Mechanism of action of local anesthesia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a thorough breakdown of the mechanism of action of local anesthetics, drawn from authoritative textbooks.
Mechanism of Action of Local Anesthetics
Core Mechanism: Sodium Channel Blockade
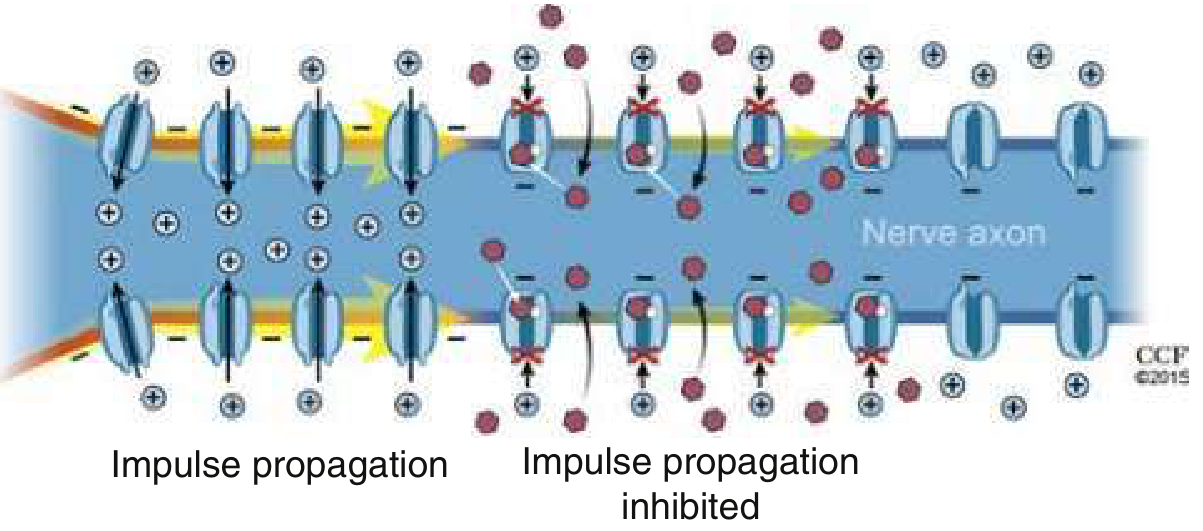
Local anesthetics produce reversible nerve blockade by inhibiting voltage-gated sodium (Na+) channels in the axonal membrane. This prevents sodium influx, which is required for the upstroke of the action potential. Without a rising action potential, the firing threshold is never reached and nerve impulse conduction is blocked entirely.
Step-by-Step Mechanism
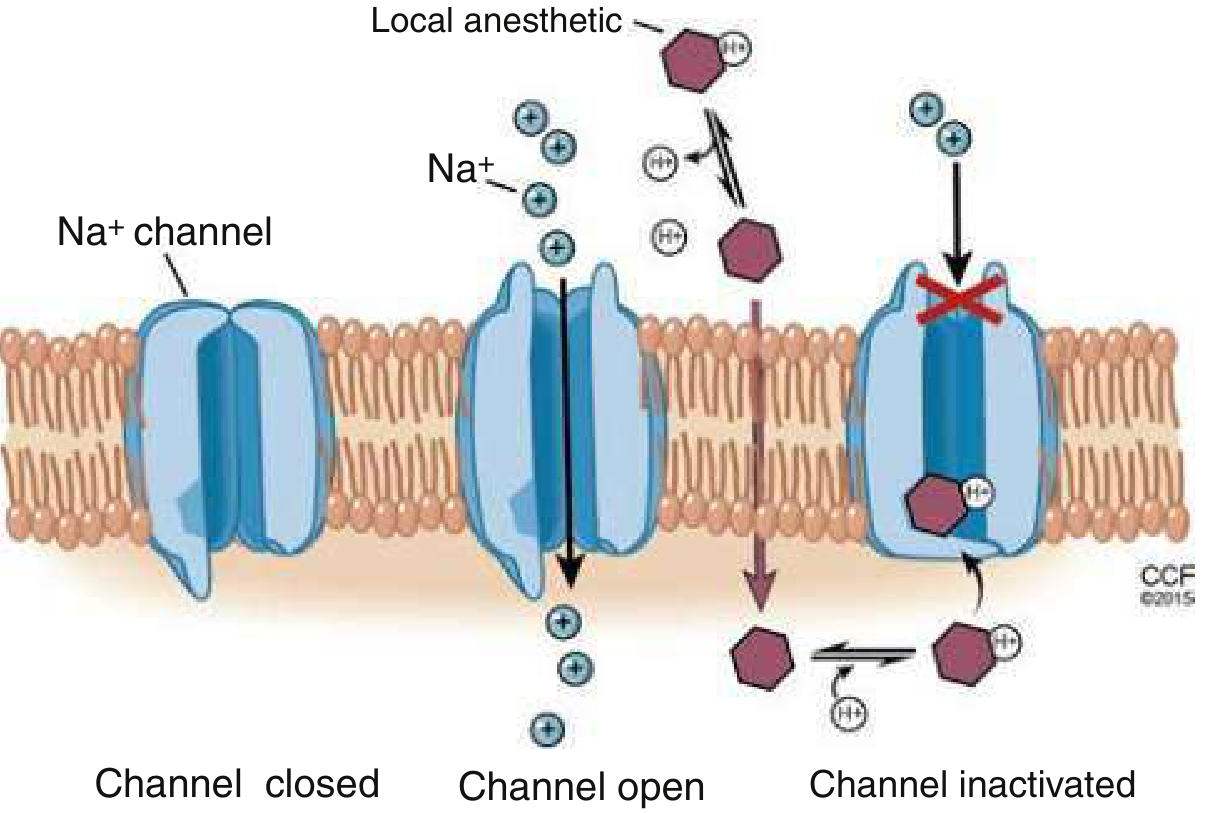
1. The drug exists in two forms
Local anesthetic solutions contain both:
- An uncharged (lipid-soluble, free base) form - able to cross tissue barriers and the nerve membrane
- A charged (cationic) form - the pharmacologically active form at the channel
The ratio of these two forms depends on the tissue pH and the drug's pKa. In an alkaline environment (higher pH), more uncharged form is present, which explains why local anesthetics work faster in normal (non-inflamed) tissue. Inflamed, acidic tissue reduces efficacy because less uncharged drug is available for membrane penetration.
2. Tissue penetration
The uncharged lipid-soluble form crosses the perineurium, nerve sheath, and axonal membrane to reach the axoplasm (interior of the nerve).
3. Re-equilibration inside the axon
Once inside, the drug re-equilibrates back into both charged and uncharged forms based on the axoplasmic pH.
4. Channel binding and blockade
The charged (cationic) form enters the sodium channel from the axoplasmic (inner) side and binds to a specific receptor site within the channel pore. This stabilizes the channel in its inactivated state, blocking Na+ influx. With the channel inactivated:
- The rate of rise and amplitude of depolarization decrease
- The firing threshold is not reached
- No action potential is formed
- Conduction is blocked
This is called the "specific receptor" theory and is the dominant accepted mechanism. (Note: it cannot fully explain the action of neutral compounds like benzocaine, which act via a separate membrane-expansion or direct pore-blocking mechanism without needing the charged form.)
