parathyroid gland and its disorders in detail trousseau sign calcium levels
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile this into a detailed, well-organized response.
Parathyroid Gland: Anatomy, Physiology, and Disorders
1. Anatomy and Embryology
Humans normally have four parathyroid glands located on the posterior surface of the thyroid lobes (two superior, two inferior). Their combined weight is less than 500 mg.
Embryological origin:
- Superior parathyroids - endoderm of the 4th pharyngeal pouch
- Inferior parathyroids - endoderm of the 3rd pharyngeal pouch (same origin as the thymus)
Ectopic parathyroid tissue (present in 3-5% of the population) may be found along the embryological migratory path, within the thymus, or within the thyroid itself.
Cell types:
- Chief cells - responsible for synthesis and secretion of PTH
- Oxyphil cells - function less well understood; found in adenomas
2. Parathyroid Hormone (PTH): Synthesis and Actions
PTH is an 84-amino acid peptide encoded by a gene on chromosome 11p15. It is synthesized as pre-pro-PTH (115 aa) → pro-PTH (90 aa) → mature PTH (84 aa).
Key regulators of PTH secretion:
| Stimulus | Effect on PTH |
|---|---|
| Low ionized Ca²+ | Increases PTH (primary stimulus) |
| High ionized Ca²+ | Decreases PTH (via calcium-sensing receptor) |
| Vitamin D (1,25-dihydroxyvitamin D) | Decreases PTH transcription |
| Hyperphosphatemia | Increases PTH release |
Calcium-Sensing Receptor (CaSR): A G-protein-coupled receptor (GPCR) on parathyroid chief cells and renal tubular cells. When activated by elevated Ca²+, it triggers phospholipase C, raising intracellular Ca²+ and suppressing PTH release.
Actions of PTH:
