Difference between undescended and ectopic testis
Reading File
Finding Sources
Searching the Web
undescended testis vs ectopic testis difference anatomy
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a thorough, well-illustrated answer. Here is the complete comparison:
Undescended Testis vs. Ectopic Testis
Both conditions result in an empty scrotum on the affected side, but they differ fundamentally in the mechanism and site of maldescent.
Core Definitions
| Feature | Undescended Testis (Cryptorchidism) | Ectopic Testis |
|---|---|---|
| Definition | Testis arrested at any point along its normal path of descent | Testis that has deviated from its normal path of descent |
| Path taken | Follows the normal retroperitoneum → inguinal canal → scrotum route, but stops early | Passes through the external ring normally, then migrates to an abnormal site |
| Scrotum | Underdeveloped/hypoplastic on affected side | Also empty, but scrotum may be better developed |
| Testicular development | Always smaller and less developed than the contralateral testis | Usually well developed |
- S Das, A Manual on Clinical Surgery, 13th Ed.
- Schwartz's Principles of Surgery, 11th Ed.
Normal Testicular Descent (Background)
The testis develops on the urogenital ridge (5th-6th week of embryonic life) and descends through the inguinal canal into the scrotum during the 7th-8th months of fetal life. At birth, ~95% of infants have normally descended testes.
