Dermatology ops cases with diagram and treatment or proper prescription
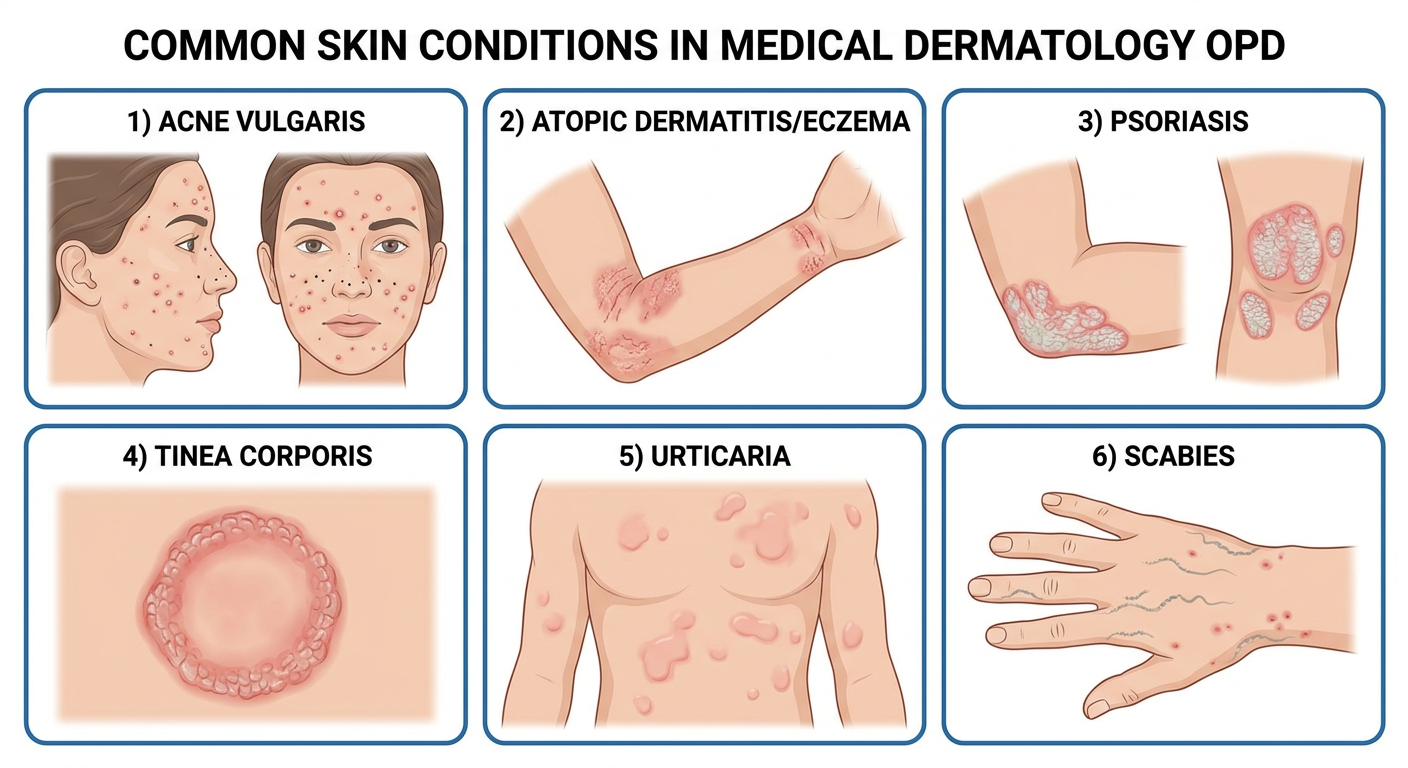
Medical dermatology OPD clinical case diagram showing 6 common skin conditions in a clean educational chart layout. Six panels arranged in a 2x3 grid, each labeled and showing: 1) Acne Vulgaris - face with comedones, papules, pustules on forehead and cheeks; 2) Atopic Dermatitis/Eczema - arm flexures with red, scaly, excoriated patches; 3) Psoriasis - thick silvery white plaques on elbow and knee; 4) Tinea Corporis - circular ring-shaped red raised lesion with central clearing on skin; 5) Urticaria - raised red hive wheals on torso skin; 6) Scabies - intensely itchy burrow lines between fingers and wrist. Each panel has the condition name as a bold label. Clean white medical illustration style with anatomical accuracy.