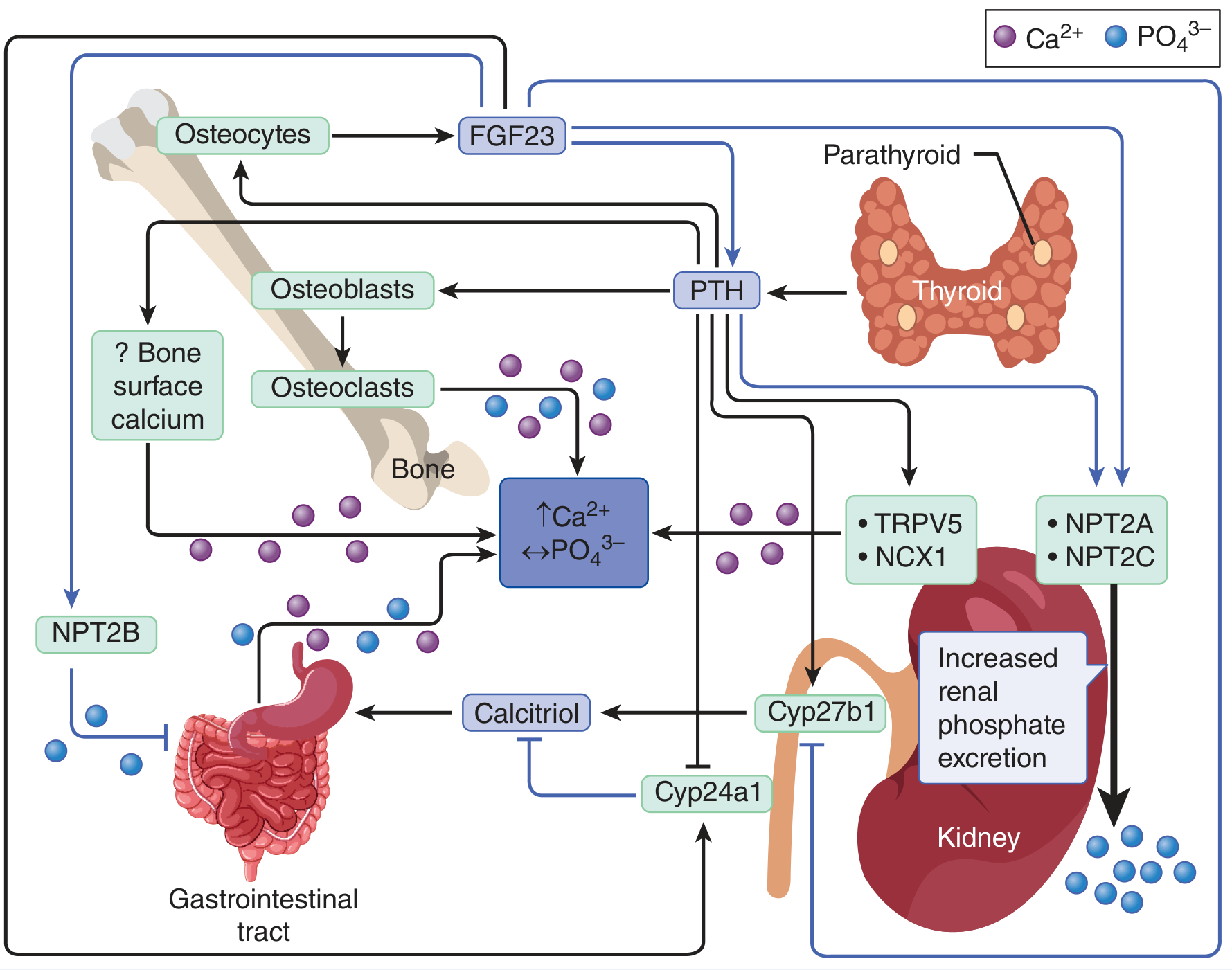
| Target Organ | Effect |
|---|---|
| Bone | Stimulates osteoclasts (via osteoblasts) → Ca²+ and PO₄³⁻ release |
| Kidney (proximal tubule) | Increases Ca²+ reabsorption; promotes phosphaturia (via NPT2A/2C); stimulates Cyp27b1 to convert 25-OH-D to 1,25(OH)₂D (calcitriol) |
| GI tract (indirect) | Via calcitriol, increases intestinal Ca²+ and PO₄ absorption (via NPT2B) |
| Net result | Increases serum Ca²+; decreases serum phosphate |
3. Normal Calcium Levels and Homeostasis
| Form | Normal Range |
|---|---|
| Total serum calcium | 8.5-10.5 mg/dL (2.12-2.62 mmol/L) |
| Ionized calcium | 4.5-5.1 mg/dL (1.1-1.3 mmol/L) |
| Hypercalcemia threshold | Serum adjusted Ca > 10.5 mg/dL or ionized Ca > 5.25 mg/dL (1.31 mmol/L) |
| Hypocalcemia threshold | Serum adjusted Ca < 8.8 mg/dL or ionized Ca < 4.4 mg/dL (1.1 mmol/L) |
About 45% of total serum calcium is bound to albumin, 10% is complexed with anions (citrate, phosphate), and 45% is the free ionized fraction (the biologically active form). To correct for hypoalbuminemia: add 0.8 mg/dL to total calcium for every 1 g/dL that albumin is below 4 g/dL.
Fine-tuned by:
- PTH (main regulator)
- 1,25-dihydroxyvitamin D (calcitriol) - raises Ca via GI absorption
- Calcitonin (from thyroid C-cells) - lowers Ca by inhibiting osteoclasts (minor role in adults)
- FGF23 (from osteocytes) - inhibits calcitriol production, promotes phosphate excretion
4. Hyperparathyroidism
A. Primary Hyperparathyroidism
Definition: Autonomous excess PTH secretion from one or more parathyroid glands.
Epidemiology: Affects ~3 in 1000 adults; most common cause of asymptomatic hypercalcemia in outpatients.
