):
- The immune system attacks the gastric mucosa (fundus and body), specifically targeting H+/K+ ATPase in parietal cells.
- This leads to:
- Loss of parietal cells → loss of Intrinsic Factor (IF) secretion
- Achlorhydria (loss of gastric acid) → B12 cannot be released from food protein
- Without IF, the B12-IF complex cannot form, so B12 cannot bind the cubam receptor in the terminal ileum.
- Result: B12 malabsorption despite adequate dietary intake → megaloblastic anemia after body stores (2-5 years supply) are depleted.
- Autoantibodies against IF ("anti-IF antibodies") and parietal cells can be detected in blood (diagnostic marker).
In Type B atrophic gastritis (H. pylori-related): achlorhydria prevents protein-bound B12 absorption, causing protein-bound cobalamin malabsorption.
Q.8 How will you manage this patient? [1 mark]
Management of Vitamin B12 Deficiency Megaloblastic Anemia:
-
Confirm diagnosis: Serum B12 level (low), serum folate, check for anti-IF antibodies (if pernicious anemia suspected), reticulocyte count, LDH, bilirubin (elevated from ineffective erythropoiesis).
-
Vitamin B12 Replacement:
- IM Cyanocobalamin or Hydroxocobalamin: 1000 mcg IM daily for 1 week, then weekly for 4 weeks, then monthly for life (if pernicious anemia/malabsorption)
- Oral Cyanocobalamin: 1000-2000 mcg/day (effective even without IF due to passive absorption at high doses)
-
Folic Acid: Give supplemental folate if folate deficiency co-exists (but MUST confirm B12 is also replaced - see Q.9).
-
Monitor: Reticulocyte crisis within 3-5 days of treatment (confirms diagnosis), Hb normalizes over 6-8 weeks, peripheral neuropathy may take longer or may be permanent.
-
Treat underlying cause: H. pylori eradication, diet counseling for vegetarians, treat underlying GI disease.
Q.9 What will happen if you give only folic acid supplementation in pernicious anemia? [1 mark]
This is a clinically dangerous situation:
Folic acid corrects the hematological features but NOT the neurological complications.
- Supplemental folate bypasses the "folate trap" and can partially restore DNA synthesis, so the anemia and macrocytosis may improve or even normalize.
- However, the underlying Vitamin B12 deficiency continues undetected.
- The subacute combined degeneration of the spinal cord (posterior and lateral column demyelination) continues to progress silently.
- The patient may develop irreversible neurological damage - spastic paraparesis, sensory ataxia, dementia - while the blood counts look normal, giving a false sense of security.
This is why it is mandatory to always rule out B12 deficiency before starting folate therapy in any patient with megaloblastic anemia. Giving folate alone to a B12-deficient patient can lead to permanent neurological disability.
Q.10 What is the mode of action of Vitamin B12 and Folic Acid in erythropoiesis? [1 mark]
Folic Acid (as Tetrahydrofolate - THF):
- Serves as a one-carbon donor in the synthesis of thymidylate (dTMP) from dUMP via thymidylate synthase.
- Also required for purine synthesis (adenine, guanine).
- Both thymidine and purines are essential building blocks for DNA replication.
- Without adequate folate, DNA synthesis fails → impaired cell division → megaloblastic changes in all rapidly dividing cells, especially erythroblasts in bone marrow.
Vitamin B12 (Cobalamin):
- Acts as a cofactor for methionine synthase: Methyl-THF + Homocysteine → THF + Methionine
- This reaction regenerates active THF from the inactive methyl-THF form.
- Active THF is required for the folate-dependent reactions above (thymidine and purine synthesis).
- Without B12, folate is trapped as methyl-THF and cannot enter the folate cycle - this is the "methylfolate trap".
- Additionally, B12 (as adenosyl-cobalamin) is needed for normal fatty acid metabolism via methylmalonyl-CoA mutase - deficiency here leads to abnormal myelin.
In summary: Both vitamins are interdependent - B12 deficiency functionally creates a folate deficiency for purposes of DNA synthesis, even if dietary folate is adequate. Both are needed for normal erythropoiesis by ensuring rapid DNA replication in erythroblasts.
