Para thyroid adenoma
"parathyroid adenoma" AND "primary hyperparathyroidism"
Parathyroid Adenoma
Definition and Epidemiology
- Robbins Pathologic Basis of Disease, p. 1010
- Schwartz's Principles of Surgery, p. 1665
Etiology and Molecular Pathogenesis
-
Cyclin D1 (CCND1) gene inversion - A pericentromeric inversion on chromosome 11 relocates the CCND1 gene adjacent to the PTH gene promoter, causing overexpression of cyclin D1 (a cell cycle regulator), driving cell proliferation. Even without this inversion, cyclin D1 is overexpressed in up to 40% of adenomas.
-
MEN1 gene mutation - ~15% of sporadic tumors carry somatic mutations of the MEN1 tumor suppressor gene (chromosome 11q13), with loss of heterozygosity (LOH) at the second allele.
-
CDC73 mutation - Encodes parafibromin; mutated in ~70% of sporadic parathyroid carcinomas and occasionally in adenomas. Germline CDC73 mutations cause the rare hyperparathyroidism-jaw tumor (HPT-JT) syndrome.
- Robbins Pathologic Basis of Disease, p. 1010
Pathology
Gross Appearance
- Almost always solitary (double adenomas occur in only 1.7-12% of PHPT cases)
- Weight averages 0.5-5 g (mean ~0.55 g; tumours up to 53 g recorded)
- Well-circumscribed, soft, tan to reddish-brown (or yellow-red to orange-brown) nodule
- More severe hypercalcemia correlates with larger adenoma size
- The remaining glands are normal or shrunken due to feedback suppression (helps distinguish from hyperplasia)
Microscopic Appearance
- Sheets of uniform, polygonal chief cells with small, centrally placed nuclei and pale/vacuolated cytoplasm
- Nests of larger oxyphil cells are also present; rarely, adenomas are composed entirely of oxyphil or water-clear cells
- A rim of compressed, non-neoplastic parathyroid tissue may be visible at the edge
- Mitotic figures are rare; bizarre/pleomorphic nuclei (endocrine atypia) may be present - this is NOT a criterion for malignancy
- Stromal fat is inconspicuous (unlike normal parathyroid)
- Robbins Pathologic Basis of Disease, p. 1011
- Scott-Brown's Otorhinolaryngology, p. 2113
Variants of Parathyroid Adenoma (WHO 4th Ed, 2017)
| Variant | Key Features |
|---|---|
| Cystic adenoma | Cystic ab initio or secondary to subsiding post-infarction haematoma |
| Lipoadenoma (parathyroid hamartoma) | Rare; admixture of parenchymal cells with 20-90% mature adipocytes; ~50% associated with hypercalcaemia |
| Oxyphil adenoma | Composed entirely of oxyphil cells |
| Water-clear adenoma | Substantially composed of water-clear cells |
| Papillary variant | Rare; may mimic papillary thyroid carcinoma |
- Scott-Brown's Otorhinolaryngology, p. 2207
Clinical Presentation
Asymptomatic (most common today)
Symptomatic
| System | Manifestation |
|---|---|
| Skeletal | Bone pain, fractures, osteoporosis, osteitis fibrosa cystica, subperiosteal resorption, brown tumours |
| Renal | Nephrolithiasis (calcium oxalate/phosphate), nephrocalcinosis, polyuria, polydipsia, renal insufficiency |
