Re exposure prophylaxis of rabies
rabies post-exposure prophylaxis
Rabies Post-Exposure Prophylaxis (PEP)
Overview
Step 1 - WHO Exposure Category & PEP Decision
| Category | Nature of Contact | PEP Action |
|---|---|---|
| I | Touching/feeding animals, licks on intact skin | None required |
| II | Nibbling of uncovered skin, minor scratches/abrasions without bleeding | Immediate vaccination + wound care |
| III | Transdermal bites/scratches, licks on broken skin, mucous membrane contamination, bat contact | Immediate vaccination + RIG + wound care |
- The biting mammal is a known rabies reservoir/vector
- The animal appears sick or behaves abnormally
- A wound or mucous membrane was contaminated by saliva
- The bite was unprovoked
- The animal was unvaccinated or cannot be traced
Step 2 - Local Wound Treatment
- Cleansing - Immediately flush and wash all wounds with soap and water under a running tap for at least 15 minutes. For puncture wounds, use a catheter for irrigation. If no soap, flush with plenty of water.
- Chemical treatment - After cleansing, apply a virucidal agent: alcohol (400-700 ml/litre), tincture or 0.01% aqueous iodine, or povidone-iodine.
- Suturing - Do NOT suture bite wounds immediately. If suturing is unavoidable, wait 24-48 hours using minimum stitches, under cover of local RIG infiltration.
- Antibiotics & anti-tetanus - Give as indicated.
Step 3 - Vaccines (Active Immunization)
Type of Vaccines
- Human diploid cell vaccine (HDCV)
- Purified chick embryo cell vaccine (PCECV)
- Vero cell (purified Vero cell rabies vaccine - PVRV)
- Primary chick embryo cells, hamster kidney cells, duck egg vaccines
Intramuscular (IM) Schedules
(i) Essen Regimen - 5-dose schedule
(ii) Zagreb (Abbreviated Multisite) Regimen - 4-dose (2-1-1) schedule
(iii) Simplified 4-dose IM schedule
Intradermal (ID) Schedule
- Inject 0.1 ml at 2 sites on Days 0, 3, 7, and 28 (Day 14 is skipped)
- 1 ID dose = 1/5 of the IM dose (0.1 ml per site)
- Requires national health authority endorsement
Step 4 - Rabies Immunoglobulin (RIG) - Passive Immunization
| Product | Dose | Origin |
|---|---|---|
| Human RIG (HRIG) | 20 IU/kg body weight | Homologous - preferred |
| Equine RIG (ERIG) / F(ab')2 | 40 IU/kg body weight | Heterologous |
- Administer only once, on Day 0 (simultaneously with the first vaccine dose), or as soon as possible after
- NOT indicated beyond Day 7 after first vaccine dose (active antibody response presumed to have begun)
- Inject as much as anatomically possible directly into and around the wound site(s); remaining dose goes IM at a site distant from the vaccine injection site
- RIG may be diluted in saline if needed to infiltrate multiple wounds
- Equine RIG is cheaper but carries a small risk of anaphylaxis (~1/45,000). No skin testing needed - it does not predict reactions. Be prepared to manage anaphylaxis.
- No skin testing before ERIG - it should be given regardless
Previously Vaccinated Individuals
- Only 2 doses IM on Days 0 and 3 are needed (or 4-site ID on a single visit)
- RIG is NOT indicated in these patients
Immunocompromised Individuals (incl. HIV/AIDS)
- Full 5-dose IM CCEEV series required (not the abbreviated schedules)
- Comprehensive wound management
- RIG must be given for Category II and III exposures
- Check rabies-virus neutralizing antibody titre 2-4 weeks after vaccination; give an additional dose if response is inadequate
Special Considerations
- No contraindications to PEP after high-risk exposure - this applies to infants, pregnant women, and anyone else
- No delay is permissible - start PEP immediately
- Local wound treatment remains effective even if started hours or days late (though immediate treatment is best)
- In developing countries, vaccination status of the animal alone should not be used as grounds to withhold PEP
Recent evidence note: A 2026 meta-analysis (PMID: 41997000) examined factors influencing rabies vaccine immunogenicity during PEP, which may update specific dosing considerations - the core WHO PEP framework above remains current.
Find the latest clinical guidelines for rabies PEP (CDC, WHO 2025-2026)
CDC rabies post-exposure prophylaxis guidelines 2025 2026 updated
WHO rabies post-exposure prophylaxis guidelines 2025 updated recommendations
rabies post-exposure prophylaxis guidelines recommendations
https://www.cdc.gov/rabies/hcp/clinical-care/post-exposure-p…
WHO position paper rabies vaccines 2024 2025 PEP schedule updated
https://www.who.int/teams/control-of-neglected-tropical-dise…
PMID: 41997000
Latest Clinical Guidelines for Rabies PEP (CDC & WHO, 2025-2026)
CDC / ACIP Guidelines (Updated July 15, 2025)
Standard PEP (Previously Unvaccinated)
| Component | Detail |
|---|---|
| 1. Wound care | Immediate thorough washing with soap and water |
| 2. HRIG | 20 IU/kg - infiltrate into wound; remaining volume IM at distant site |
| 3. Vaccine series | 4 doses IM on Days 0, 3, 7, and 14 |
Key 2025 update: The standard regimen for healthy, immunocompetent individuals in the US is now a 4-dose schedule (Days 0, 3, 7, 14) - not the older 5-dose Essen schedule. The 5th dose on Day 28 is reserved for immunocompromised patients.