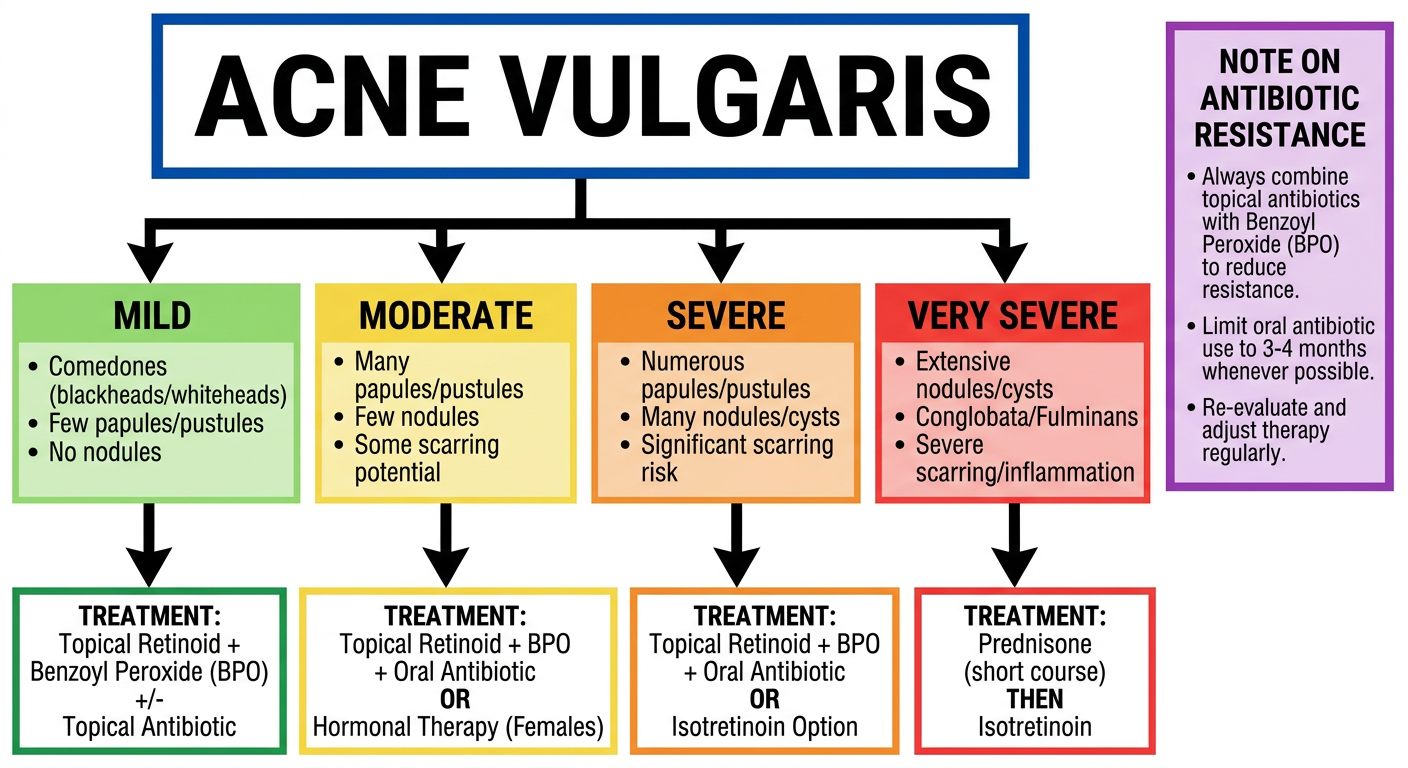
Acne Vulgaris treatment algorithm flowchart for dermatology OPD. Clean medical educational diagram showing: Top box "ACNE VULGARIS" with subclassification into 4 severity grades (Mild, Moderate, Severe, Very Severe) with bullet points for each. Below each grade, arrows point to treatment boxes. Mild: Topical retinoid + BPO +/- topical antibiotic. Moderate: Topical retinoid + BPO + oral antibiotic or hormonal therapy (females). Severe: Add isotretinoin option. Very Severe: Prednisone then isotretinoin. Side box showing note on antibiotic resistance - always combine with BPO. Color coded green/yellow/orange/red for severity. White background, bold labels, professional medical style.
