Air transport when to consider And problems need to be taken care during air transport
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information. Let me compile a thorough, well-organized answer.
Air Medical Transport (AMT)
When to Consider Air Transport
Air transport is considered when speed and level of care cannot be achieved by ground. There are two types:
- Primary (scene) response: Aircraft goes directly to accident/illness scene
- Secondary (interfacility): Moves patient from outlying hospital to higher-level facility
General Criteria for Air Medical Transport
(From Rosen's Emergency Medicine, Box E13.3)
- Distance to the closest appropriate facility is too great for safe, timely ground transport
- Patient's clinical condition requires that time spent in transport be minimized
- Condition is time-critical, requiring specific treatment not available at the referring hospital
- Ground transport delay is likely to worsen the patient's condition
- Patient requires critical care life support during transport not available from local ground ambulance
- Patient is in a location inaccessible to regular ground traffic
- Local ground units are unavailable for long-distance transport
- Use of local ground transport would leave the area without adequate EMS coverage
Practical Decision Questions
(Tintinalli's Emergency Medicine, Table 3-1)
- Is minimization of time out of hospital important?
- Is time-sensitive evaluation/treatment involved and not available at the referring facility?
- Is the patient inaccessible to ground transport?
- What are the transport route weather conditions?
- Does patient weight preclude air transport?
- Are landing facilities available near the referring hospital?
- Is critical-care life support required that is unavailable with ground transport?
Note: Fixed-wing transport is preferred when weather is poor or transport distance exceeds 150-200 miles. Helicopters reduce travel time by up to 75% vs. ground.
Specific Indications by Category
Trauma Indications (Table 3-2, Tintinalli's)
General/mechanism:
- Trauma score <12, unstable vital signs
- Multisystem injuries
- Age <12 or >55, pregnant patients with significant trauma
- Ejection from vehicle, pedestrian/cyclist struck, death in same compartment
- Penetrating trauma to head, neck, chest, abdomen, or pelvis
- Crush injury, fall from height, near-drowning
Neurologic:
- GCS <10, mental status deterioration
- Obvious skull fracture, spinal cord injury
Thoracic:
- Major chest wall injury (flail chest), pneumothorax, hemothorax, suspected cardiac injury
Abdominal/pelvic:
- Significant abdominal pain after injury, seatbelt sign, unstable pelvis, open pelvic fracture with hypotension
Orthopedic:
- Amputation (partial or complete)
- Fracture/dislocation with vascular compromise, limb ischemia
- Two or more long-bone fractures
Thermal:
- Burns >20% BSA, facial/hand/foot burns, inhalation injury, chemical/electrical burns
Non-Trauma Indications (Table 3-3, Tintinalli's)
| Category | Examples |
|---|---|
| Cardiac | Acute coronary syndromes, cardiogenic shock, cardiac tamponade |
| Critical medical/surgical | Pre-transport cardiac/respiratory arrest, mechanical ventricular assist, continuous vasoactive medications, airway at risk of deterioration, severe poisoning, need for hyperbaric O2, emergent dialysis, unstable GI bleeding, aortic dissection |
| Neurologic | CNS hemorrhage, spinal cord compression, status epilepticus |
| Obstetric | High-risk delivery beyond local capability, preterm labor <34 weeks or fetal weight <2000g, preeclampsia/eclampsia, third-trimester hemorrhage |
| Neonatal | Gestational age <30 weeks, supplemental O2 >60%, pneumothorax, surgical emergencies (diaphragmatic hernia, NEC) |
Problems to Manage During Air Transport
1. Altitude-Related Physiological Changes (Most Important)
Boyle's Law - Gas Expansion
At altitude, decreased barometric pressure causes enclosed gas volumes to expand. This has critical clinical implications:
- Pneumothorax - a small, untreated pneumothorax can expand and become tension pneumothorax. Not all small pneumothoraces need pre-transport decompression, but this must be carefully assessed
- Bowel gas - abdominal distension; consider NGT insertion for unconscious patients
- Endotracheal tube (ETT) cuff - ETT cuff pressure increases an average of 33.9 cm H2O at ~2260 ft altitude, potentially exceeding tracheal mucosal perfusion pressure and causing injury. Monitor and adjust cuff pressure to target 20-30 cm H2O using a cuff manometer
- IABP/tamponading devices - esophageal balloon tamponade devices may expand and cause problems
- Air in IV lines - small air emboli may enlarge
- Middle ear/sinus barotrauma - in patients with upper respiratory tract issues
Dalton's Law - Reduced Partial Pressure of Oxygen
- At cabin altitude, partial pressure of inspired O2 falls even with the same FiO2
- Hypoxemia is a major risk for critically ill patients; supplemental oxygen is mandatory
- Even crew members may need supplemental O2 at higher altitudes in some western US programs
2. Temperature
- Temperature drops with altitude (~2°C per 300 m / 1000 ft)
- Patients are at risk of hypothermia, especially if already in shock or with burns
- Active warming may be needed in flight
3. Dehydration
- Low humidity in aircraft cabins increases insensible fluid losses
- Patients with prolonged flights should have fluid management addressed
4. Noise and Vibration
- Noise makes auscultation impossible (breath sounds, heart sounds, bowel sounds)
- Rely on visual alarms rather than auditory alarms on ventilators and monitors
- Vibration can interfere with fine motor tasks and monitoring equipment accuracy
- ECG artifact may be generated from vibration
5. Ergonomic Constraints
- Confined cabin space limits procedures and access to the patient
- Preflight intubation should be performed if the patient is at risk of airway deterioration (easier on the ground than in flight)
- Limited number of personnel and equipment that can be carried
6. Motion Sickness
- Affects both crew and awake patients
- Prophylactic anti-emetics may be considered for susceptible patients
7. Safety Hazards (Ground Operations)
- Main rotor blades dip lower at slow rotor speeds (start-up/shutdown) - increased strike risk
- Tail rotor blades are virtually invisible at full speed - never approach from the rear
- Rotor wash can propel debris
- Personnel and vehicles must stay at least 100 ft (30 m) from the landing zone
8. Contraindications / Precautions to Bear in Mind
- Traumatic cardiac arrest - air transport shows very low resuscitation rates; most programs accompany these patients by ground to the nearest facility
- Imminent delivery - in-flight delivery is a major resuscitation problem for mother and infant
- Patient weight - may preclude air transport (aircraft weight limits)
- Weather conditions - may make helicopter flight impossible; consider fixed-wing
Summary Table: Problems and Solutions
| Problem | Management |
|---|---|
| Gas expansion (pneumothorax) | Reassess pre-flight; drain if indicated |
| ETT cuff overinflation | Cuff manometer; maintain 20-30 cm H2O |
| Bowel gas/aspiration risk | NGT insertion for unconscious patients |
| Hypoxemia | Supplemental oxygen for patient and crew |
| Hypothermia | Active warming, insulated blankets |
| Noise (monitoring) | Visual alarms; pre-flight auscultation |
| Airway deterioration in flight | Intubate before transport if risk exists |
| Limited access/confined space | All procedures completed pre-flight when possible |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Chapter 3 - Air Medical Transport
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Chapter e13 - Specific Issues in Air Medical Transport (Box E13.3, Fig. e13.1)
Components of medical action plan in mass gathering event
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have all the key content needed for a comprehensive answer. Let me compile it.