Undescended Testis - Sites of Arrest
The testis is arrested within its normal path:
- Retroperitoneum / abdominal cavity
- Internal inguinal ring
- Inguinal canal (most common palpable site)
- External inguinal ring / upper scrotum
A testis in the inguinal canal is most likely undescended. It may be associated with an inguinal/interstitial hernia.
Ectopic Testis - Sites
The ectopic testis has passed through the external ring and come to rest outside its normal path. Sites correspond to the accessory tails of the gubernaculum:
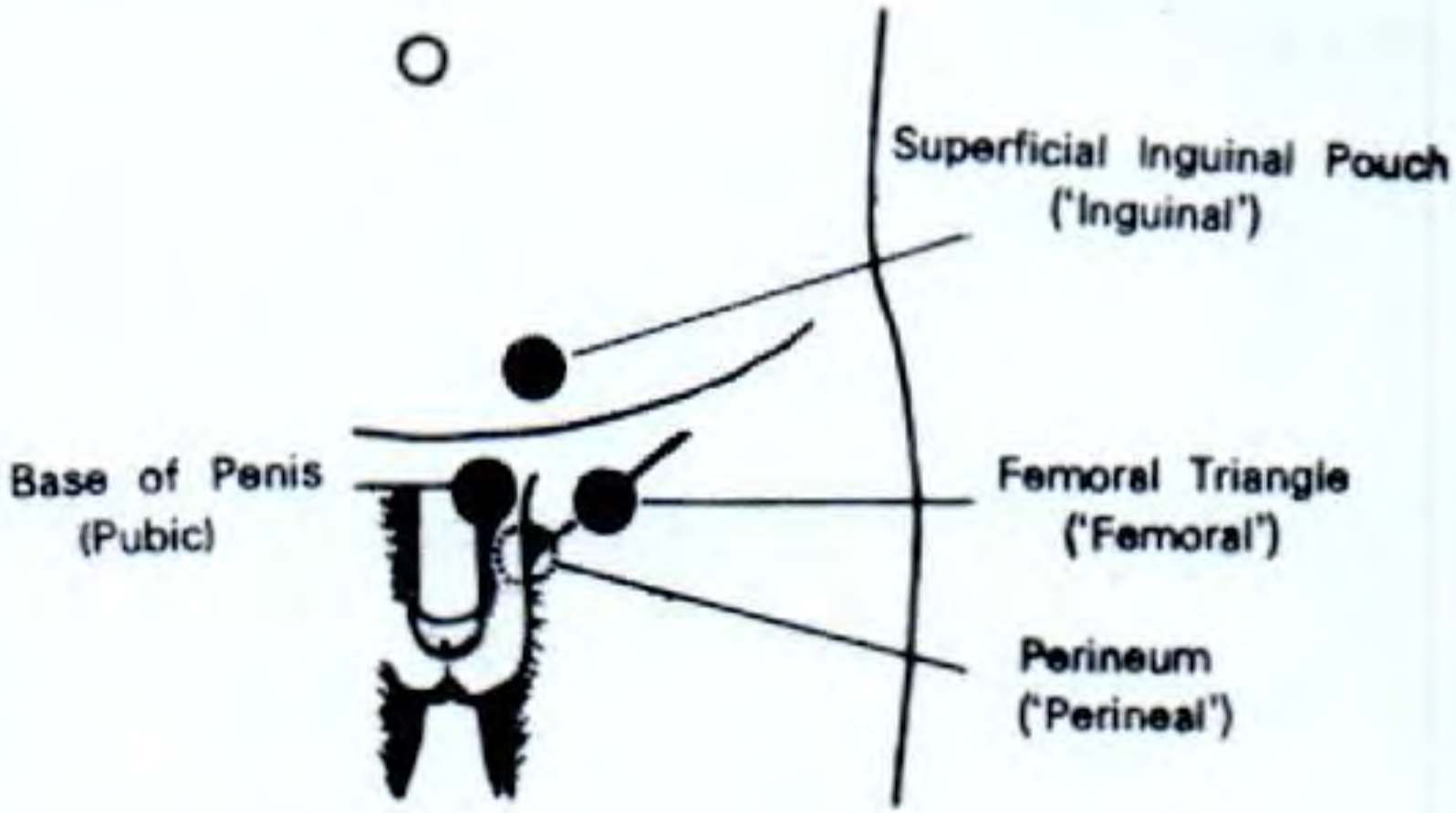
| Type | Location |
|---|---|
| Inguinal (most common) | Superficial inguinal pouch - just above and lateral to the superficial inguinal ring, superficial to the external oblique aponeurosis |
| Pubic | Root/base of the penis |
| Perineal | Perineum |
| Femoral | Upper medial part of femoral triangle (near saphenous opening) |
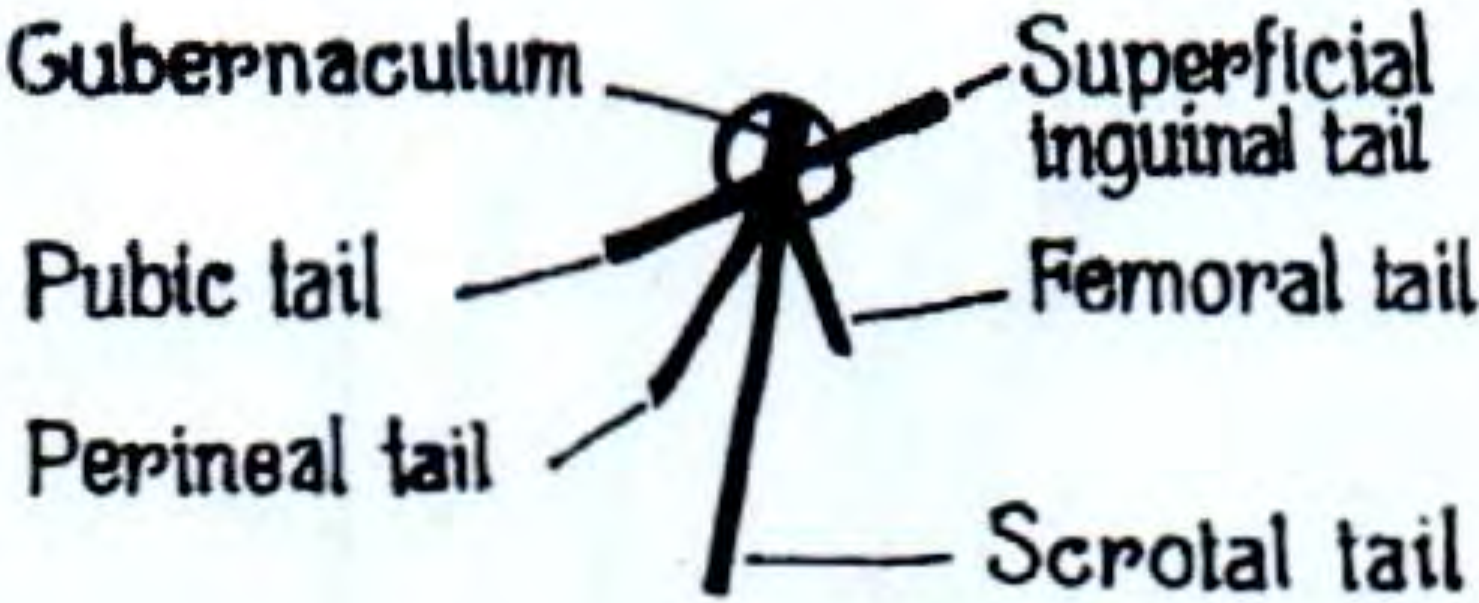
Mechanism: The Gubernaculum Theory (Lockwood)
The gubernaculum testis has five tails:
- Scrotal tail - the main one; normally the strongest
- Pubic tail - attached to the pubic tubercle
- Perineal tail - attached to the perineum
- Superficial inguinal tail - attached to the front of the inguinal canal
- Femoral tail - attached to the saphenous opening
Normally, the scrotal tail dominates and guides the testis into the scrotum. The other four tails regress.