| GI | Nausea, vomiting, constipation, peptic ulcers (gastrin stimulation), pancreatitis |
| Neuromuscular | Muscle weakness, fatigue, depression, cognitive changes |
| Cardiovascular | Hypertension, arrhythmias |
- Robbins Pathologic Basis of Disease, p. 1012
- Schwartz's Principles of Surgery, p. 1667
Biochemical Diagnosis
| Test | Finding |
|---|---|
| Serum calcium | Elevated (hypercalcaemia) |
| PTH | Elevated or inappropriately normal (key: PTH should be low in hypercalcaemia from other causes) |
| Serum phosphate | Decreased (hypophosphataemia) |
| Chloride:phosphate ratio | Increased (>33) |
| Urinary calcium | Increased (helps exclude FHH - familial hypocalciuric hypercalcaemia, where urine calcium is low) |
| Urinary cAMP | Increased |
| Serum ALP | Elevated if bone disease present |
Localization Imaging
| Modality | Notes |
|---|---|
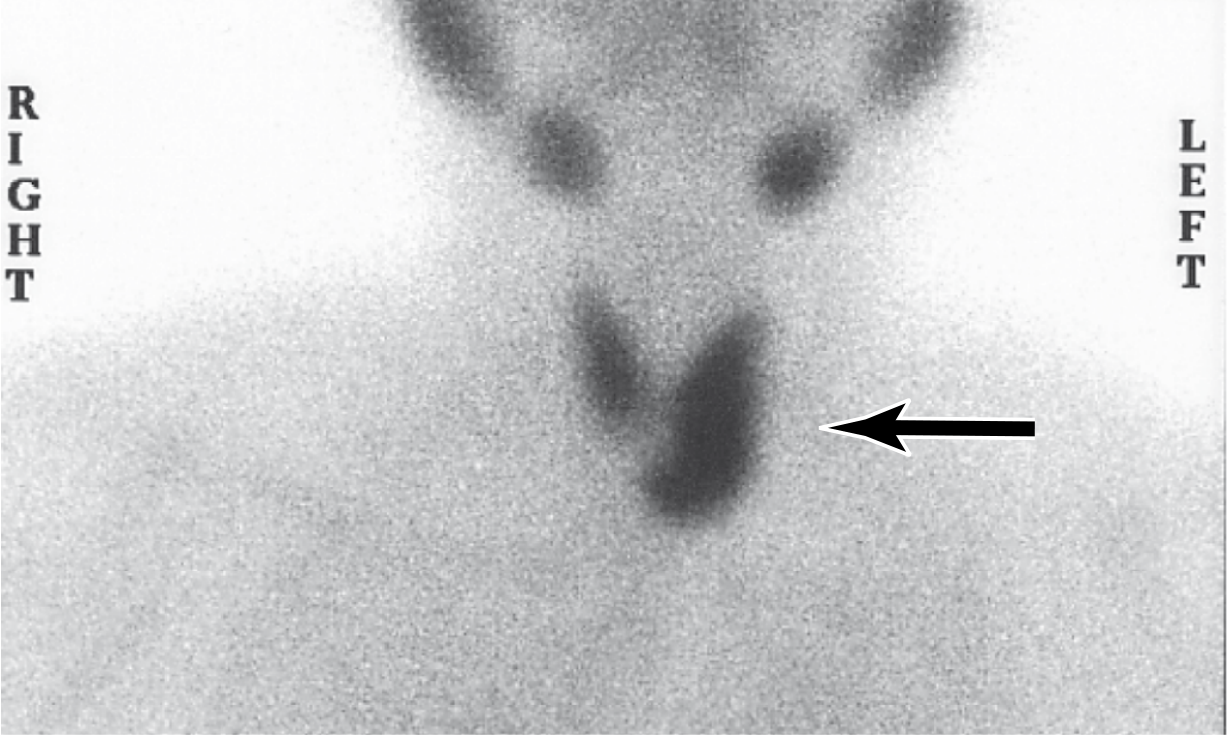
| Technetium-99m sestamibi scan | First-line; identifies single adenoma well; reduced accuracy for multiglandular disease |
| Neck ultrasound | Complements sestamibi; together give ~95% accuracy if both identify the same gland |
| 4D-CT | Useful in re-operative cases |
| MRI | Used for ectopic/mediastinal adenomas |
Treatment
Surgery (definitive)
- Minimally invasive parathyroidectomy (MIP): Focused unilateral exploration guided by preoperative localization studies. Suitable when both sestamibi and ultrasound concordantly identify the same gland (~95% success).
- Bilateral neck exploration: Standard when localization fails, multiglandular disease is suspected, or IOPTH is unavailable.
- Intraoperative PTH monitoring (IOPTH): PTH has a 3-5 minute half-life; a >50% drop from baseline at 10 minutes confirms curative resection (the Miami criterion).
- Radio-guided parathyroidectomy: Uses pre-injected Tc-99m sestamibi and a handheld gamma probe; rarely used now as it offers little advantage over preoperative scanning.
Non-surgical management (for asymptomatic, ineligible patients)
-
Adequate hydration, avoid thiazides and immobilization
-
Cinacalcet (calcimimetic): Reduces serum calcium by increasing sensitivity of the CaSR to extracellular calcium; does not improve bone density
-
Bisphosphonates: Improve bone density
-
Schwartz's Principles of Surgery, p. 1670-1701
-
Scott-Brown's Otorhinolaryngology, p. 2086
Familial Associations
| Syndrome | Gene | Features |
|---|---|---|
| MEN-1 | MEN1 (11q13) | Parathyroid + pituitary + pancreatic tumours |
| MEN-2A | RET | Parathyroid + MTC + phaeochromocytoma |
| MEN-4 | CDKN1B | MEN-1-like, RET-negative |
| HPT-JT syndrome | CDC73 | Parathyroid carcinoma + ossifying jaw tumours |
| FHH | CASR | Hypocalciuric hypercalcaemia; no surgery benefit |
Recent Evidence (2024-2026)
- A 2024 systematic review in JCEM (PMID 38739762) confirms that parathyroidectomy has a significant positive skeletal effect in PHPT patients.