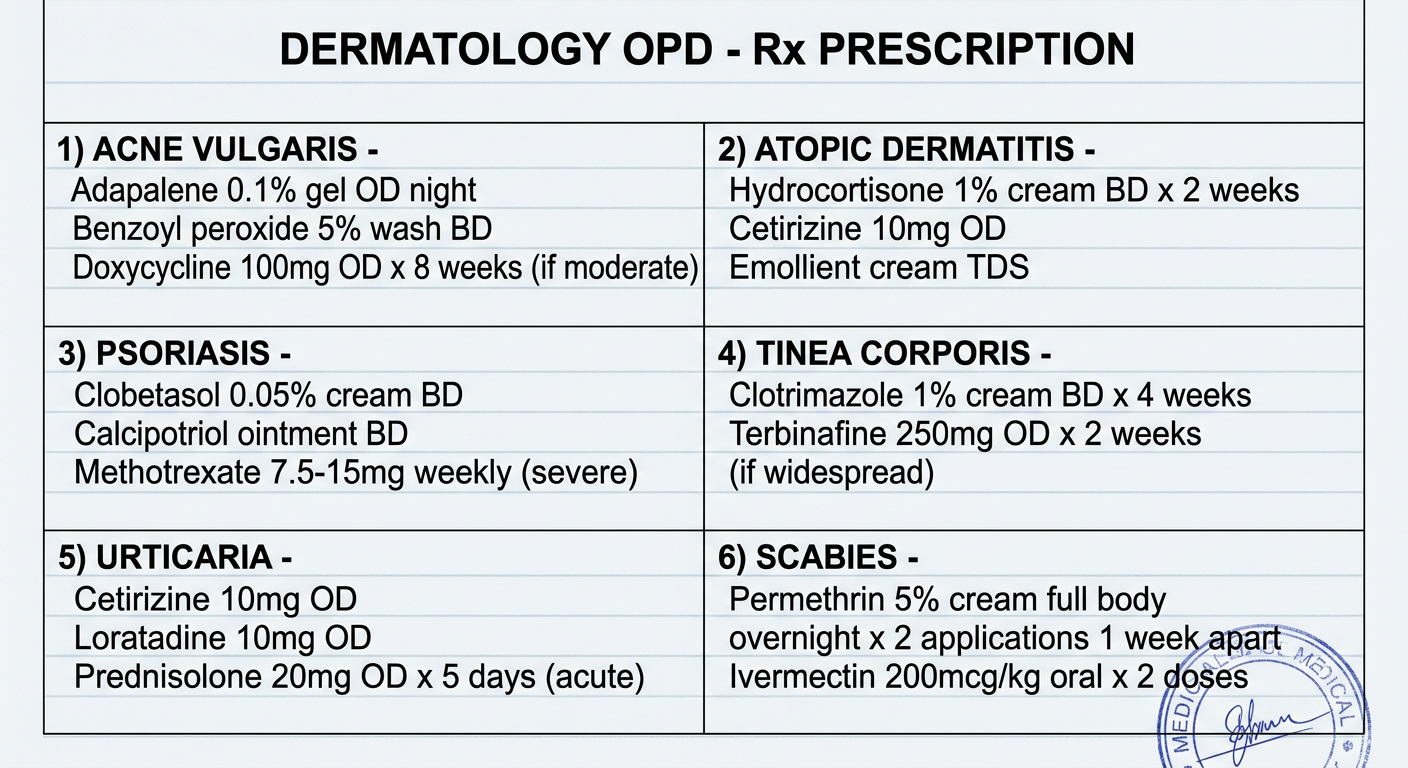
Dermatology OPD prescription pad design - a clean medical prescription template showing: Title "DERMATOLOGY OPD - Rx PRESCRIPTION" at top. Then 6 sections each with a condition header and prescription details: 1) ACNE VULGARIS - Adapalene 0.1% gel OD night, Benzoyl peroxide 5% wash BD, Doxycycline 100mg OD x 8 weeks (if moderate). 2) ATOPIC DERMATITIS - Hydrocortisone 1% cream BD x 2 weeks, Cetirizine 10mg OD, Emollient cream TDS. 3) PSORIASIS - Clobetasol 0.05% cream BD, Calcipotriol ointment BD, Methotrexate 7.5-15mg weekly (severe). 4) TINEA CORPORIS - Clotrimazole 1% cream BD x 4 weeks, Terbinafine 250mg OD x 2 weeks (if widespread). 5) URTICARIA - Cetirizine 10mg OD, Loratadine 10mg OD, Prednisolone 20mg OD x 5 days (acute). 6) SCABIES - Permethrin 5% cream full body overnight x 2 applications 1 week apart, Ivermectin 200mcg/kg oral x 2 doses. Clean white paper background with blue ruled lines, black text, medical stamp style.