- In undescended testis: the scrotal tail is weak and the testis simply stops partway along the normal route.
- In ectopic testis: the scrotal tail ruptures and one of the accessory tails becomes dominant, pulling the testis to that aberrant site.
Key Clinical Differences
| Feature | Undescended | Ectopic |
|---|---|---|
| Testicular size | Small, atrophic (especially after puberty) | Usually normal size |
| Location on exam | Within the inguinal canal or abdomen | Superficial to the external oblique aponeurosis ("rising test" positive - rises as you try to push it toward the abdomen) |
| Associated hernia | Common (processus vaginalis remains open) | Less common |
| Risk of torsion | Higher (undescended testis commonly undergoes torsion) | Lower |
| Risk of malignancy | Significantly elevated | Also elevated (same congenital basis) |
| Fertility impact | Reduced spermatogenesis (temperature-dependent) | Less impaired because the testis is usually well developed |
The "Rising Test"
To distinguish ectopic from undescended testis on clinical examination: attempt to push the swelling toward the abdominal cavity. An ectopic testis (which lies superficial to the external oblique) will rise (move away from the examiner's hand superficially), while an undescended testis within the inguinal canal will move normally with the canal.
Complications (Shared, but differ in degree)
- Infertility - both cause reduced spermatogenesis; worse with undescended testis due to temperature
- Malignancy - risk elevated in both; research suggests they may share a common congenital anomaly basis (PubMed PMID 10688032)
- Torsion - especially with undescended testis; mimics strangulated hernia
- Psychological impact of empty scrotum
Treatment
Both are treated with orchidopexy (surgical placement into the scrotum), ideally by 1 year of age to preserve fertility potential and allow earlier malignancy detection. Hormonal therapy (hCG) may be tried first in bilateral cases, but failure after 1 month is an indication for surgery.
Summary in one sentence: An undescended testis is arrested along the normal path, is always underdeveloped, and sits within the inguinal canal or abdomen; an ectopic testis has completed the normal path but deviated to an abnormal site (most commonly the superficial inguinal pouch), and is typically well developed.
Sources: S Das, A Manual on Clinical Surgery 13th Ed. | Schwartz's Principles of Surgery 11th Ed. | Bailey & Love's Short Practice of Surgery 28th Ed.
In tabular column
Here is the complete comparison in a single tabular format:
| Feature | Undescended Testis (Cryptorchidism) | Ectopic Testis |
|---|---|---|
| Definition | Testis arrested at any point along its normal path of descent | Testis that has deviated from its normal path after passing through the external ring |
| Path of descent | Follows the normal route but stops prematurely | Completes the inguinal canal, then migrates to an abnormal site |
| Mechanism | Scrotal tail of gubernaculum is weak - testis stalls | Scrotal tail ruptures; an accessory gubernacular tail becomes dominant |
| Scrotum | Underdeveloped / hypoplastic on affected side | Empty but may be better developed |
| Testicular size & development | Always smaller and less developed than the opposite side | Usually well developed and normal sized |
| Common sites | Abdomen, internal ring, inguinal canal, external ring / upper scrotum | Superficial inguinal pouch (most common), base of penis (pubic), perineum, femoral triangle |
| Relation to external oblique | Deep to the external oblique (within canal) | Superficial to the external oblique aponeurosis |
| Rising test | Negative - moves with the inguinal canal | Positive - rises superficially away from the examiner |
| Associated inguinal hernia | Common (patent processus vaginalis) | Less common |
| Risk of torsion | High | Lower |
| Risk of malignancy | Significantly elevated | Also elevated (shared congenital basis) |
| Fertility | Reduced spermatogenesis due to elevated temperature; worse bilaterally | Less impaired (testis is usually well developed) |
| Histological changes | Progressive from 1-2 years of age onwards | Less severe changes |
| Tendency to atrophy | Atrophies as puberty approaches | Less prone to atrophy |
| Treatment | Orchidopexy - ideally by 1 year of age; hCG trial in bilateral cases | Orchidopexy - same timing |
| Orchidopexy difficulty | Variable - abdominal testes require laparoscopy | Usually easier - testis is well developed with adequate cord length |
Sources: S Das, A Manual on Clinical Surgery 13th Ed. | Schwartz's Principles of Surgery 11th Ed. | Bailey & Love's Short Practice of Surgery 28th Ed.