Use-Dependent (Phasic) Blockade
Local anesthetics bind preferentially to sodium channels in their open or inactivated states rather than the resting (closed) state. This means nerves that fire frequently (high frequency) are blocked more readily - a property called use-dependent or phasic blockade. Rapidly firing pain fibers are therefore more susceptible than resting motor fibers.
Physicochemical Properties Governing Activity
| Property | Determines | Example |
|---|---|---|
| pKa | Onset of action | Lower pKa → more uncharged form → faster onset (e.g., lidocaine is faster than bupivacaine) |
| Lipid solubility | Potency | Higher solubility → better membrane penetration → greater potency (e.g., bupivacaine > lidocaine) |
| Protein binding | Duration | Tighter binding → longer duration (e.g., bupivacaine > procaine) |
Differential Nerve Blockade
Local anesthetics block nerve fibers in a predictable order based on fiber size and myelination:
- Small myelinated fibers (Aδ) - pain, temperature - blocked first
- Small unmyelinated fibers (C) - pain, autonomic
- Large myelinated fibers (Aα, Aβ) - touch, pressure, motor - blocked last (require higher concentrations)
This produces the characteristic clinical sequence: loss of pain → temperature → touch → proprioception → motor function.
Role of Epinephrine
Adding epinephrine to a local anesthetic causes local vasoconstriction, which:
- Slows systemic absorption
- Prolongs duration of anesthesia
- Reduces the peak plasma concentration (less systemic toxicity)
Summary
| Step | Event |
|---|---|
| Injection | Drug equilibrates into uncharged and charged forms based on tissue pH |
| Tissue penetration | Uncharged form crosses barriers |
| Inside axon | Re-equilibration; charged form predominates |
| Channel binding | Charged form binds inside Na+ channel from axoplasmic side |
| Blockade | Channel locked in inactivated state; Na+ influx blocked |
| Result | No action potential; no impulse conduction; reversible anesthesia |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 633
- Rosen's Emergency Medicine: Concepts and Clinical Practice, p. 3097
- Lippincott Illustrated Reviews: Pharmacology, p. 692
This is a shared conversation. Sign in to Orris to start your own chat.