🔬 Clinical Diagram - 6 Common Dermatology OPD Conditions
Treatment Algorithm Diagram
Sample Prescription Pad
CASE 1: ACNE VULGARIS
- Blackheads/whiteheads (comedones) + inflammatory papules/pustules
- Distribution: face, upper chest, back
- Grade: Mild / Moderate / Severe
Rx (by severity)
| Severity | First-Line Treatment |
|---|---|
| Mild | Topical retinoid (adapalene 0.1% gel OD night) + Benzoyl peroxide (BPO) 5% wash BD |
| Moderate | Topical retinoid + BPO + Oral doxycycline 100 mg OD x 8 weeks +/- combined OCP (females) |
| Severe | Above + Isotretinoin 0.5 mg/kg/day (after counseling) |
| Very Severe | Prednisolone 0.5 mg/kg/day x 4 weeks → then Isotretinoin (slow dose escalation) |
CASE 2: ATOPIC DERMATITIS (ECZEMA)
- Chronic relapsing pruritic dermatitis
- Flexural lichenification in older children/adults
- Xerosis (dry skin), Dennie-Morgan folds
- Pruritus, typical morphology/distribution, chronic relapsing course, personal/family atopy history
Rx
Rx
1. Emollient (Cetaphil/Vaseline) - apply liberally TDS and after bathing
2. Hydrocortisone 1% cream - apply BD to affected areas x 2 weeks (mild/face)
OR Mometasone furoate 0.1% cream - BD x 2 weeks (moderate)
3. Cetirizine 10 mg tablet - 1 OD at night x 2 weeks (antipruritic)
4. Tacrolimus 0.03% ointment - BD (if steroid-sparing needed, face/skin folds)
5. Avoid triggers: soap, wool, animal dander, sweating
CASE 3: PSORIASIS
- Chronic relapsing papulosquamous disorder
- Salmon-red plaques + silvery micaceous scale
- Auspitz sign (pinpoint bleeding on scale removal)
- Sites: extensor surfaces, scalp, nails, umbilicus, lower back
Rx
| Form | Treatment |
|---|---|
| Mild (< 10% BSA) | Clobetasol 0.05% cream/ointment BD x 4 weeks (potent topical steroid) + Calcipotriol 0.005% ointment BD |
| Scalp psoriasis | Clobetasol 0.05% shampoo + salicylic acid 2% shampoo to descale |
| Moderate-Severe | Methotrexate 7.5 mg once weekly PO, increase to 15-25 mg/week. Folate 5 mg/week supplementation |
| Biologic | Secukinumab 300 mg SC weekly x 5 weeks then monthly; or Adalimumab 80 mg then 40 mg EOW |
| Phototherapy | Narrowband UVB (NBUVB) 3x/week (308 nm excimer laser for localized plaques) |
CASE 4: TINEA CORPORIS (RINGWORM)
- Well-marginated annular plaque with raised scaly erythematous border
- Central clearing (hallmark)
- May have vesicles at advancing edge
- KOH mount: branching septate hyphae
Rx
Rx
1. Clotrimazole 1% cream - apply BD to lesion + 2 cm margin x 4 weeks
OR Terbinafine 1% cream - apply OD x 2-4 weeks (fungicidal, preferred)
OR Miconazole 2% cream - BD x 4 weeks
2. If widespread/resistant/hair involvement:
Terbinafine 250 mg tablet - 1 OD x 2-4 weeks
OR Itraconazole 200 mg BD x 1 week (pulse)
3. Advice: Keep area dry, avoid sharing towels, treat contacts
4. Tinea cruris: same regimen; add plain talc powder to groin area