Immunocompromised / Immunosuppressed Patients
- Use the 5-dose regimen: Days 0, 3, 7, 14, and 28
- HRIG is still required
- Avoid immunosuppressive agents during PEP unless essential
- After completing the series, test for rabies virus neutralizing antibody (RVNA)
- Advise patients that immune response may be inadequate
Previously Vaccinated Individuals
- No HRIG required
- Only 2 doses of vaccine IM on Days 0 and 3
- Applies to those who completed prior ACIP-recommended PrEP or PEP
HRIG - Key Rules (CDC 2025)
| Point | Guidance |
|---|---|
| Product available in US | Human Rabies Immune Globulin (HRIG) only - e.g., HyperRab, Imogam Rabies |
| Dose | 20 IU/kg - infiltrate directly into wound |
| Window | Give on Day 0; can be given up to Day 7 if missed initially |
| Max dose | Do NOT exceed recommended dose - higher dose impairs vaccine response |
| Special product | HyperRab 300 IU/ml must be diluted with D5W (dextrose 5% in water) |
| Never | Give HRIG in the same syringe or same anatomical site as vaccine |
Practical Pitfalls (CDC 2025 Guidance)
- If HRIG and vaccine were inadvertently given at the same site: re-administer vaccine at a distant site; may re-administer HRIG if total dose does not exceed 40 IU/kg
- If the PEP schedule is delayed: maintain recommended spacing for subsequent doses; delays of a few days are acceptable but lapses of weeks may have unpredictable consequences
- Mild adverse reactions: do NOT interrupt PEP; manage with ibuprofen or acetaminophen
WHO Guidelines (2018 Position Paper - Current as of 2025)
WHO Exposure Categories (Unchanged)
| Category | Contact | PEP |
|---|---|---|
| I | Touch/feed animals, licks on intact skin | None |
| II | Nibbling of uncovered skin, minor scratches without bleeding | Vaccine + wound care |
| III | Transdermal bites/scratches, mucous membrane licks, bat contact | Vaccine + RIG + wound care |
WHO-Recommended Vaccine Schedules
- Essen (5-dose): Days 0, 3, 7, 14, 28
- Zagreb (2-1-1): 2 doses Day 0 (one each deltoid), then Day 7, Day 21
- Simplified 4-dose: Days 0, 3, 7, 14 (for immunocompetent patients with quality wound care + RIG)
Key WHO update: WHO promotes intradermal (ID) administration as the preferred route in endemic settings. It is equally safe and efficacious while using 60-80% less vaccine volume and requiring only 1-2 vials for a full course vs. 4-5 vials IM.
| Schedule | Regimen |
|---|---|
| Shortened 1-week ID (current WHO recommendation) | 0.1 ml at 2 sites, Days 0, 3, and 7 only |
| Legacy 2-site ID | 0.1 ml at 2 sites on Days 0, 3, 7, 28 |
- Previously vaccinated: 1-site ID 0.1 ml on Days 0 and 3 only (no RIG)
WHO RIG Recommendations
| Product | Dose | Notes |
|---|---|---|
| Human RIG (HRIG) | 20 IU/kg | Preferred; homologous |
| Equine RIG (ERIG) / F(ab')2 | 40 IU/kg | Acceptable; cheaper; small anaphylaxis risk (~1/45,000); no skin test needed |
- Give RIG only once, Day 0 (up to Day 7 if missed)
- Infiltrate all of it directly into/around the wound; remainder IM at distant site from vaccine
CDC vs. WHO: Key Differences at a Glance
| Aspect | CDC (US, 2025) | WHO (Global, 2025) |
|---|---|---|
| Standard vaccine schedule | 4-dose IM (Days 0, 3, 7, 14) | Multiple options; 1-week 2-site ID preferred for endemic settings |
| Immunocompromised | 5-dose IM | 5-dose IM |