- A 2026 meta-analysis in ANZ J Surg (PMID 41721481) shows minimally invasive parathyroidectomy under locoregional anaesthesia is a safe and effective alternative to general anaesthesia.
Varicose vein, pre and clinical with management from cpg , investigations 101
"varicose veins" AND "clinical practice guideline"
varicose veins CPG clinical practice guideline 2023 2024 management NICE SVS
https://www.nice.org.uk/guidance/CG168
SVS AVF 2022 2023 varicose veins guidelines CEAP classification recommendations duplex endovenous ablation
https://emedicine.medscape.com/article/462579-guidelines
Varicose Veins - Complete Clinical Overview
Definition
- Telangiectasias / spider veins (C1): intradermal dilated vessels <1 mm
- Reticular veins (C1): dilated blue subdermal veins 1-3 mm
Epidemiology & Risk Factors
- Adult prevalence of visible varicose veins: 30-50%
- More common in women; increases markedly with age (Edinburgh Vein Study: 11.5% at 18-24 years up to 55.7% at 55-64 years)
| Factor | Detail |
|---|---|
| Gender | More common in women |
| Age | Prevalence rises with age |
| Pregnancy | Progesterone relaxes vein walls; increased pelvic pressure |
| Family history | Strong familial susceptibility (genetic predisposition to connective tissue weakness) |
| Obesity | Raised intra-abdominal pressure |
| Prolonged standing | Occupational risk (inconclusive evidence) |
| Deep vein thrombosis (DVT) | Leads to secondary varicose veins |
| Pelvic masses | Obstruct venous return |
- Bailey and Love's Short Practice of Surgery, 28th Ed, p. 1051
Classification
1. Primary vs Secondary
| Type | Cause |
|---|---|
| Primary | Intrinsic weakness of venous wall / valve leaflets - no identifiable cause |
| Secondary | DVT (post-thrombotic syndrome), pelvic obstruction, AV fistula, pregnancy |
2. CEAP Classification (2020 Updated)
| Class | Description |
|---|---|
| C0 | No visible or palpable signs of venous disease |
| C1 | Telangiectasias or reticular veins |
| C2 | Varicose veins (≥3 mm diameter) |
| C2r | Recurrent varicose veins |
| C3 | Oedema (venous origin, daily occurrence) |
| C4a | Pigmentation or eczema |
| C4b | Lipodermatosclerosis or atrophie blanche |
| C4c | Corona phlebectatica |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
| C6r | Recurrent active venous ulcer |
Pathophysiology
- Valvular incompetence - valve leaflets fail to coapt, allowing reflux
- Primary wall weakness - defective connective tissue (reduced collagen/elastin ratio) causes vein dilatation, which stretches and separates valve cusps
- Calf muscle pump failure - ineffective muscle contraction fails to propel blood centrally
- Perforator incompetence - bidirectional flow in perforators allows high-pressure deep system blood to enter low-pressure superficial system
- Great Saphenous Vein (GSV) joins the femoral vein at the Saphenofemoral Junction (SFJ) in the groin - responsible for ~60% of varicose veins (medial thigh and calf distribution)
- Small Saphenous Vein (SSV) joins the popliteal vein at the Saphenopopliteal Junction (SPJ) - responsible for ~20% (posterolateral calf)
- Anterior Accessory GSV (AAGSV) - anterolateral thigh/calf distribution
- Fitzpatrick's Dermatology, p. 2185; Bailey and Love, p. 1052
Clinical Features
Presenting Symptoms (Subjective)
- Aching, heaviness, throbbing, burning, bursting sensation in affected leg
- Itching over varicosities
- Ankle swelling (oedema), especially in the evening
- All symptoms worsen with prolonged standing and are relieved by elevation and compression
- Cosmetic concern (most common complaint)
- Symptoms may be disproportionate to the severity of visible veins - a trial of compression helps confirm venous aetiology
Signs (Objective)
- Tortuous, dilated subcutaneous veins - visible and palpable
- Saphena varix - large dilated veins at SFJ, presents as a soft groin lump disappearing on lying (can mimic inguinal hernia; has a cough impulse)
- Oedema of ankle (pitting - venous)
- Haemosiderin pigmentation (brown staining) at medial gaiter area
- Venous eczema / stasis dermatitis - dry, scaly, itchy skin
- Lipodermatosclerosis - woody induration and fibrosis of the skin
- Atrophie blanche - white, scarred plaques
- Varicose (venous) ulcer - typically medial gaiter area (over medial malleolus), shallow, sloping edges, granulating base, painful
Complications
| Acute | Chronic |
|---|---|
| Thrombophlebitis (superficial vein thrombosis) | Venous eczema |
| Haemorrhage (spontaneous or traumatic) | Lipodermatosclerosis |
| - | Venous ulcer |
| - | Hyperpigmentation |
| - | Infection/cellulitis |
Clinical Tests (Bedside Examination)
Note: Tourniquet tests (Trendelenburg/Perthes) and handheld Doppler are now largely abandoned in favour of duplex ultrasound, which provides definitive anatomical and physiological information.