Q2. Different Types of Cell Junctions [10 marks]
Intercellular junctions are specialized structures between adjacent cells. They fall into two broad groups: anchoring junctions (hold cells together or to matrix) and communicating junctions (allow transfer of signals).
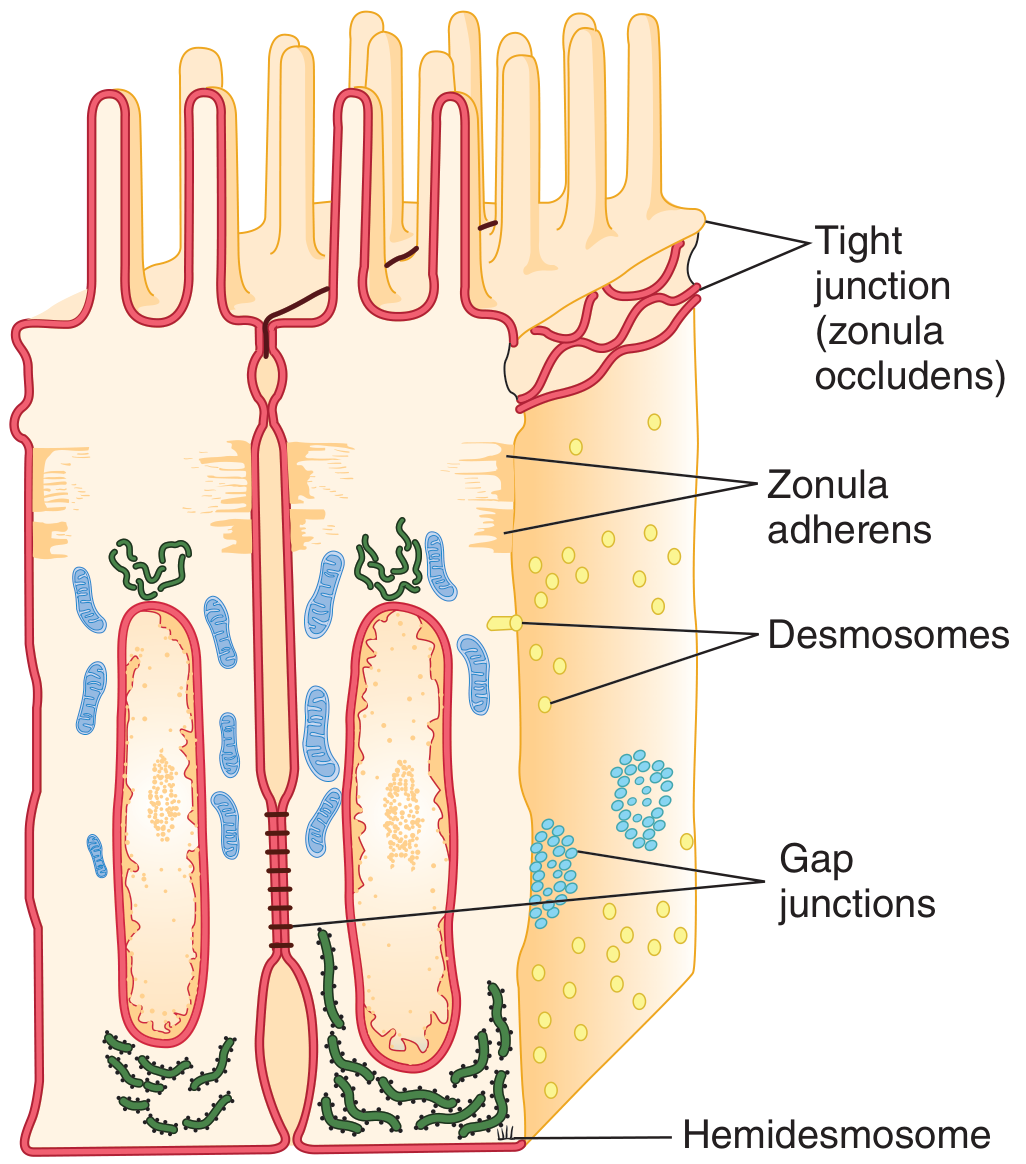
1. Tight Junctions (Zonula Occludens)
- Located at the apical margin of epithelial cells (e.g., intestinal mucosa, renal tubules, choroid plexus, blood-brain barrier).