| ID route | Not used in US | Strongly promoted; cost-saving |
| RIG type in use | HRIG only (US) | HRIG or ERIG/F(ab')2 |
| HRIG dose | 20 IU/kg | 20 IU/kg (HRIG); 40 IU/kg (ERIG) |
| Previously vaccinated | 2 doses Days 0 & 3, no RIG | 2 doses Days 0 & 3 (IM or ID), no RIG |
| Skin test before ERIG | N/A | NOT recommended |
Latest Evidence (2026 Meta-Analysis)
- Seroconversion rate by Day 14: 98% across all vaccines - not affected by vaccine type, route (IM vs. ID), or RIG use
- All three vaccines provide equivalent protection regardless of route of administration
- Supports WHO's position that ID and IM routes are interchangeable
Tell me about the latest schedule followed in India
India rabies PEP schedule 2024 2025 NCDC APCRI updated guidelines intradermal intramuscular
rabies post-exposure prophylaxis India schedule guidelines
https://pmc.ncbi.nlm.nih.gov/articles/PMC12759123
https://ncdc.mohfw.gov.in/wp-content/uploads/2024/11/Rabies-…
India NCDC 2019 rabies prophylaxis guidelines intradermal schedule TRC Updated ID 4-site regimen RIG dose
https://ncdc.mohfw.gov.in/uploads/pdf/COH14.pdf
Rabies PEP Schedules Followed in India (Current, 2024-2025)
Regulatory Framework
- NCDC (National Centre for Disease Control) National Guidelines for Rabies Prophylaxis - last revised 2019, updated in line with WHO TRS1012 (2018)
- NCDC Operational Guidelines - "Rabies Free City Initiative" - published September 25, 2024 under the National Rabies Control Programme (NRCP)
- APCRI (Association for Prevention and Control of Rabies in India) consensus guidelines
- Drug Controller General of India (DCGI) approved intradermal route in 2006
Step 1 - Wound Care (Same as WHO)
| Action | Detail |
|---|---|
| Washing | Flush with soap and water under running tap for ≥15 minutes |
| Virucidal irrigation | Povidone-iodine or 70% alcohol |
| Suturing | Avoid immediate suturing; if needed, do after 24-48 hours with local RIG cover |
| Anti-tetanus | Give as indicated |
| Antibiotics | Give as indicated |
Step 2 - WHO Exposure Categories (Used in India)
| Category | Exposure | PEP Required |
|---|---|---|
| I | Touching/feeding animals, licks on intact skin | None |
| II | Nibbling of uncovered skin, minor scratches/abrasions without bleeding | Vaccine + wound care |
| III | Transdermal bites/scratches, licks on broken skin, mucous membrane contamination, bat contact | Vaccine + RIG + wound care |
Step 3 - India's Preferred PEP Vaccine Schedule
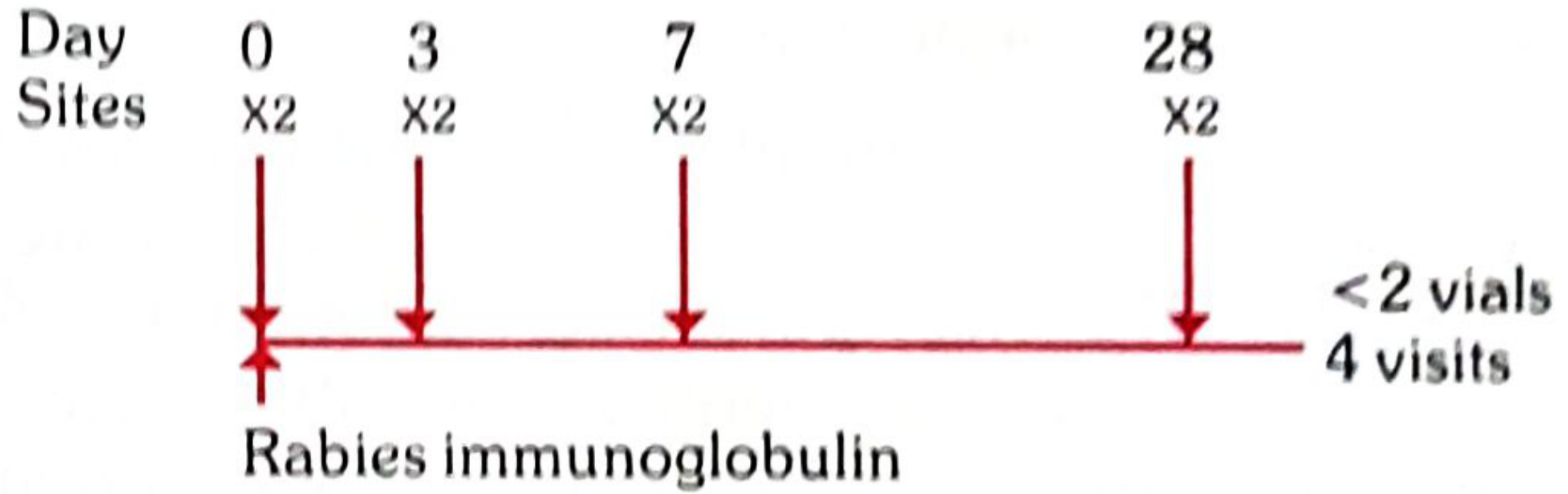
The "Updated Thai Red Cross (TRC)" Intradermal Schedule - India's Standard
| Day | Sites | Dose per site | Notes |
|---|---|---|---|
| 0 | 2 sites (both deltoids) | 0.1 ml each | + RIG for Cat III |
| 3 | 2 sites | 0.1 ml each | |
| 7 | 2 sites | 0.1 ml each | |
| 14 | Skipped | - | |
| 28 | 2 sites | 0.1 ml each |
- Total vaccine used: <2 vials vs. 5 vials for IM Essen
- Each 0.1 ml ID = 1/5 of an IM dose
- Injected into the deltoid or anterolateral thigh (intradermal, not subcutaneous)
- Advantages: 60-80% dose saving, lower cost, better compliance reported (77% vs. 60% for IM)
Important note: India has NOT yet adopted WHO's 1-week shortened ID schedule (Days 0, 3, 7 only). The Government of India is awaiting Indian-specific evidence before endorsing this change. The 4-week schedule (Days 0, 3, 7, 28) remains the official standard in India as of 2025.