Aswer above in tabular column
Here is the full first response converted into a tabular format:
Undescended Testis vs Ectopic Testis - Complete Comparison
Core Definitions & Pathology
| Feature | Undescended Testis | Ectopic Testis |
|---|---|---|
| Definition | Arrested along its normal path of descent | Deviated from its normal path of descent |
| Path | Normal route, stops prematurely | Passes through external ring normally, then migrates abnormally |
| Scrotum | Underdeveloped / hypoplastic | Empty but relatively better developed |
| Testicular development | Always smaller and less developed | Usually well developed |
Normal Descent Timeline
| Point | Detail |
|---|---|
| Origin | Urogenital ridge (5th-6th week of embryonic life) |
| Descent | Through inguinal canal in 7th-8th month of fetal life |
| At birth | ~95% of infants have normally descended testes |
| By 3 months | Testes absent from scrotum after this age are unlikely to descend spontaneously |
Sites of Arrest / Maldescent
| Undescended Testis (within normal path) | Ectopic Testis (outside normal path) |
|---|---|
| Retroperitoneum / abdomen | Superficial inguinal pouch - most common |
| Internal inguinal ring | Base / root of penis (pubic type) |
| Inguinal canal - most common palpable site | Perineum (perineal type) |
| External ring / upper scrotum | Upper medial femoral triangle (femoral type) |
Gubernaculum Theory (Lockwood)
| Tail | Attachment | Role |
|---|---|---|
| Scrotal tail | Scrotum | Main tail; normally the strongest - guides testis into scrotum |
| Pubic tail | Pubic tubercle | Accessory; normally regresses |
| Perineal tail | Perineum | Accessory; normally regresses |
| Superficial inguinal tail | Front of inguinal canal | Accessory; normally regresses |
| Femoral tail | Saphenous opening | Accessory; normally regresses |
| Condition | Gubernaculum Mechanism |
|---|---|
| Undescended testis | Scrotal tail is weak; testis stalls along normal route |
| Ectopic testis | Scrotal tail ruptures; an accessory tail becomes dominant and pulls testis to its attachment site |
Clinical Differences
| Feature | Undescended Testis | Ectopic Testis |
|---|---|---|
| Testicular size | Small, atrophic (worsens after puberty) | Normal size |
| Relation to external oblique | Deep to it (within canal) | Superficial to external oblique aponeurosis |
| Rising test | Negative | Positive (rises superficially when pushed) |
| Associated hernia | Common (patent processus vaginalis) | Less common |
| Risk of torsion | High | Lower |
| Risk of malignancy | Significantly elevated | Also elevated |
| Fertility impact | Reduced spermatogenesis due to heat; worse bilaterally | Less impaired |
| Histological changes | Progressive from 1-2 years of age | Less severe |
Complications
| Complication | Undescended Testis | Ectopic Testis |
|---|---|---|
| Infertility | More severe | Mild to moderate |
| Malignancy | Elevated risk | Elevated risk (shared congenital basis) |
| Torsion | High risk; mimics strangulated hernia | Lower risk |
| Psychological (empty scrotum) | Present | Present |
Treatment
| Aspect | Undescended Testis | Ectopic Testis |
|---|---|---|
| Primary treatment | Orchidopexy | Orchidopexy |
| Optimal age | By 1 year of age | By 1 year of age |
| Hormonal therapy (hCG) | Trial in bilateral cases before surgery | Rarely needed |
| Surgical difficulty | Variable; abdominal testes need laparoscopy | Usually easier - testis is well developed with adequate cord length |
| Effect on fertility | Improves but never fully normal | Good prognosis |
| Effect on malignancy risk | Risk remains; scrotal position allows earlier detection | Same |
Sources: S Das, A Manual on Clinical Surgery 13th Ed. | Schwartz's Principles of Surgery 11th Ed. | Bailey & Love's Short Practice of Surgery 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.