Components of a Medical Action Plan (MAP) for Mass Gathering Events
(Based on Tintinalli's Emergency Medicine, Chapter 4 - Mass Gathering Medicine)
1. Physician Medical Oversight
Every mass gathering event must have an identified physician medical director responsible for developing and overseeing the MAP. Requirements:
- Board certified in emergency medicine (increasingly, board certified in EMS)
- Current medical license for the state(s) where the event is located
- Experience in EMS medical direction and mass gathering medicine
Two types of oversight the director must plan:
- Indirect oversight - written protocols providing standardized directions for traumatic and medical conditions; must be at least commensurate with local EMS protocols
- Direct oversight - real-time communication with medical providers during the event; the medical director should be on site as much as possible
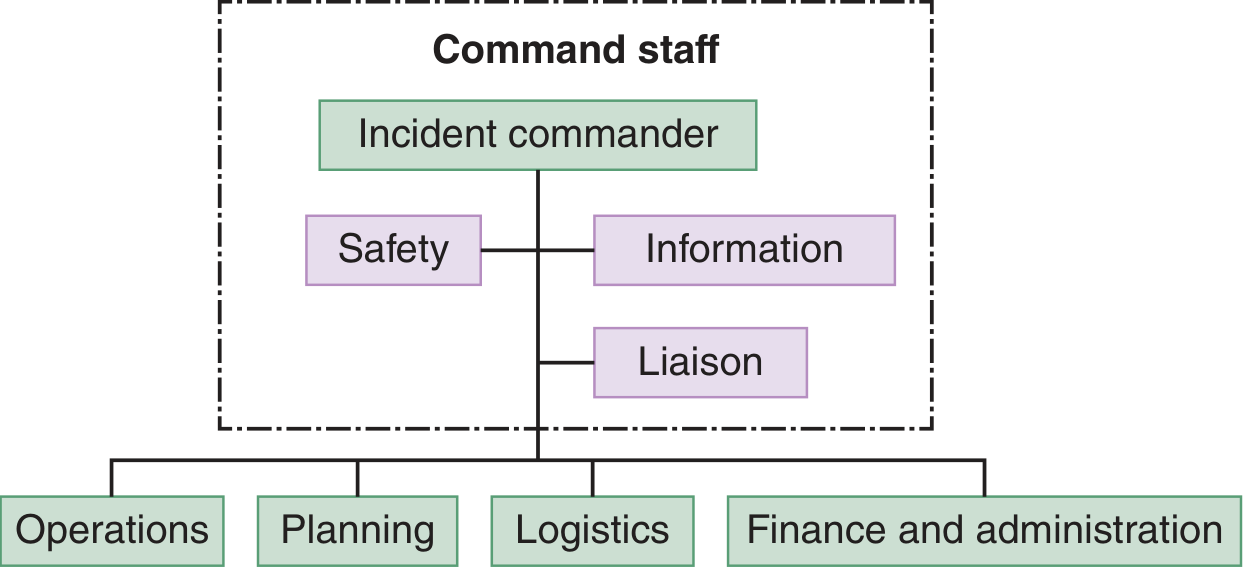
2. Command and Control
An organized command and control system must be established. The Incident Command System (ICS) is the recommended framework - it can scale for any size event and enables multiple agencies to communicate using common terminology.
ICS structure:
- Command - always established; Incident Commander heads the structure with Safety, Information, and Liaison officers
- Operations - where medical care delivery lives ("the doers"); includes EMTs, paramedics, nurses, PAs, physicians
- Logistics - resources and support
- Planning - situation tracking
- Finance - cost and administration
The physician's role within ICS should focus on direct patient care oversight, not the global issues handled by the incident commander.
3. Force Protection Medical Support
Medical providers who become sick or injured will consume resources intended for the public and distract other providers. The plan must include:
- Dedicated medical care for the medical and law enforcement personnel themselves
- Communication with law enforcement to ensure protection of medical providers
- Rapid response capability for any location should the situation become unsafe
- Awareness of threats: visible threats (crowds) and hidden threats (explosives, weapons)
4. Event Reconnaissance (Site Assessment)
Before the event, the medical director and team must conduct a site survey to:
- Identify potential risks for morbidity
- Review adequacy of exits and routes of ingress/egress
- Identify the geographic area the medical sector is responsible for
- Determine ideal locations for: base of operations, fixed medical care sites, mobile unit staging areas
- Account for predicted traffic flow and sites of high-volume medical need
- Identify natural geographic barriers
- Note the location of receiving medical facilities
- Meet with jurisdictional 9-1-1 EMS medical directors to discuss MCI response plans
- Develop backup plans for all key functions
5. Event Negotiations (Interagency Agreements)
Developing the MAP requires negotiation and agreements with multiple stakeholders:
| Stakeholder | Agreement Content |
|---|---|
| Event planners | Locations for fixed/mobile units, level of care, resource provision, financing, liability |
| Local EMS | Transport of patients out of the event to receiving hospitals |
| Hospitals | Transfer and acceptance agreements |
| Local law enforcement | Traffic flow management, security |
| Dept. of Homeland Security | National-scale security/disaster response (for large events) |
Regardless of who finances supplies, the medical director should retain ultimate control over the acquisition and maintenance of critical medical supplies.