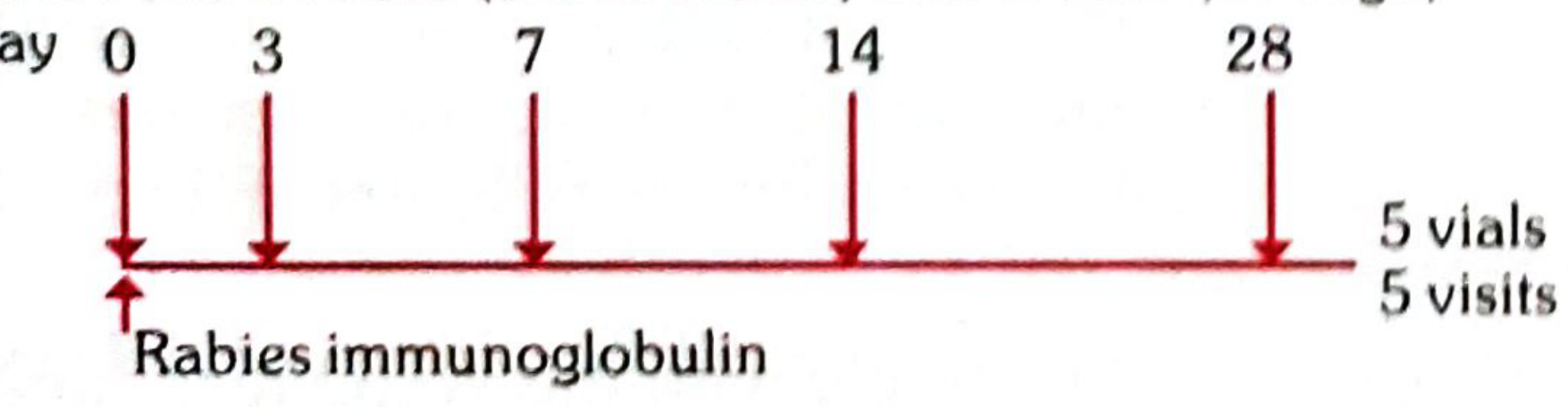
Intramuscular (IM) Alternative - Essen Regimen
| Day | Dose | Route | Site |
|---|---|---|---|
| 0 | 1.0 ml (full vial) | IM | Deltoid (thigh in <2 yrs) |
| 3 | 1.0 ml | IM | Deltoid |
| 7 | 1.0 ml | IM | Deltoid |
| 14 | 1.0 ml | IM | Deltoid |
| 28 | 1.0 ml | IM | Deltoid |
- Total: 5 vials, 5 visits
- Do NOT inject in the gluteal region
Step 4 - Rabies Immunoglobulin (RIG) in India
| Product | Dose | Route |
|---|---|---|
| Human RIG (HRIG) | 20 IU/kg body weight | Into and around wound |
| Equine RIG (ERIG) / F(ab')2 | 40 IU/kg body weight | Into and around wound |
- RIG is administered at the wound site only (changed from earlier practice of giving remainder IM at a distant site)
- This reduces RIG wastage without compromising efficacy
- Give on Day 0 only; not beyond Day 7
- No skin test before equine RIG (does not predict reactions)
- Be prepared for anaphylaxis management
Step 5 - Previously Vaccinated Individuals
| Route | Schedule | RIG |
|---|---|---|
| ID | 1-site, 0.1 ml on Days 0 and 3 | NOT required |
| IM | 1 dose on Days 0 and 3 | NOT required |
| Alternative (single visit) | 4-site ID on Day 0 only | NOT required |
Special Populations in India
| Population | Recommendation |
|---|---|
| Immunocompromised / HIV | Full 5-dose IM (Days 0, 3, 7, 14, 28) + full RIG for Category II and III; check RVNA 2-4 weeks post-series |
| Pregnancy | No contraindication - treat same as standard PEP |
| Children <2 years | Use anterolateral thigh for IM; standard ID schedule applies |
| Re-exposure in previously vaccinated | 1-site ID Days 0 & 3 only; no RIG |
India vs. WHO: Key Difference in 2025
| Aspect | India (NCDC 2019/2024) | WHO (2018-current) |
|---|---|---|
| Standard route | 2-site ID preferred | ID preferred |
| Standard ID schedule | Days 0, 3, 7, 28 (4 visits) | Days 0, 3, 7 (3 visits, 1-week) |
| Reason for difference | Awaiting Indian evidence on 1-week ID schedule | Recommends 1-week based on global RCT data |
| IM option | Essen 5-dose | Multiple options |
| RIG (equine) | Wound infiltration only | Wound + remaining IM at distant site |
Available Vaccines in India
| Vaccine | Cell Substrate | Brand Examples |
|---|---|---|
| PCECV (Purified Chick Embryo Cell Vaccine) | Chick embryo cells | Rabipur, Abhayrab |
| PVRV (Purified Vero Cell Rabies Vaccine) | Vero cells | Verorab, Indirab |
| PDEV (Purified Duck Embryo Vaccine) | Duck embryo | Lyssavac-N |
Key Takeaway
Are you sure that acc to latest guidelines rabies immunoglobulin is given only at wound site in India
India NCDC rabies immunoglobulin RIG administration wound site only remaining IM 2019 2024 guidelines
Correction on RIG Administration in India
What the Official NCDC Guidelines Actually Say
"As much of the calculated dose of RIG as is anatomically feasible should be infiltrated into and around the wound/s... After all the wound/s has been infiltrated, if any volume of RIG is remaining, it should be administered by deep intramuscular injection at a site distant from the vaccine injection site."