Etiology:
| Cause | Frequency |
|---|---|
| Sporadic parathyroid adenoma (single gland) | ~85% |
| Multiglandular hyperplasia | ~12-15% |
| Parathyroid carcinoma | <1% |
| MEN1 or MEN2A (familial) | Rare |
MEN associations:
- MEN1: Parathyroid hyperplasia + pituitary adenoma + pancreatic tumors
- MEN2A: Parathyroid hyperplasia + medullary thyroid carcinoma + pheochromocytoma
- HPT-JT syndrome: Parathyroid tumor + jaw fibroma (CDC73/parafibromin mutations)
Classic Clinical Features - "Stones, Bones, Abdominal Groans, Psychic Moans":
| System | Manifestations |
|---|---|
| Renal (Stones) | Nephrolithiasis (calcium oxalate/phosphate stones), nephrocalcinosis, polyuria/polydipsia |
| Skeletal (Bones) | Osteitis fibrosa cystica, subperiosteal bone resorption (radial aspect of middle phalanx), brown tumors, osteoporosis |
| GI (Abdominal groans) | Nausea, vomiting, constipation, anorexia, peptic ulcer disease, pancreatitis |
| Neuropsychiatric (Psychic moans) | Depression, anxiety, cognitive dysfunction, lethargy, stupor (in severe hypercalcemia) |
| Cardiovascular | Shortened QT interval, hypertension |
Pathology (Robbins):
- Adenomas: solitary, 0.5-5 g, tan-reddish-brown, composed of chief cells with small central nuclei; remaining glands are normal/suppressed due to feedback inhibition
- Hyperplasia: involves all four glands (though asymmetric); chief cell hyperplasia pattern
- Carcinoma: gray-white invasive mass; diagnosis requires invasion or metastasis (cytology alone is unreliable); CDC73 gene mutation in ~30%
Lab findings:
- High serum Ca²+, low serum PO₄ (phosphaturia)
- High PTH (inappropriately elevated for Ca level)
- Hypercalciuria (24-hour urine)
- Elevated alkaline phosphatase (if bone involvement)
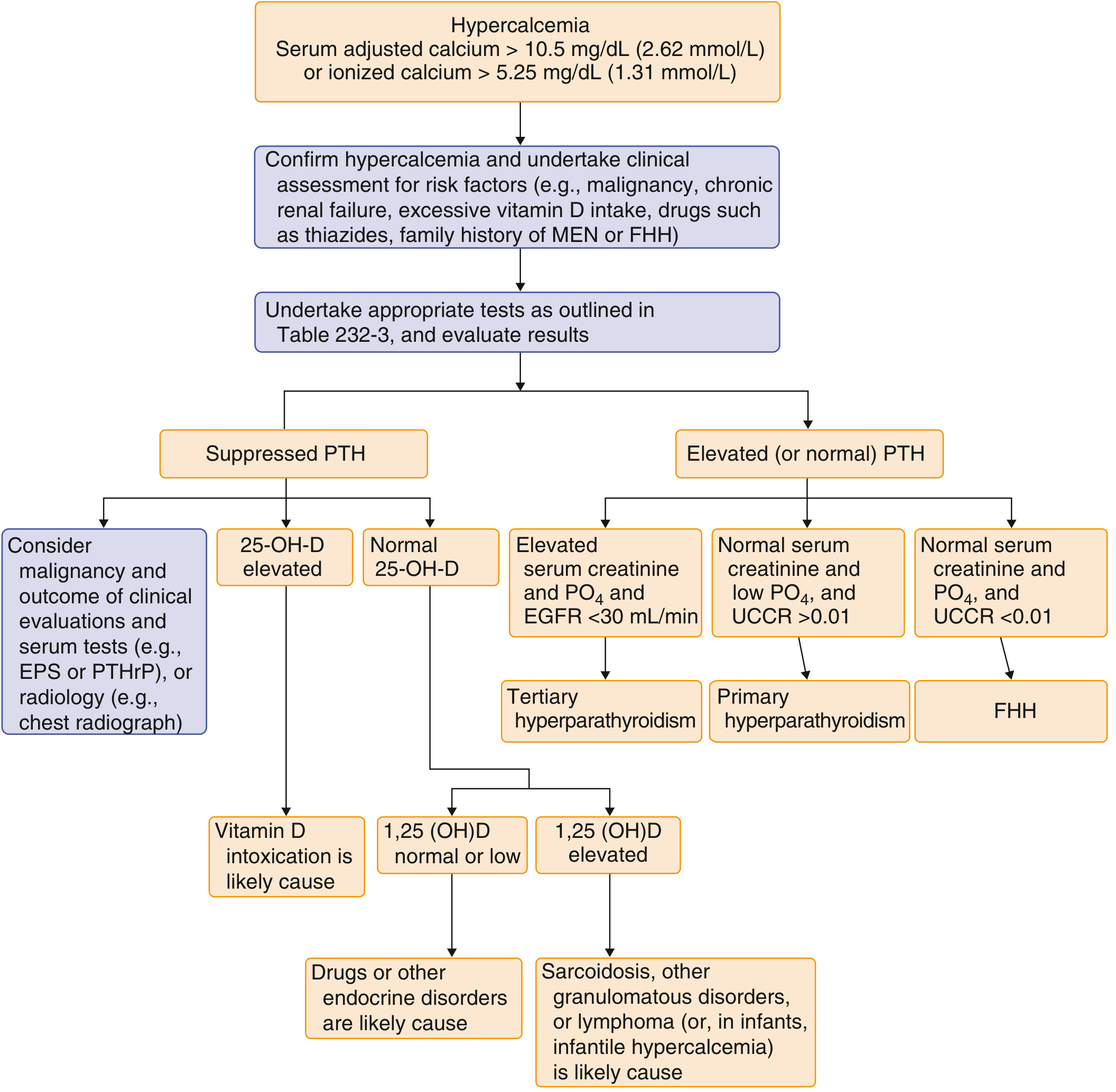
Diagnosis algorithm:
Surgery guidelines (indications for parathyroidectomy):
- Any complication (nephrolithiasis, osteitis fibrosa cystica)
- Episode of life-threatening hypercalcemia
- Serum Ca > 1 mg/dL above upper limit of normal
- Marked hypercalciuria (>400 mg/24h men, >300 mg/24h women) + stone risk
- Creatinine clearance < 60 mL/min
- BMD T-score below -2.5 or vertebral fracture
- Age < 50 years
Medical treatment:
- Cinacalcet (calcimimetic - activates CaSR, reduces PTH) for patients who cannot have surgery or have recurrence
B. Secondary Hyperparathyroidism
Definition: Reactive PTH excess due to persistent hypocalcemia driving parathyroid hyperplasia.