5. Tinea unguium (nail): Itraconazole 200 mg BD x 1 week/month x 3 pulses
CASE 5: URTICARIA (HIVES)
- Transient erythematous or skin-colored wheals (edema of superficial dermis)
- Each wheal resolves within 24 hours leaving no mark
- Angioedema may accompany (deeper dermis/subcutis)
- Acute urticaria: < 6 weeks; Chronic: > 6 weeks
Rx
Rx - Acute Urticaria
1. Cetirizine 10 mg - 1 tab OD (non-sedating H1 antihistamine, FIRST LINE)
OR Levocetirizine 5 mg - 1 tab OD
OR Loratadine 10 mg - 1 tab OD
2. If inadequate control: INCREASE DOSE up to 4x (e.g. cetirizine 10 mg QDS)
OR add Ranitidine 150 mg BD (H2 blocker) + above
3. Severe/anaphylaxis:
Prednisolone 40 mg OD x 5 days (short course)
Epinephrine 0.3 mg IM (if angioedema with laryngeal involvement)
Chronic Urticaria:
4. Omalizumab (anti-IgE) 300 mg SC every 4 weeks (if refractory to antihistamines)
5. Identify and remove triggers: foods, NSAIDs, infections, autoimmune workup
CASE 6: SCABIES
- Nocturnal pruritus (hallmark)
- Burrows (pathognomonic) - tiny S-shaped greyish lines at web spaces, wrists
- Papules, vesicles, excoriations
- Secondary eczematization/impetiginization common
- Causative organism: Sarcoptes scabiei var. hominis
Rx
Rx
1. Permethrin 5% cream (DRUG OF CHOICE)
- Apply to entire body (neck to toes) including under nails and umbilicus
- Leave on 8-14 hours, then wash off
- REPEAT after 1 week (2 applications total)
2. Ivermectin 200 mcg/kg oral (if permethrin fails or compliance issue)
- Give 2 doses, 7-14 days apart
- NOT for children < 15 kg or pregnant women
3. For residual pruritus (post-scabetic itch):
Cetirizine 10 mg OD + Clobetasone butyrate 0.05% cream BD (mild steroid)
4. Secondary infection: Mupirocin 2% ointment BD OR Cloxacillin 500 mg QDS x 7 days
INSTRUCTIONS:
- Treat ALL household contacts simultaneously
- Wash all clothing/bedding in HOT water and dry on hot cycle
- Items that cannot be washed: seal in plastic bag for 3 days
Quick Reference Summary Table
| Condition | Key Sign | First-Line Rx | Duration |
|---|---|---|---|
| Acne Vulgaris | Comedones + papules/pustules | Topical retinoid + BPO | 12+ weeks |
| Atopic Dermatitis | Pruritus + flexural eczema | Emollient + topical steroid | Chronic |
| Psoriasis | Silvery plaques, Auspitz sign | Topical steroid + calcipotriol | Chronic |
| Tinea Corporis | Ring with central clearing | Terbinafine cream OD x 4 weeks | 2-4 weeks |
| Urticaria | Transient wheals < 24 hrs | Cetirizine 10 mg OD | Acute: 5-7 days |
| Scabies | Nocturnal itch + burrows | Permethrin 5% cream x 2 | 2 weeks |
- Dermatology 2-Volume Set 5e - Treatment of Acne Vulgaris table
- Fitzpatrick's Dermatology Vol 1&2 - Tinea management
- Harrison's Principles of Internal Medicine 22E - Scabies, Dermatophytosis
- Red Book 2021 - Committee on Infectious Diseases - Scabies treatment protocols