Where My Previous Claim Came From
"Rabies immunoglobulin is now administered at the site of wound only, reducing its wastage without compromising the efficacy."
Current Standard RIG Protocol in India (NCDC/APCRI)
| Step | Action |
|---|---|
| 1 | Calculate dose: ERIG = 40 IU/kg; HRIG = 20 IU/kg |
| 2 | Bring RIG to room temperature (25-30°C) before injection |
| 3 | Infiltrate as much as anatomically feasible into and around all wounds |
| 4 | Avoid multiple needle pricks into the same wound |
| 5 | Remaining volume (if any) - inject deep IM at a site distant from the vaccine site |
| 6 | RIG may be diluted with normal saline to ensure adequate volume for large/multiple wounds |
| 7 | Never administer RIG in the same syringe or same anatomical site as the vaccine |
| 8 | Keep patient under observation for at least 30 minutes after ERIG (anaphylaxis risk) |
| 9 | Skin testing before ERIG is NOT recommended (does not predict reactions) |
| 10 | RIG on Day 0 only; not beyond Day 7 |
Bottom Line
Can you give me a corrected version
Rabies PEP Schedules in India - Current Guidelines (2024-2025)
Regulatory Framework
- NCDC National Guidelines for Rabies Prophylaxis - revised 2019, aligned with WHO TRS1012 (2018)
- NCDC Operational Guidelines - "Rabies Free City Initiative" - published September 25, 2024 under the National Rabies Control Programme (NRCP)
- APCRI (Association for Prevention and Control of Rabies in India) consensus guidelines
- DCGI approved intradermal route in 2006
Step 1 - Wound Care
| Action | Detail |
|---|---|
| Washing | Flush with soap and water under running tap for ≥15 minutes |
| Virucidal irrigation | Povidone-iodine or 70% alcohol after washing |
| Suturing | Avoid immediately; if unavoidable, infiltrate RIG first, then apply minimum stay sutures after 24-48 hrs |
| Anti-tetanus | Give as indicated |
| Antibiotics | Give as indicated |
Step 2 - WHO Exposure Categories (Used in India)
| Category | Exposure | PEP Action |
|---|---|---|
| I | Touching/feeding animals, licks on intact skin | None |
| II | Nibbling of uncovered skin, minor scratches/abrasions without bleeding | Vaccine + wound care |
| III | Transdermal bites/scratches, licks on broken skin, mucous membrane contamination, bat contact | Vaccine + RIG + wound care |
Step 3 - Vaccine Schedules
India's Standard: Updated TRC 2-Site Intradermal (ID) Schedule
| Day | Sites | Dose per site | Visits |
|---|---|---|---|
| 0 | 2 (both deltoids) | 0.1 ml ID each | Visit 1 - also give RIG for Cat III |
| 3 | 2 | 0.1 ml ID each | Visit 2 |
| 7 | 2 | 0.1 ml ID each | Visit 3 |
| 14 | - | Skipped | - |
| 28 | 2 | 0.1 ml ID each | Visit 4 |
- Total vaccine needed: <2 vials (vs. 5 vials for IM Essen)
- Inject strictly intradermal (not subcutaneous) - a visible bleb must form
- Use deltoid or anterolateral thigh
Important: India has NOT yet adopted WHO's 1-week ID schedule (Days 0, 3, 7 only). The Government of India is awaiting Indian-specific evidence. The 4-week, 4-visit schedule remains the official national standard as of 2025. Note: Himachal Pradesh has trialled the 1-week schedule at pooling centres, but this is not a national policy.