Most common causes:
- Chronic kidney disease (CKD) - reduced calcitriol production + hyperphosphatemia → low Ca
- Vitamin D deficiency
- Malabsorption syndromes
Labs: Low or normal Ca, elevated PTH, elevated phosphate (in CKD)
Treatment: Correct the cause; calcitriol (0.5-1.0 μg/day) to suppress PTH; avoid if phosphorus > 5.5 mg/dL.
C. Tertiary Hyperparathyroidism
Definition: In chronic secondary hyperparathyroidism (usually CKD), parathyroid activity becomes autonomous and independent of calcium levels, producing hypercalcemia. Essentially an adenoma developing within the hyperplastic glands.
Treatment: Parathyroidectomy.
5. Hypoparathyroidism
Definition: Deficiency or inactivity of PTH, resulting in hypocalcemia and hyperphosphatemia.
Causes:
| Category | Examples |
|---|---|
| Surgical (most common acquired) | Inadvertent removal during thyroidectomy, radical neck dissection, or treatment of primary hyperparathyroidism |
| Autoimmune | Isolated autoimmune; APS-1 (autoimmune polyglandular syndrome type 1 - AIRE gene mutations): candidiasis + hypoparathyroidism + adrenal insufficiency |
| Genetic | DiGeorge syndrome (3rd/4th pharyngeal pouch abnormality - chromosome 22q11 deletion), familial isolated hypoparathyroidism (FIH), gain-of-function CaSR mutations |
| Infiltrative | Hemochromatosis, amyloidosis, sarcoidosis, Wilson disease, thalassemia |
| Functional | Hypomagnesemia (impairs PTH release AND causes end-organ resistance) |
Labs:
- Low serum Ca, high serum PO₄ (because PTH normally promotes phosphaturia)
- Low or inappropriately normal PTH
Clinical features:
- Tetany - hallmark; carpopedal spasm, laryngospasm, generalized seizures
- Circumoral and distal extremity paresthesias/numbness
- Chvostek sign and Trousseau sign (see Section 7)
- Mental status changes: emotional instability, anxiety, depression, confusion, hallucinations, psychosis
- Basal ganglia calcifications (paradoxical - due to elevated phosphate → calcium phosphate deposits)
- Cataracts (lens calcification)
- QT prolongation on ECG
- Dental abnormalities (if hypocalcemia present during development): enamel defects, delayed eruption, hypoplasia
Treatment:
- Calcitriol (active vitamin D) + oral calcium supplements
- IV calcium gluconate for acute symptomatic hypocalcemia (10 mL of 10% calcium gluconate over 5 minutes; can repeat)
- Hypomagnesemia must be corrected first (otherwise PTH remains suppressed/ineffective)
6. Pseudohypoparathyroidism
Definition: End-organ resistance to PTH. PTH is secreted normally (or in excess), but target tissues fail to respond.
Labs: Low Ca, high PO₄, elevated PTH (distinguishes it from true hypoparathyroidism)
Mechanism: Defects in the G-protein coupled signaling pathway shared by PTH, TSH, FSH/LH receptors. PTH infusion fails to produce the expected rise in urinary cAMP and phosphorus excretion.