| Test | What it assessed | Status |
|---|---|---|
| Trendelenburg test | Level of valvular incompetence | Superseded |
| Perthes' test | Deep vein patency | Superseded |
| Handheld Doppler | Reflux at SFJ/SPJ | Superseded |
| Duplex ultrasound | Full venous mapping | Current gold standard |
- Bailey and Love, p. 1052
Investigations
1. Duplex Ultrasound Scan (DUS) - MANDATORY before any intervention
- Confirm reflux in the deep and superficial venous systems
- Define the exact distribution and extent of reflux and affected junctions (SFJ, SPJ, perforators)
- Assess deep vein patency (exclude obstruction/DVT)
- Assess suitability for treatment (diameter, extent, tortuosity)
- Detect thrombus within superficial veins
- Identify pelvic source of reflux
- High-frequency linear array transducer: 7.5-13 MHz
- Patient examined standing for diameter/reflux measurements
- Reflux definition: retrograde flow lasting ≥0.5 seconds (superficial/perforator veins) or ≥1 second (proximal deep veins)
- Elicited by calf/foot squeeze release, manual compression, or Valsalva
2. Other Investigations (Selected Cases)
| Investigation | Indication |
|---|---|
| Venous duplex (full leg) | All patients before intervention (CPG) |
| CT venography / MRI venography | Suspected pelvic source (May-Thurner, pelvic varicosities), suspected DVT extension |
| Ascending phlebography (venography) | Pre-deep vein reconstruction; rarely needed now |
| Descending venography | Deep valve incompetence assessment before valve reconstruction (highly specialised) |
| Abdominal USS / CT abdomen | Suspected secondary cause (pelvic mass, IVC obstruction) |
| ABI (Ankle-Brachial Index) | Mandatory before prescribing compression - to exclude peripheral arterial disease (PAD); ABI <0.8 = compression contraindicated |
| D-dimer + Doppler | If concurrent DVT/SVT suspected |
| Blood tests (FBC, coagulation) | Pre-operative work-up |
- Bailey and Love, p. 1052; Schwartz's Surgery, p. 1670
Management
Framework (SVS/AVF/AVLS 2022/2023 CPG + NICE CG168)
Step 1 - Conservative Management
- British Classification: Class 1 (14-17 mmHg), Class 2 (18-24 mmHg), Class 3 (25-35 mmHg)
- Improves symptoms but does NOT prevent progression or occurrence
- Compliance is universally poor
- CPG (NICE/SVS): Compression is an adjunct, NOT a substitute for definitive treatment; interventional treatment is superior and cost-effective
- ABI must be checked before prescribing; contraindicated if ABI <0.8
- Leg elevation
- Weight loss
- Exercise / calf muscle pump activation
- Avoid prolonged standing
Step 2 - Interventional Treatment (for symptomatic C2-C6)
A. Endothermal Ablation - First-line treatment (CPG Grade 1A)
| Technique | Details |
|---|---|
| Endovenous Laser Ablation (EVLA) | Wavelength typically 1470 nm; laser fibre inserted into vein; bare tip or radial firing designs available; very high technical efficacy |
| Radiofrequency Ablation (RFA) | Radiofrequency energy; ClosureFAST catheter most used; equally effective to EVLA; less post-procedure pain and bruising in some studies |
- Both are equivalent in efficacy; associated with faster recovery and less morbidity than open surgery
- Bailey and Love, p. 1051-1058; Schwartz's Surgery, p. 1671
B. Non-Thermal, Non-Tumescent (NTNT) Ablation
| Technique | Details |
|---|---|
| Ultrasound-Guided Foam Sclerotherapy (UGFS) | Sclerosant (sodium tetradecyl sulphate) converted to foam (Tessari method: 1:3 or 1:4 sclerosant:air); foam maximises endothelial contact; performed under US guidance; lower efficacy than thermal ablation but suitable for recurrent/residual veins |
| Cyanoacrylate glue (VenaSeal) | Medical-grade adhesive injected into vein; no tumescent needed; no thermal injury; promising results |
| Mechanochemical ablation (MOCA - ClariVein) | Rotating wire causes mechanical endothelial injury + simultaneous sclerosant infusion; no heat or tumescent needed |
C. Open Surgical Treatment (still used, less commonly)
- Oblique groin incision at pubic tubercle level
- Dissect and ligate SFJ (flush ligation with all six tributaries)