Alternative: Essen Intramuscular (IM) Schedule
| Day | Dose | Route | Site |
|---|---|---|---|
| 0 | 1.0 ml (full vial) | IM | Deltoid (thigh in <2 yrs) - also give RIG for Cat III |
| 3 | 1.0 ml | IM | Deltoid |
| 7 | 1.0 ml | IM | Deltoid |
| 14 | 1.0 ml | IM | Deltoid |
| 28 | 1.0 ml | IM | Deltoid |
- Total: 5 vials, 5 visits
- Never inject in the gluteal region (fat delays absorption, impairs seroconversion)
Step 4 - Rabies Immunoglobulin (RIG) - Category III Only
Products Available in India
| Product | Dose | Notes |
|---|---|---|
| Equine RIG (ERIG) | 40 IU/kg body weight | More widely available in India; cheaper |
| Human RIG (HRIG) | 20 IU/kg body weight | Preferred if available; 150 IU/ml concentration |
| Monoclonal antibody (mAb) | As per product | Licensed in India since 2016 as alternative; limited availability |
RIG Administration Protocol (NCDC / APCRI Standard)
- Bring RIG to room temperature (25-30°C) before administration
- Infiltrate as much of the calculated dose as anatomically feasible into and around all wounds
- Avoid multiple needle pricks into the same wound
- If any volume remains after wound infiltration - administer by deep IM injection at a site distant from the vaccine injection site
- RIG may be diluted with normal saline to ensure adequate volume for large or multiple wounds
- Never administer RIG in the same syringe or same anatomical site as the vaccine
- RIG is given only once, on Day 0; not beyond Day 7 after the first vaccine dose
- Keep patient under observation for at least 30 minutes after ERIG administration (anaphylaxis risk)
- No skin test before ERIG - it does not predict reactions and should not delay administration; have anaphylaxis management ready
Step 5 - Previously Vaccinated Individuals
| Route | Schedule | RIG |
|---|---|---|
| ID | 1-site, 0.1 ml on Days 0 and 3 | NOT indicated |
| IM | 1 full dose on Days 0 and 3 | NOT indicated |
| Single-visit alternative | 4-site ID (0.1 ml × 4 sites) on Day 0 only | NOT indicated |
Vaccination cards are essential for making this determination. If prior vaccination cannot be documented, treat as unvaccinated.
Step 6 - Special Populations
| Population | Recommendation |
|---|---|
| Immunocompromised / HIV | Full 5-dose IM Essen (Days 0, 3, 7, 14, 28) + RIG for Cat II and III; check RVNA titre 2-4 weeks after series; may need additional dose |
| Pregnancy | No contraindication - treat same as standard PEP; rabies diagnosis in mother is not an indication for termination |
| Children <2 years | Use anterolateral thigh for IM injections; standard ID schedule applies |
| Re-exposure in previously vaccinated | 1-site ID Days 0 & 3 only; no RIG required |
| Immunocompromised with prior vaccination | Full PEP including RIG still required |
Available Vaccines in India
| Vaccine | Cell Substrate | Brand Examples |
|---|---|---|
| PCECV | Chick embryo cells | Rabipur, Abhayrab |
| PVRV | Vero cells | Verorab, Indirab |
| PDEV | Duck embryo | Lyssavac-N |
- All must have WHO potency ≥2.5 IU per IM dose
- Store at 2-8°C, protected from sunlight
- Use within 6-8 hours of reconstitution
- Switching between vaccine products or routes mid-course is acceptable if unavoidable
India vs. WHO - Key Difference in 2025
| Aspect | India (NCDC 2019/2024) | WHO (Current) |
|---|---|---|
| Preferred ID schedule | Days 0, 3, 7, 28 (4 visits, 4 weeks) | Days 0, 3, 7 (3 visits, 1 week) |
| Reason for difference | Awaiting Indian-specific evidence on 1-week regimen | Recommends 1-week based on global RCT data |
| RIG - remaining volume | IM at distant site (standard WHO protocol) | IM at distant site (wound-only infiltration in research settings only) |
| IM option | Essen 5-dose | Multiple options |
| Equine RIG skin test | NOT recommended | NOT recommended |
If we a person got post exposure prophylaxis today and got bitten by a dog tomorrow will he receive PEP again?
rabies PEP re-exposure during ongoing course bitten again second exposure management guidelines WHO CDC
Re-exposure During an Ongoing PEP Course - What Happens?
Short Answer
The Key Principle
- The new wound receives proper local treatment and RIG
- The existing vaccine course continues uninterrupted
Scenario: Bitten Today (Day 0), Bitten Again Tomorrow (Day 1)
| Question | Answer |
|---|---|
| Start a brand new PEP course? | No |
| Continue the existing schedule (Days 3, 7, 14/28)? | Yes, unchanged |
| Give RIG for the new wound? | Yes - if the new wound is Category III and RIG was not already given, OR was given but the new wound site was not infiltrated |
| Give RIG at the new wound site? | Yes - the new wound must be infiltrated, provided it is still within the Day 7 window |
| Give another dose of vaccine? | No - no additional vaccine doses; the ongoing schedule suffices |
Why? On Day 1, the person has received only one vaccine dose - active immunity has not yet developed. RIG is still indicated (within the Day 0-7 window) for the new wound. The vaccine schedule already in progress will cover both exposures.
