Primary adrenal insufficiency
Reading File
Reading File
Finding Sources
Searching PubMed
"primary adrenal insufficiency" AND "Addison disease"
Running Command
python3 -c " import pdfplumber pdf_path = '/home/daytona/workspace/attachments/e…
Finding Sources
Running Command
python3 -c " import pdfplumber pdf_path = '/home/daytona/workspace/attachments/e…
Reading File
Running Command
python3 -c " from pypdf import PdfReader pdf_path = '/home/daytona/workspace/att…
Reading File
Running Command
python3 -c " from pypdf import PdfReader pdf_path = '/home/daytona/workspace/att…
Reading File
Running Command
python3 -c " from pypdf import PdfReader pdf_path = '/home/daytona/workspace/att…
Reading File
Loading Image
Loading Image
I now have all the content needed. Here is a comprehensive summary of Primary Adrenal Insufficiency synthesized from Nelson Textbook of Pediatrics 2024 (Chapter 615) and Goldman-Cecil Medicine.
Primary Adrenal Insufficiency (Addison Disease)
Definition
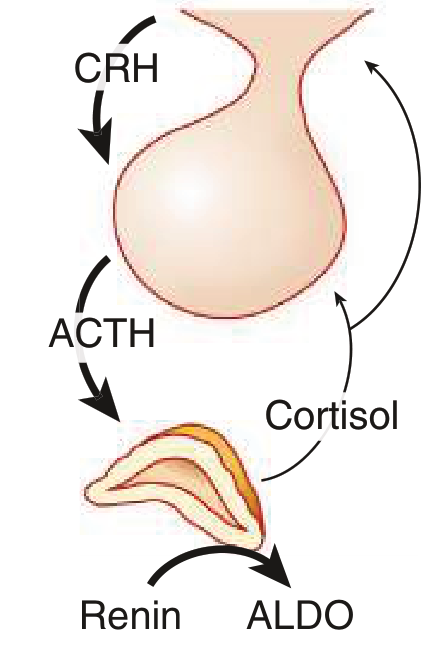
Primary adrenal insufficiency (PAI) results from congenital or acquired destruction/dysfunction of the adrenal cortex itself, causing deficiency of cortisol and often aldosterone (and DHEA). This distinguishes it from secondary (pituitary ACTH deficiency) and tertiary (hypothalamic CRH deficiency) forms.
Normal HPA axis:
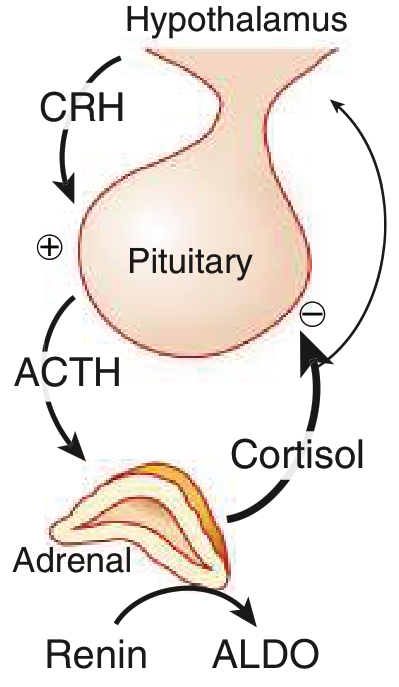
In PAI, adrenal destruction → ↓cortisol → loss of negative feedback → ↑↑ CRH + ACTH → hyperpigmentation. Aldosterone deficiency → ↑ renin.