- GSV stripped retrogradely to the knee (not ankle - reduces saphenous nerve injury risk)
- Followed by phlebectomy of residual varicosities
-
Popliteal fossa incision at skin crease
-
Duplex marking of SPJ essential pre-operatively (very variable anatomy)
-
SSV can be ligated or stripped; risk of sural nerve injury with stripping
-
Bailey and Love, p. 1052-1658
D. Phlebectomy (Ambulatory / Stab Phlebectomy)
- Removal of varicose tributaries through multiple small (2-3 mm) stab incisions using phlebectomy hooks
- Performed as sole treatment (isolated tributary incompetence) or concurrently with truncal ablation
- Concomitant phlebectomy gives more rapid QOL improvement and allows single-visit treatment
- Superior to powered transilluminated phlebectomy for bruising and pain
E. Sclerotherapy (Liquid / Foam)
- Sclerosing agents: sodium tetradecyl sulphate (STS), polidocanol, hypertonic saline
- Liquid sclerotherapy for telangiectasias/reticular veins (C1)
- Foam sclerotherapy for larger varicosities and truncal veins
- Compression bandaging applied post-procedure for 3-5 days, then stockings for 2 weeks
- Complications: pigmentation, thrombophlebitis, DVT, skin necrosis, allergic reaction, visual disturbance (rare, with foam)
CPG Summary Table (SVS/AVF/AVLS 2022/2023 - Key Recommendations)
| Recommendation | Grade |
|---|---|
| Duplex ultrasound scanning before any intervention | Strong (1A) |
| Endovenous thermal ablation (EVLA/RFA) as first-line over open surgery for GSV/SSV reflux | Strong (1A) |
| UGFS as an alternative when thermal ablation not suitable | Conditional (2B) |
| Compression therapy for symptom relief as adjunct | Conditional |
| Compression alone NOT preferred over intervention for symptomatic patients | Strong |
| Treat truncal reflux + varicose tributaries in same session (if possible) | Consensus |
| Perforator vein treatment in mild-moderate disease: limited role | Consensus |
| ABI before compression prescription | Best Practice |
Special Situations
| Situation | Action |
|---|---|
| Thrombophlebitis (SVT) | NSAIDs, compression; exclude DVT with duplex; anticoagulate if propagating towards SFJ (<5 cm from SFJ = high risk DVT) |
| Haemorrhage from varicose vein | Elevate limb, apply pressure; firm compression bandaging; arrange urgent intervention |
| Venous ulcer (C6) | Compression (4-layer bandaging), wound care, debridement; ablate superficial reflux to aid healing; consider skin grafting for large ulcers |
| Pregnancy | Conservative (elevation, compression stockings); defer intervention until 3+ months post-partum |
| Recurrent varicose veins | Repeat duplex; UGFS or re-do endovenous ablation preferred over re-do open surgery |
Surgical Complications
| Complication | Incidence |
|---|---|
| Wound infection | Most common; reduced by prophylactic antibiotics |
| Saphenous nerve neuralgia (GSV stripping to knee) | Up to 7% |
| Sural nerve neuropraxia (SSV surgery) | Up to 20% |
| Common peroneal nerve injury (SSV surgery) | Up to 4% |
| DVT / PE | ~0.5% |
| Recurrence at 5-10 years | 20-30% |
- Bailey and Love's Short Practice of Surgery, 28th Ed - Chapter 62 (Varicose Veins), pp. 1050-1058
- Schwartz's Principles of Surgery, 11th Ed - Chapter 23, pp. 1669-1672
- Mulholland & Greenfield's Surgery, 7th Ed - Chapter on Chronic Venous Insufficiency
- SVS/AVF/AVLS CPG Part I (Gloviczki et al., J Vasc Surg Venous Lymphat Disord 2023;11:231-261) - Duplex & Truncal Reflux Treatment
- SVS/AVF/AVLS CPG Part II (Gloviczki et al., J Vasc Surg Venous Lymphat Disord 2024;12:101670) - Compression, Tributaries & Complications
- NICE CG168 - Varicose veins: diagnosis and management (2013, reviewed 2016)
Presentation: Clinical Features of Intestinal Obstruction + Neonatal Causes - Hema Cardinal features: History: Pain, vomiting, distension, constipation Examination: Distension, bowel sounds, dehydration Acute intestinal obstruction in newborn: Intestinal atresia Meconium ileus Meckel’s diverticulum Foreign body
Clinical Features of Intestinal Obstruction + Neonatal Causes
PART 1 - ACUTE INTESTINAL OBSTRUCTION: Clinical Features
Definition & Types