6. Medical Staffing
Staffing must be scaled to the event based on risk factors and anticipated patient presentation rate. Key considerations:
- Appropriate mix of providers (EMTs, paramedics, nurses, physicians)
- Mobile units (roving personnel to reach patients who cannot access fixed facilities)
- Fixed treatment posts
- Dedicated personnel for performer/VIP/law enforcement medical support
Factors that influence staffing level:
- Estimated crowd size and density
- Duration of the event
- Type of event (concert, sporting event, religious gathering)
- Weather and environmental conditions
- Availability of alcohol/drugs
- Crowd demographics (age, medical conditions)
- Distance from receiving hospitals
7. Medical Equipment and Supplies
The plan must detail:
- Equipment at each fixed and mobile unit (BLS and ALS)
- Medications and antidotes appropriate to anticipated presentations
- Supply chain and restocking protocols
- Special equipment (e.g., AEDs, defibrillators, IV fluids, airway equipment)
- Equipment for environmental emergencies (heat stroke cooling devices, hypothermia management)
8. Treatment Facilities
The plan must specify:
- Fixed treatment posts - clearly marked, accessible to all members of the public including those with disabilities (ADA-compliant)
- Triage area - to sort patients by acuity
- Advanced care area - for critical patients
- Mobile medical personnel - wearing high-visibility vests/clothing for easy public identification
- Pamphlets and signage to alert the public about how to access care
9. Transportation Plan
Includes:
- On-site transport (golf carts, ATVs, stretchers) to bring patients from the crowd to treatment posts
- Ground EMS for transport to hospitals
- Air transport consideration for critically ill or geographically isolated patients
- Pre-designated receiving hospitals with confirmed acceptance agreements
- Clear protocols for activating additional transport resources
10. Communications
A robust communications system is the backbone of any successful mass gathering event. The plan must address:
System design factors:
- Size and geography of the venue
- Number of participants
- Budget
- Environmental factors (temperature extremes, water, noise)
Modalities to consider:
- Consumer walkie-talkies (1-2 mile range, limited)
- Cellular/landline phones (may be overwhelmed by high user density during a crisis)
- Two-way radios (VHF, UHF, 800 MHz) with repeater antennas for extended range
- Trunked radio systems for large-scale, central-controlled communication
Key requirements:
- Communications center co-located with the event command center when possible
- Network separate from surrounding EMS jurisdiction and dedicated solely to the event
- Linked to: PSAP (9-1-1), local emergency management, hospital EDs, public health departments
- Special devices for high-noise venues (concerts, motor sports)
11. Public Health Considerations
(Table 4-4, Tintinalli's)
The MAP should address:
- Access to potable water
- Proper waste management (human and non-human)
- Food service management to prevent foodborne illness
- Road/traffic management to prevent injuries
- Other injury prevention measures
- Plans for large-scale natural or man-made disaster
12. Mass Casualty Incident (MCI) Planning
The event medical director must contribute to and have full working knowledge of the MCI action plan:
- Triage protocols (START triage or equivalent)
- Patient surge management
- Resource request procedures
- Activation criteria for MCI
- Communication with surrounding hospitals about mass casualty capability
- Integration with local/regional emergency management
13. Documentation
A documentation system must be in place for all patient encounters:
- Standardized patient encounter form capturing: demographics, presenting complaint, acuity, medications administered, disposition
- Data used for post-event analysis and quality improvement
- Medical records that comply with patient privacy regulations
- Data sharing with local health departments if required (for public health surveillance)
Summary Diagram
MEDICAL ACTION PLAN
├── 1. Physician Medical Director & Oversight
├── 2. Command & Control (ICS)
├── 3. Force Protection for Medical Staff
├── 4. Site Reconnaissance & Risk Assessment
├── 5. Interagency Agreements & Negotiations
├── 6. Medical Staffing Plan
├── 7. Equipment & Supplies
├── 8. Treatment Facilities (Fixed + Mobile)
├── 9. Transportation Plan
├── 10. Communications System
├── 11. Public Health Measures
├── 12. MCI/Disaster Contingency Plan
└── 13. Documentation System
Source: Tintinalli's Emergency Medicine: A Comprehensive Study Guide - Chapter 4, Mass Gathering Medicine
This is a shared conversation. Sign in to Orris to start your own chat.