- Formed by transmembrane proteins: occludin, claudins, junctional adhesion molecules (JAMs); intracellularly anchored by zonula occludens proteins (ZO-1, ZO-2).
- The two cell membranes are so closely fused they virtually obliterate the intercellular space.
- Function:
- Act as a barrier preventing paracellular passage of large molecules between the apical and basolateral compartments (e.g., prevent gut contents from leaking into bloodstream)
- Maintain cell polarity by preventing lateral diffusion of membrane proteins between apical and basolateral domains
- Degree of "leakiness" varies by claudin composition
2. Adherens Junctions (Zonula Adherens)
- Located just basal to the tight junction (together they form the "junctional complex")
- Transmembrane proteins: cadherins (calcium-dependent cell adhesion molecules), linked intracellularly to actin microfilaments via catenins
- Function: Mechanical anchorage between cells; major site of attachment for actin cytoskeleton; maintain tissue integrity under mechanical stress
3. Desmosomes (Macula Adherens)
- Disc-shaped patches of dense material on opposing cell membranes
- Transmembrane proteins: cadherins (desmoglein, desmocollin), intracellularly linked to intermediate filaments (keratin/tonofilaments), not actin
- Function: Provide strong mechanical attachment between cells - abundant in tissues subject to mechanical stress (skin epidermis, cardiac muscle, uterine epithelium)
- Clinical relevance: Pemphigus vulgaris (autoantibodies against desmoglein 3 cause skin blistering)
4. Hemidesmosomes
- Appear as "half-desmosomes" on the basal surface of epithelial cells
- Transmembrane proteins: integrins (not cadherins), linked to intermediate filaments intracellularly
- Attach cells to the basal lamina (extracellular matrix)
- Function: Anchor epithelium to underlying connective tissue
5. Focal Adhesions
- Also attach cells to the basal lamina via integrins
- Linked intracellularly to actin stress fibers
- Important in cell migration and mechanotransduction
6. Gap Junctions (Nexus)
- Formed by connexins - 6 connexin subunits form a hemichannel (connexon); two connexons from opposing cells align to form a complete gap junction channel
- The intercellular space is only ~2-3 nm (compared to ~20 nm elsewhere)
- Each channel allows passage of molecules <1000 Da (ions, cAMP, small metabolites) - NOT proteins
- Function:
- Electrical coupling: Allow action potential propagation in cardiac and smooth muscle (cardiac syncytium)
- Chemical coupling: Allow passage of second messengers (IP3, cAMP) for coordinated cellular responses
- Found in liver, cardiac muscle, smooth muscle, lens of eye, astrocytes
| Junction Type | Transmembrane Protein | Intracellular Linkage | Main Function |
|---|---|---|---|
| Tight Junction | Occludin, Claudin, JAM | ZO proteins | Paracellular barrier, cell polarity |
| Zonula Adherens | Cadherin | Actin (via catenins) | Mechanical adhesion |
| Desmosome | Desmoglein/Desmocollin | Intermediate filaments | Strong cell-cell adhesion |
| Hemidesmosome | Integrin | Intermediate filaments | Cell-ECM adhesion |
| Gap Junction | Connexin | None (channels) | Cell-cell communication |
Q3. Resting Membrane Potential (RMP) and Gibbs-Donnan Equilibrium [10 marks]
Definition of RMP
The resting membrane potential is the electrical potential difference that exists across the cell membrane of an excitable cell (nerve, muscle) in the resting state (between action potentials). By convention, it is expressed as the intracellular voltage relative to the extracellular (extracellular = 0 mV). In most excitable cells, RMP = -70 to -90 mV (inside negative).