| Type | Description |
|---|---|
| Mechanical | Physical blockage - intraluminal, intramural, or extraluminal |
| Paralytic (Adynamic/Ileus) | Failure of peristalsis without mechanical cause |
| Strangulating | Blood supply compromised - surgical emergency |
| Simple | Blood supply intact |
Cardinal Clinical Features (The "Big Four")
"Pain, Vomiting, Distension, Absolute Constipation"
HISTORY
1. Abdominal Pain
- First and most prominent symptom - occurs suddenly and is usually severe
- Character: Colicky (intermittent, wave-like) - coincides with peristaltic contractions
- Proximal (jejunum/high ileum): Colic in waves every 3-5 minutes, lasting ~30 seconds; centred at the umbilicus/epigastrium; vomiting often terminates the pain
- Distal (terminal ileum): Longer intervals between cramps, 8-10 minutes; more distension, less vomiting
- Colonic obstruction: Pain in the lower abdomen (hypogastrium)
- With increasing distension: colicky pain becomes constant, diffuse aching
- Severe unrelenting pain = strangulation until proven otherwise; beware the patient whose pain is not controlled with IV opiates
2. Vomiting
- The more proximal the obstruction, the earlier and more frequent the vomiting
- Character changes with time:
- Early: Ingested food/gastric contents
- Intermediate: Bilious (bile-stained, duodenal content)
- Late (days): Faeculent vomiting - grave sign (bacterial overgrowth of intestinal content; takes ~3-4 days in complete obstruction)
- In high duodenal/proximal small bowel obstruction: vomiting is early, profuse, relieves pain
- In low/colonic obstruction: vomiting is late, distension is pronounced
- Bilious vomiting in a neonate = mechanical obstruction until proven otherwise
3. Distension
- Depends on site and duration of obstruction
- Small bowel (proximal): Less distension, central (umbilical)
- Small bowel (distal): Pronounced central distension
- Large bowel: Peripheral (flank) distension, appears later
- Visible peristalsis: Pathognomonic when present; can be provoked by gently flicking the abdominal wall; seen in thin patients
- Volvulus: Regional distension
4. Absolute Constipation
- Defined as failure to pass both faeces AND flatus - absolute feature of complete obstruction
- Important caveat: Takes at least 24 hours to develop as a sign; early cases may still pass stool evacuated from below the obstruction
- Diarrhoea may occur instead of constipation in:
- Mesenteric vascular occlusion
- Richter's hernia
- Pelvic abscess with adhesion obstruction
- Partial obstruction
EXAMINATION
A. Inspection
| Finding | Significance |
|---|---|
| Abdominal distension | Central (small bowel), peripheral (large bowel), regional (volvulus) |
| Visible peristalsis | Diagnostic of mechanical obstruction |
| Scars | Previous surgery - adhesions |
| Hernial orifices | MUST always be examined - strangulated hernia is a common cause |
| Skin changes (erythema, purplish discoloration) | Underlying ischaemia of strangulated hernia |
B. Palpation
- Muscle guarding: Conspicuously absent in simple obstruction (differentiates from peritonitis)
- Local tenderness: Impending or established ischaemia
- Localised tenderness over surgical scar: Adhesion obstruction
- Generalised tenderness + rigidity: Indicates need for early laparotomy (perforation/infarction)
- Shock (tachycardia, hypotension): Suggests strangulation/ischaemia
C. Bowel Sounds
- High-pitched tinkling rushes: Classic of mechanical obstruction; coincide with colic, may precede vomiting
- Normal bowel sounds: Negative predictive value (do NOT exclude obstruction)
- Scanty or absent: Long-standing obstruction; bowel has become inactive
- Ominously quiet bowel: Strangulation/peritonitis developing - bowel becomes atonic
D. Dehydration
- Seen predominantly in small bowel obstruction (repeated vomiting + fluid sequestration into obstructed loops)
- Up to 6 litres/day of salt-rich fluid secreted into small intestine normally; in obstruction, this accumulates
- Signs: dry mucous membranes, sunken eyes, poor venous filling, oliguria, tachycardia