Type Ia (Albright Hereditary Osteodystrophy - AHO):
- Short stature, round facies, obesity, brachyactyly (shortened 4th/5th metacarpals)
- Mental retardation
- Also resistant to TSH (mild hypothyroidism) and gonadotropins (hypogonadism in females)
- Caused by loss-of-function mutation in GNAS1 (Gsα subunit)
7. Trousseau Sign
What it is: A classic bedside sign of latent tetany due to hypocalcemia.
How to elicit it:
- Inflate a sphygmomanometer (blood pressure cuff) around the forearm to 20 mmHg above the patient's systolic blood pressure for 3 minutes
- Watch for carpal spasm of the outstretched hand (main d'accoucheur - "obstetrician's hand"): flexion at the wrist and MCP joints, extension at the IP joints, adduction of the thumb
Mechanism: Occlusion of the brachial artery produces ischemia and local hypoxia, which lower the threshold for nerve fiber firing in already-excitable (hypocalcemic) nerves. This unmasks latent tetany.
Interpretation:
- Positive Trousseau sign = strongly suggests hypocalcemia (more specific than Chvostek's sign)
- Chvostek sign (tapping the facial nerve near the ear to produce ipsilateral facial muscle twitching) may be positive in up to 10% of normal individuals - less specific
- Trousseau sign is considered more specific for clinically significant hypocalcemia
Conditions causing a positive Trousseau sign:
- Hypoparathyroidism (post-surgical, autoimmune, genetic)
- Vitamin D deficiency / rickets
- Chronic kidney disease (secondary hyperparathyroidism with low Ca)
- Acute pancreatitis (fat saponification consumes Ca)
- Hypomagnesemia
- After massive blood transfusion (citrate chelates Ca)
- Pseudohypoparathyroidism
- Respiratory alkalosis (hyperventilation reduces ionized Ca fraction without changing total Ca)
8. Hypercalcemia Summary
Definition: Total Ca > 10.5 mg/dL or ionized Ca > 5.25 mg/dL (1.31 mmol/L)
Two most common causes:
- Primary hyperparathyroidism (most common in outpatients/asymptomatic)
- Malignancy (most common in hospitalized patients - via PTHrP from tumor, or osteolytic mets)
Malignancy-associated hypercalcemia:
- PTHrP (parathyroid hormone-related peptide) secretion by squamous cell carcinomas, renal cell carcinoma, breast cancer, etc. - mimics PTH action
- Osteolytic metastases (breast, lung)