The 3-Month Rule (WHO / NCDC)
| Timing of Re-exposure | Status | Action |
|---|---|---|
| During ongoing PEP (Day 1 in your scenario) | Partially immunized | Continue existing course; RIG for new wound if within Day 7 window |
| Within 3 months of completing a full PEP/PrEP course | Considered immune | No new PEP required at all |
| More than 3 months after completing a full course | Re-exposure protocol | 2 vaccine doses on Days 0 and 3 only; no RIG |
What Exactly Should Be Done in Your Scenario (Day 0 PEP, Bitten on Day 1)
| Step | Action |
|---|---|
| 1. Wound care | Immediate thorough wash with soap and water ≥15 min + virucidal agent for the new wound |
| 2. RIG | Infiltrate RIG into the new wound (still within the Day 7 window); total dose must not exceed the weight-based maximum (ERIG 40 IU/kg, HRIG 20 IU/kg) across both wounds combined |
| 3. Vaccine | Do not give an extra dose; continue the original schedule (Day 3, Day 7, Day 28 for India's ID schedule) |
| 4. Documentation | Record both exposure events on the vaccination card |
What if RIG Was Already Given on Day 0 at Maximum Dose?
- If the full weight-based RIG dose was already given and infiltrated on Day 0, you cannot give more RIG (excess RIG suppresses the vaccine-induced antibody response)
- In this case, only wound care is performed for the new bite
- The ongoing vaccine course provides the protection - by Day 3-7, some active immunity is already developing
Summary
Day 0: Bitten → Full PEP started (Vaccine Day 0 + RIG for Cat III)
Day 1: Bitten again
↓
Wound care for new bite ✓
RIG to new wound only (if within Day 7 window & dose not exceeded) ✓
NO new vaccine dose ✓
Continue existing PEP schedule (Day 3, 7, 28) ✓
What is the 3 month rule?
WHO rabies PEP "3 months" re-exposure previously vaccinated guideline rule
The "3-Month Rule" - What It Actually Is
Honest Clarification First
What the Underlying Principle Actually Is
For re-exposed patients who can document previous complete PrEP or PEP with a CCEEV, a shortened re-exposure regimen applies - 2 doses on Days 0 and 3 only, no RIG.
The Actual Framework for Re-exposure
| Situation | What Applies |
|---|---|
| Re-exposed and completed a full, documented PEP or PrEP course (regardless of time elapsed, as long as antibody memory is expected) | Shortened re-exposure regimen: 2 vaccine doses - Days 0 and 3 only; no RIG |
| Re-exposed, received at least 2 doses of a prior PEP series (even if course was not completed) | Same shortened regimen: Days 0 and 3; no RIG |
| Re-exposed, but prior vaccination cannot be documented | Treat as fully unvaccinated - full PEP including RIG |
| Re-exposed during an ongoing course (your original scenario) | Continue the existing schedule; RIG to new wound if within Day 7 window |
Where Does "3 Months" Come From?
- Bangladesh National Guidelines (citing it as a WHO recommendation) - no new PEP if re-bitten within 3 months of a complete course
- Some regional/state health authority guidelines (e.g., New York State mentions exposures >3 months ago being managed case-by-case for low-risk animals)
- It reflects the practical understanding that immunological memory from a completed cell-culture vaccine course is robust within the first few months, when neutralizing antibody titres are reliably above the protective threshold of 0.5 IU/ml
The Correct Clinical Decision Tree for Re-exposure
Re-exposed to suspected rabid animal?
↓
Wound care always first (wash ≥15 min)
↓
Can document previous complete PEP/PrEP
with a cell-culture vaccine?
↓ ↓
YES NO
↓ ↓
2 doses Full PEP
Days 0 & 3 (vaccine +
No RIG RIG for Cat III)
Bottom Line
- Documented complete prior vaccination → shortened re-exposure regimen (Days 0 & 3, no RIG), regardless of time elapsed
- Undocumented or incomplete prior vaccination → treat as unvaccinated, full PEP
- The vaccination card is therefore the single most important document a patient should retain after completing PEP
In India for what animal bites Rabies PEP is not required
India NCDC rabies PEP not required which animals rodents birds squirrel cow guidelines
Animal Bites in India - When is Rabies PEP NOT Required?
Animals for Which PEP is Generally NOT Required in India
1. Domestic Rodents, Squirrels, Hares & Rabbits
"Exposure to domestic rodents, squirrel, hare and rabbits do not ordinarily require PEP." - NCDC Guidelines
- Includes: house rats, mice, squirrels, rabbits, hares, bandicoots
- Rationale: Rodents are not primary hosts of rabies virus and do not play a role in its transmission or maintenance in India
- Very few examples of rabies virus infection have ever been observed in Indian rodents
- Exception: Bites by wild rats/rodents in unusual circumstances - consult an infectious disease physician; PEP may be considered on a case-by-case basis
2. Bats
"Bat rabies has not been conclusively proved in India and hence, at present, exposure to bats does not warrant PEP." - NCDC Guidelines
- Only one reported case of bat-transmitted rabies in India (1954); none since
- Lyssaviruses have been detected in bats globally, but not confirmed in Indian bats
- Exception: Bat bites in unusual circumstances may be considered for PEP after expert consultation
- This is a major difference from Western guidelines (CDC/WHO globally strongly recommend PEP for all bat exposures)
3. Birds
- Birds are not known to transmit rabies - they are not mammals and do not carry rabies virus
- Bird bites/scratches do not require rabies PEP
4. Category I Exposures from ANY Animal
- Touching or feeding animals, licks on intact skin - no PEP regardless of species
5. Consumption of Cooked Meat of a Rabid Animal
- Cooking kills the rabies virus - no PEP required
- Raw meat from a rabid animal - PEP is warranted
6. Drinking Milk of a Rabid Animal
- No documented cases of transmission through milk
- No PEP required (though boiling milk is always recommended as routine practice)
7. Contact with Rabies Patient (Human)
- PEP is not recommended for persons who had contact with a rabies patient
- Exception only: Direct exposure to saliva or organs of a rabid person (e.g., organ transplant, deep bite from patient) - PEP may be considered in these special circumstances
Animals for Which PEP IS Always Required in India
| Animal | Frequency of Transmission | PEP Needed? |
|---|---|---|
| Dogs | ~96-97% of all human rabies deaths | Always |
| Cats | Common | Always |
| Mongoose, foxes, jackals, wild dogs | 2% of cases | Always (Category III) |
| Monkeys | Occasional | Yes |
| Horses, donkeys | Occasional | Yes |
| Cows, buffaloes, goats, sheep, pigs | Rare but documented | Yes |
| All wild animals in forest/wild | Variable | Always treated as Category III |
Key rule from NCDC: "Bite by all wild animals should be treated as Category III exposure. All animal bites in forest or in the wild should be treated as Category III exposure."