Etiology
In Children — Genetic causes predominate (>65% of childhood PAI)
| Category | Examples |
|---|---|
| Inborn errors of steroidogenesis (CAH) | 21-hydroxylase def. (CYP21A2), 11β-hydroxylase def. (CYP11B1), 3β-HSD def., lipoid adrenal hyperplasia (StAR) — most common cause of PAI in infancy (~59%) |
| ACTH unresponsiveness | Familial glucocorticoid deficiency type 1 (MC2R), type 2 (MRAP); Triple A/Allgrove syndrome (AAAS) |
| Adrenal hypoplasia congenita | X-linked (NR0B1/DAX1) — common in males; NR5A1 (SF-1) deficiency |
| Peroxisomal defects / lipid metabolism | X-linked adrenoleukodystrophy (ABCD1/Xq28) — most common in preadolescent boys; Zellweger syndrome, neonatal ALD |
| Mitochondrial / redox defects | NNT, TXNRD2 deficiency |
| Syndromic / growth restriction | IMAGe syndrome (CDKN1C), MIRAGE syndrome (SAMD9), Pallister-Hall (GLI3) |
In Adults — Acquired causes predominate
| Cause | Notes |
|---|---|
| Autoimmune (Addison disease) | ~80% in developed countries; anti-CYP21A2 antibodies; isolated or as APS-1 (AIRE mutation: + hypoparathyroidism + mucocutaneous candidiasis) or APS-2 (+ autoimmune thyroid disease or T1DM) |
| Infections | TB (historically), meningococcemia (Waterhouse-Friderichsen syndrome), histoplasmosis, cryptococcosis, CMV in AIDS |
| Infiltration / metastases | Lung, breast, kidney, colon carcinoma; lymphoma; amyloidosis; hemochromatosis |
| Adrenal hemorrhage | Neonatal (breech delivery); anticoagulated adults; antiphospholipid syndrome |
| Drugs | Ketoconazole, mitotane, etomidate, abiraterone, immune checkpoint inhibitors (nivolumab, pembrolizumab) |
| Adrenoleukodystrophy | Present in childhood/adolescence; ↑ plasma C26:0 very-long-chain fatty acids |
Pathophysiology
| Deficiency | Consequence |
|---|---|
| Cortisol ↓ | ↓Cardiac output + vascular tone; catecholamine resistance → hypotension, shock; ↓gluconeogenesis → hypoglycemia; ↓free water excretion → hyponatremia; loss of negative feedback → ↑↑ACTH → hyperpigmentation |
| Aldosterone ↓ | ↓Na⁺ reabsorption → hypovolemia, hyponatremia, salt craving; ↓K⁺ excretion → hyperkalemia |
| ↑↑ ACTH / POMC peptides | Skin hyperpigmentation (via γ-MSH); prominent in creases, buccal mucosa, scars, nipples |
Clinical Manifestations
Table: Signs, Symptoms, and Prevalence (Nelson 2024, Table 615.6)
| Feature | Mechanism | Prevalence |
|---|---|---|
| Fatigue, anorexia, weight loss | GC deficiency | ~90% |
| Nausea, vomiting | GC + MC deficiency | ~90% |
| Hyperpigmentation (primary only) | Excess ACTH/POMC | ~70% |
| Hypotension / orthostatic hypotension | MC + GC deficiency | 70–100% |
| Hyponatremia | MC + GC deficiency | ~90% |
| Hyperkalemia (primary only) | MC deficiency | ~50% |
| Hypoglycemia | GC deficiency | ~30% |
| Salt craving (primary only) | MC deficiency | ~20% |
| High ACTH | GC deficiency | 100% |
| High plasma renin activity | MC deficiency | 100% |
Age-specific features:
- Infants: Hyperkalemia, hyponatremia, hypoglycemia dominate; hyperpigmentation absent (takes weeks/months); decompensation can occur within days
- Older children/adults: Insidious onset of weakness, malaise, weight loss, orthostatic hypotension; often misdiagnosed as chronic fatigue, depression, or anorexia nervosa; acute adrenal crisis can be precipitated by minor illness
Adrenal Crisis (acute):
Orthostatic hypotension → circulatory collapse, abdominal pain, fever, confusion. Most often caused by hemorrhage, metastasis, or acute infection. Life-threatening if untreated.
Diagnosis
Diagnostic algorithm (Nelson 2024, Fig. 615.2):
Primary Adrenal Insufficiency suspected
│
├─ Measure 17-OH-progesterone
│ (+) >1000 ng/dL → CAH (21-hydroxylase deficiency)
│ (−) ↓
│
├─ 21-OH Antibody (if >6 months)
│ (+) → Autoimmune AI (consider APS-1/APS-2)
│ (−) ↓
│
├─ VLCFA (males) → Adrenoleukodystrophy
│ (+) → ALD
│ (−) ↓
│
└─ CT Adrenals → Infiltrative disease, hemorrhage, infection, malignancy
If negative → Genetic syndromes (rare CAH, AHC, etc.)