- Labs: raised urea, raised haematocrit, electrolyte disturbance
E. Other Findings
| Sign | Significance |
|---|---|
| Pyrexia | Onset of ischaemia, perforation, or inflammatory cause |
| Hypothermia | Septicaemic shock, neglected cases |
| Hypokalaemia | Common in small bowel obstruction with vomiting |
| Raised WBC (neutrophilia) | Intestinal infarction; rising WBC warns of developing ischaemia |
| Raised serum amylase | Moderately elevated in strangulation/infarction |
Features Distinguishing Simple vs Strangulating Obstruction
| Feature | Simple | Strangulating |
|---|---|---|
| Pain | Colicky, intermittent | Continuous, severe |
| Tenderness | Absent/mild | Present, localised then generalised |
| Pulse | Normal | Tachycardia/shock |
| Temperature | Normal | Raised (or hypothermia = late) |
| WBC | Normal/mildly elevated | Marked leukocytosis |
| Peritonism | Absent | Present - indicates infarction |
PART 2 - NEONATAL INTESTINAL OBSTRUCTION: Classification & Clinical Features
General Features of Obstruction in the Newborn
- Bilious vomiting in a neonate = mechanical intestinal obstruction until proven otherwise
- Non-bilious persistent vomiting may indicate: gastro-oesophageal reflux, pyloric stenosis, or high duodenal (pre-ampullary) obstruction
- Additional features:
- Abdominal distension (degree directly related to level of lesion)
- Failure to pass meconium (98% of full-term infants pass meconium within 24 hours)
- Hyperactive bowel sounds
- Distension confined to upper abdomen = high (duodenal/jejunal) obstruction
- Massive distension (may cause respiratory embarrassment) = lower level
- Erythema/oedema of anterior abdominal wall = peritonitis (perforation or ischaemia)
Classification of Neonatal Intestinal Obstruction
| Level | Causes |
|---|---|
| Intraluminal | Meconium ileus, milk inspissation, meconium plug syndrome |
| Intramural | Intestinal atresia/stenosis, Hirschsprung's disease, anorectal malformations |
| Extrinsic | Malrotation ± volvulus, irreducible inguinal hernia, intussusception, duplication cysts |
1. INTESTINAL ATRESIA
Definition
Incidence
Aetiology
Sites (frequency order)
- Duodenal atresia - most common form of neonatal intestinal obstruction; associated with Down syndrome (trisomy 21) in 30%
- Jejunal atresia - second most common
- Ileal atresia
- Colonic atresia - rare
Types (Grosfeld Classification)
| Type | Description |
|---|---|
| Type I | Mucosal web/membrane - muscular wall intact; continuity preserved |
| Type II | Blind-ending segments connected by a fibrous cord |
| Type IIIa | Blind ends separated by a V-shaped mesenteric defect |
| Type IIIb | "Apple-peel" / "Christmas tree" - distal bowel receives retrograde blood supply from ileocolic/right colic artery; proximal obstruction + coiled distal ileum |
| Type IV | Multiple atresias - "string of sausages/beads" |

Clinical Features
- Bilious vomiting - dominant in jejunal atresia (onset within hours of birth)
- Abdominal distension - more prominent in ileal atresia (lower level)
- Failure to pass normal meconium - small amounts of pale meconium may be passed even with complete atresia
- Possible antenatal history of polyhydramnios (failure to swallow amniotic fluid)
- Associated malformations common (assess whole bowel intraoperatively for multiple atresias)
Investigations
- Plain abdominal X-ray (supine + erect): Variable number of dilated loops with air-fluid levels; number of dilated loops reflects level of obstruction
- "Double bubble" sign (duodenal atresia): Gas in stomach + duodenum; no distal bowel gas
- Contrast enema: In stable infants for distal obstructions; identifies microcolon (distal ileal atresia), meconium plug, Hirschsprung's, or meconium ileus
Management
- Resuscitate with IV fluids, NGT decompression
- Duodenal atresia: Duodenoduodenostomy
- Jejunal/ileal atresia: Resection of dilated proximal segment (poor motility) + primary end-to-end anastomosis (end-to-back "fish-mouth" technique for disparity in lumen size)
- Tapering of proximal bowel if extremely dilated
- Temporary stoma if primary anastomosis not safe (unstable infant, ischaemia)