Ionic Basis of RMP
The RMP is generated by differential ion permeabilities across the membrane, driven by concentration gradients established by active transport pumps:
| Ion | Intracellular | Extracellular | Equilibrium Potential |
|---|---|---|---|
| K+ | 140 mEq/L | 4 mEq/L | -94 mV |
| Na+ | 14 mEq/L | 140 mEq/L | +61 mV |
| Cl- | 4 mEq/L | 114 mEq/L | -90 mV |
| Ca2+ | 0.0001 mM | 1.2 mM | +132 mV |
At rest, the membrane is highly permeable to K+ and Cl- but poorly permeable to Na+ and Ca2+. Therefore, RMP is close to K+ equilibrium potential (-94 mV), dragged slightly positive by small Na+ leak.
Chord Conductance Equation
The contribution of each ion can be calculated by the chord conductance equation (Costanzo Physiology):
$$E_m = \frac{G_{K^+}}{G_T}E_{K^+} + \frac{G_{Na^+}}{G_T}E_{Na^+} + \frac{G_{Cl^-}}{G_T}E_{Cl^-}$$
Ions with the highest conductance (K+, Cl-) dominate the RMP.
Role of Na+/K+ ATPase
The Na+/K+ ATPase contributes to RMP in two ways:
- Direct electrogenic effect: Pumps 3 Na+ out for every 2 K+ in → net negative charge inside (small contribution, ~-5 mV)
- Indirect effect (more important): Maintains the high intracellular K+ and low intracellular Na+ concentration gradients, which drive the K+ diffusion potential that is the primary determinant of RMP.
Gibbs-Donnan Equilibrium
Definition: A state of equilibrium reached when a membrane permeable to small ions but impermeable to large charged molecules (like proteins) separates two solutions. The presence of impermeable charged macromolecules (anions) on one side causes unequal distribution of permeant ions across the membrane.
Key features (Medical Physiology - Boulpaep & Boron):
- The cell interior contains large, negatively charged, impermeant proteins (designated Y-)
- These negative charges attract cations (Na+, K+) and repel anions (Cl-) into the cell
- At Gibbs-Donnan equilibrium, the Donnan ratio r must be equal for all permeant ions:
$$\frac{[Na^+]_o}{[Na^+]_i} = \frac{[Cl^-]_i}{[Cl^-]_o} = r$$
- This creates a membrane potential (Donnan potential) with the side containing the impermeant anions being electrically negative
- The redistribution also causes an osmotic imbalance - more osmotically active particles accumulate on the protein-containing side (the cell interior)
- This osmotic imbalance would cause water to enter the cell, leading to cell swelling if unopposed
Why don't cells swell?: Achieving true Gibbs-Donnan equilibrium would require 967 mm Hg of hydrostatic pressure to oppose water entry. Living cells prevent this by the active Na+/K+ ATPase pump, which continuously pumps Na+ out of the cell, counteracting the Donnan-driven Na+ entry and maintaining osmotic balance. This is called the pump-leak model.
Relationship of Donnan Equilibrium to RMP:
- Gibbs-Donnan forces contribute to the resting membrane potential by creating ionic asymmetry
- In capillaries: plasma proteins create a Donnan equilibrium that causes slightly higher [Na+] and [Ca2+] in plasma vs. interstitial fluid (Donnan factor ~1.05), which accounts for part of the oncotic pressure difference
Generation of RMP - Summary
- Na+/K+ ATPase establishes ion concentration gradients (3 Na+ out, 2 K+ in per cycle)
- High K+ permeability at rest → K+ diffuses out down its gradient → leaves negative charges behind → inside becomes negative
- This negative interior repels further K+ efflux and attracts Na+ slightly
- The RMP settles at ~-70 to -90 mV where the electrical force inward on K+ equals the chemical force outward
- Gibbs-Donnan equilibrium due to intracellular proteins adds to this negativity
- The final RMP reflects the weighted average of all ionic equilibrium potentials (Goldman equation)
All answers are based on authoritative sources: Goldman-Cecil Medicine (25th Ed.), Costanzo Physiology (7th Ed.), Ganong's Review of Medical Physiology (26th Ed.), Medical Physiology (Boulpaep & Boron).
This is a shared conversation. Sign in to Orris to start your own chat.