Key lab tests:
| Test | Interpretation |
|---|---|
| Morning serum cortisol | <3 μg/dL diagnostic; >18 μg/dL excludes; 3–18 μg/dL indeterminate |
| ACTH stimulation test (gold standard) | 250 μg cosyntropin IV; cortisol <18 μg/dL at 30–60 min = PAI |
| Low-dose ACTH test | 1 μg/1.73 m² — more sensitive for secondary AI |
| Plasma ACTH | High in primary; low/normal in secondary |
| Plasma renin activity | Elevated in primary (aldosterone deficiency) |
| Electrolytes | Hyponatremia, hyperkalemia, hypoglycemia |
| Anti-CYP21A2 antibodies | Autoimmune Addison; small adrenals on imaging |
| VLCFA | Adrenoleukodystrophy (screen all males with PAI) |
| CT/MRI adrenals | Large +/− calcified (TB, fungal, hemorrhage); small (autoimmune) |
Treatment
Acute Adrenal Crisis
- Draw blood for cortisol, ACTH, aldosterone, renin, electrolytes, glucose before treatment if possible
- IV fluids: 5% dextrose in 0.9% NaCl — corrects hypoglycemia, hypovolemia, hyponatremia. Avoid hypotonic fluids.
- Hydrocortisone sodium succinate IV bolus, then q6h × 24 hours:
- Infants: 10 mg bolus
- Toddlers: 25 mg
- Older children: 50 mg
- Adolescents: 100 mg
- Treat hyperkalemia if severe: IV calcium, bicarbonate, glucose/insulin, Kayexalate
Chronic Replacement
| Drug | Dose | Notes |
|---|---|---|
| Hydrocortisone (glucocorticoid) | 10–15 mg/m²/day PO ÷ 3 doses | Monitor with ACTH levels (morning ACTH 1–4× ULN acceptable) |
| Fludrocortisone (mineralocorticoid) | 0.05–0.2 mg/day PO | Monitor with plasma renin activity; if primary AI only |
| DHEA | Adults: controversial | May improve fatigue/energy, especially in women |
Stress dosing:
- Minor illness / fever: 2–3× usual hydrocortisone dose
- Major surgery / GA: High-dose IV hydrocortisone (as for acute crisis)
⚠️ Caution: If concurrent hypothyroidism, treat adrenal insufficiency first — thyroxine accelerates cortisol clearance and can precipitate crisis if GC replacement is inadequate.
⚠️ Rifampicin, phenytoin, and phenobarbital induce hepatic steroid metabolism and reduce effectiveness of corticosteroid replacement — higher doses may be needed.
Key Distinguishing Features: Primary vs. Secondary AI
| Feature | Primary | Secondary |
|---|---|---|
| Cause | Adrenal gland destruction | Pituitary/hypothalamic ACTH or CRH ↓ |
| Cortisol | ↓ | ↓ |
| Aldosterone | ↓ | Normal |
| ACTH | ↑↑ | ↓ or inappropriately normal |
| Hyperpigmentation | Yes | No |
| Hyperkalemia | Yes | No |
| Hyponatremia | Yes | Yes (mild) |
| Adrenal size on imaging | Small (autoimmune) or large (infiltration) | Normal or small |
Recent Evidence
Two 2024–2025 meta-analyses are notable:
- Increased pregnancy/fetal complications in PAI (PMID: 39277840) — systematic review confirming adverse obstetric outcomes; relevant for management in women of reproductive age.
- Increased mortality in PAI (PMID: 40966723) — 2025 meta-analysis confirming excess mortality, reinforcing the need for adequate replacement and sick-day rules.
Sources: Nelson Textbook of Pediatrics 2024, Chapter 615 (Perrin C. White); Goldman-Cecil Medicine, Chapter 208; provided Part 24 PDF attachment.
From Nelson only
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.