Summary Table
| Animal | PEP in India? | Notes |
|---|---|---|
| Dog / Cat | YES | Mainstay of rabies in India |
| Monkey | YES | |
| Mongoose / Fox / Jackal | YES | Category III |
| Cow / Buffalo / Horse / Donkey | YES | Rare but possible |
| Goat / Sheep / Pig | YES | Rare |
| All wild animals | YES | Automatically Category III |
| House rat / Mouse | NO (ordinarily) | Wild rats - consult physician |
| Squirrel / Hare / Rabbit | NO (ordinarily) | |
| Bat | NO (currently in India) | Major exception vs. global guidelines |
| Birds | NO | Not mammals; cannot carry rabies |
| Licks on intact skin (any animal) | NO | Category I |
| Cooked meat / boiled milk ingestion | NO | Virus killed by heat |
Important Caveat
"Rabies does not give a second chance as it is 100% fatal once disease occurs. Hence, it is better to over-treat rather than under-treat animal bite cases."
Is tetanus a saprozoonotic disease
tetanus saprozoonotic disease classification zoonosis Park preventive medicine
Is Tetanus a Saprozoonotic Disease?
Short Answer: It Depends on Which Classification System You Use
The Classification of Zoonoses
| Type | Definition | Examples |
|---|---|---|
| Orthozoonosis (Direct zoonosis) | Transmitted directly from vertebrate animal to human; needs only one vertebrate host | Rabies, brucellosis, plague |
| Cyclozoonosis | Requires >1 vertebrate host to complete the cycle | Taeniasis (T. solium, T. saginata), hydatid disease |
| Metazoonosis | Requires an invertebrate (arthropod) intermediate host; agent multiplies/develops in it | Malaria, dengue, filariasis |
| Saprozoonosis | Has both a vertebrate host AND a non-animal (abiotic) reservoir/developmental site - soil, organic matter, plants | Histoplasmosis, listeriosis, Erysipelothrix infection |
Where Does Tetanus Fit?
- Reservoir: Primarily soil and organic matter (abiotic environment); also found in intestines of horses, cattle, sheep, dogs, cats, and humans (as harmless gut flora)
- Transmission to humans: Via contaminated wounds - spores from soil enter tissue
- No animal-to-human transmission is required or typical
- Does NOT need a vertebrate host to survive or complete its cycle - it persists in soil indefinitely as spores
The Sapronosis vs. Saprozoonosis Debate
| Term | Definition | Applies to Tetanus? |
|---|---|---|
| Saprozoonosis (older WHO term) | Agent has both a vertebrate animal host and a non-animal reservoir | Partially - animals can harbor C. tetani in gut, but this is incidental |
| Sapronosis (more precise modern term) | Agent's primary/essential reservoir is abiotic (soil, water, organic matter); vertebrate animal reservoir is not required | Yes - this is the more accurate term |
"Tetanus, gas gangrene, botulism, anthrax... should be called sapronoses" because their infective spores survive and are produced primarily in the abiotic environment, not requiring a vertebrate host.
Why Is Tetanus Listed as Saprozoonosis in Indian Textbooks?
- The agent has a significant soil/organic matter reservoir, AND
- Animals can serve as incidental or secondary hosts
Tetanus = Saprozoonosis ✓ (for examination purposes in India)
Summary
| Context | Classification of Tetanus |
|---|---|
| Indian PSM / Park's textbook / exam answer | Saprozoonosis ✓ |
| Modern epidemiological literature (WHO/CDC) | Sapronosis (more precise - abiotic reservoir is primary; animal host not essential) |
| Is it a true zoonosis? | No - tetanus is not transmitted from animals to humans in the conventional sense |
The Conceptual Distinction in One Line
- Saprozoonosis = needs both a vertebrate animal host and an abiotic reservoir
- Sapronosis = abiotic reservoir (soil/organic matter) is sufficient; animals not required as reservoir