- 1,25(OH)₂D excess in lymphoma and granulomatous disease (sarcoidosis)
Other causes: Vitamin D intoxication, thiazide diuretics, milk-alkali syndrome, sarcoidosis, thyrotoxicosis, familial hypocalciuric hypercalcemia (FHH), immobilization, Paget disease, adrenal insufficiency.
Acute management of severe hypercalcemia:
- IV saline hydration (5-10 L of 0.9% NaCl over 24-48 hours; lowers Ca by 1-3 mg/dL)
- Loop diuretic (furosemide) - only to manage fluid overload, not as primary calciuretic
- Bisphosphonates (zoledronic acid 4 mg IV, or pamidronate 15-90 mg IV) - drug of choice for malignancy-associated hypercalcemia; do not use for primary/tertiary hyperparathyroidism
- Glucocorticoids (hydrocortisone 120 mg/day) - effective when 1,25(OH)₂D is the mediator (granulomatous disease, lymphoma)
- Dialysis - for refractory cases or renal failure
9. Hypocalcemia Diagnostic Algorithm
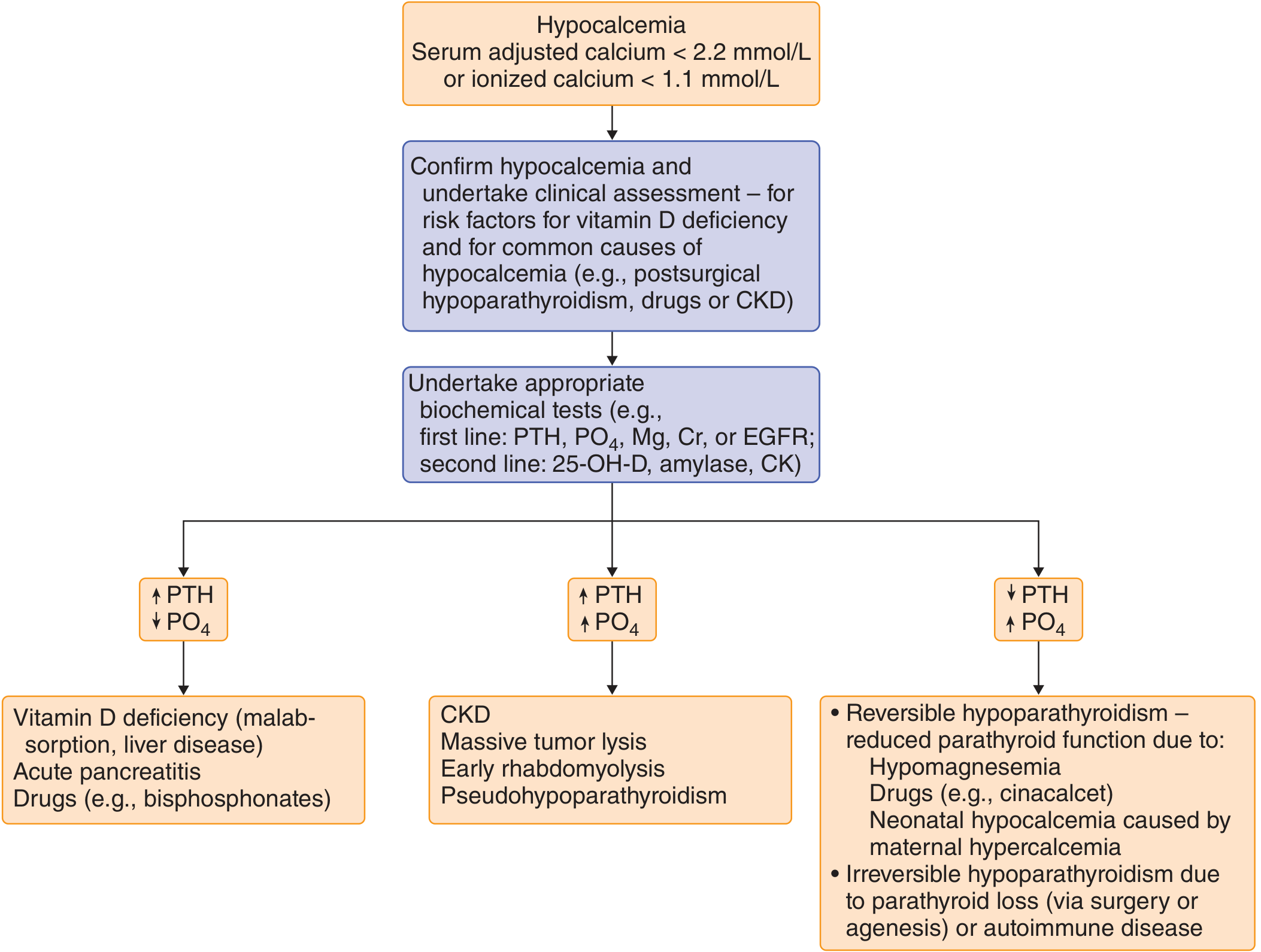
Key diagnostic pattern using PTH and phosphate:
| PTH | PO₄ | Diagnosis |
|---|---|---|
| Low or normal | High | Hypoparathyroidism (PTH absent so phosphaturia lost) |
| High | Low | Vitamin D deficiency, malabsorption, pancreatitis, bisphosphonates |
| High | High | CKD, massive tumor lysis, rhabdomyolysis, pseudohypoparathyroidism |
Quick Summary Table: Parathyroid Disorders
| Disorder | PTH | Ca | PO₄ | Key Feature |
|---|---|---|---|---|
| Primary hyperparathyroidism | High | High | Low | Stones, bones, groans; adenoma |
| Secondary hyperparathyroidism | High | Low/normal | High (in CKD) | Reactive to hypocalcemia; 4-gland hyperplasia |
| Tertiary hyperparathyroidism | High (autonomous) | High | Variable | Post-CKD autonomous |
| Hypoparathyroidism | Low | Low | High | Post-surgical most common; tetany |
| Pseudohypoparathyroidism | High | Low | High | End-organ resistance; AHO features |
| Familial hypocalciuric hypercalcemia | Normal/slightly high | High | Normal | CaSR loss-of-function; urine Ca LOW; benign |
Sources: Goldman-Cecil Medicine, Ch. 227 | Robbins & Cotran Pathologic Basis of Disease, Ch. 24 | Medical Physiology (Boron & Boulpaep), Ch. 52 | Frameworks for Internal Medicine, Ch. 9 | National Kidney Foundation Primer on Kidney Diseases, Ch. 2 | Robbins & Kumar Basic Pathology, Ch. 7
This is a shared conversation. Sign in to Orris to start your own chat.