2. MECONIUM ILEUS
Definition
Pathophysiology
- Cystic fibrosis (autosomal recessive, CFTR gene mutation) causes:
- Pancreatic enzyme deficiency → meconium not liquefied
- Abnormal chloride secretion → dehydrated, viscous intestinal contents
- Thick meconium becomes impacted in terminal ileum → progressive intestinal obstruction
Types
| Type | Features |
|---|---|
| Uncomplicated | No perforation; impacted meconium only |
| Complicated | Prenatal perforation, volvulus, atresia, or vascular compromise |
Clinical Features
- Presents shortly after birth
- Progressive abdominal distension - visibly dilated loops of bowel often palpable
- Failure to pass meconium
- Bilious vomiting (intermittent)
- Family history of CF may be present (autosomal recessive)
Investigations
- Plain X-ray: Dilated loops of small intestine; characteristic "ground glass" appearance (gas bubbles trapped in inspissated meconium in distal ileum); no air-fluid levels (meconium too viscous to separate from gas)
- Contrast enema: Shows microcolon (unused, underdeveloped colon); terminal ileum filled with meconium pellets; in uncomplicated cases, no abrupt termination of gas
- Gene mutation analysis (CFTR)
- Sweat test (beyond neonatal period): elevated sodium and chloride levels >70 mmol/L
- In complicated cases: eggshell calcifications on X-ray (intraperitoneal calcification from meconium peritonitis)
Management
- Hyperosmolar Gastrografin enema (water-soluble contrast): Draws fluid into gut lumen + detergent properties liquefy meconium; may be repeated at 12-hourly intervals
- N-acetylcysteine (Mucomyst) enema: Alternative/adjunct
- Patient requires extra IV fluids to compensate for fluid shifts
- If contrast cannot be refluxed into dilated ileum: suggests associated atresia → laparotomy
- Laparotomy + enterotomy + bowel irrigation
- Resection + primary anastomosis
- Resection + end ileostomy + mucus fistula
- Bishop-Koop anastomosis (end-to-side ileoileostomy with irrigating stoma - now rarely used)
- CF management long-term: pancreatic enzyme replacement, physiotherapy, nutritional support
3. MECKEL'S DIVERTICULUM
Definition
The "Rule of 2's"
| Fact | Detail |
|---|---|
| 2% of the population | |
| Within 2 feet (60 cm) of ileocaecal valve | |
| ~2 inches (5 cm) long | |
| 2:1 male:female ratio | |
| Symptomatic by age 2 | |
| Only ~2-4% are ever symptomatic |
Ectopic Tissue
- Present in ~50% of cases
- Gastric mucosa (80-85% of ectopic tissue) → acid secretion → peptic ulceration of adjacent ileal mucosa
- Also: pancreatic tissue, duodenal mucosa
Clinical Presentations (Complications)
| Complication | Features |
|---|---|
| Haemorrhage | Most common; painless dark rectal bleeding / melaena (maroon stool); peptic ulceration by ectopic gastric mucosa; may be massive |
| Intestinal obstruction | Second most common: (a) intussusception - Meckel's as lead point (most common cause of intussusception in children >4 years); (b) volvulus around a persistent fibrous band/vitelline cord; bilious vomiting + distension |
| Diverticulitis | Presents like appendicitis; diagnosis usually at laparotomy; perforation in ~1/3 |
| Littre's hernia | Meckel's diverticulum found in inguinal or femoral hernia sac |
Investigations
- Meckel's scan (Tc-99m pertechnetate scintigraphy): Investigation of choice for bleeding; ectopic gastric mucosa takes up isotope; sensitivity ~85% in children
- Plain X-ray: Usually unhelpful; occasionally dilated bowel loops with air-fluid levels within the diverticulum
- CT scan: May show tubular blind-ending structure from antimesenteric border of terminal ileum; CT enterography has improved detection
- Barium contrast studies: Generally unhelpful
Management
- Symptomatic Meckel's: Diverticulectomy or segmental small bowel resection + anastomosis (preferred if base is wide, inflamed, or contains ectopic tissue)
- Do NOT amputate at base and invaginate (risk of stricture, leaving ectopic tissue)
- Incidental finding at surgery: Leave if wide-mouthed and not thickened; remove if in doubt
4. FOREIGN BODY
Mechanisms of Obstruction
- Direct luminal obstruction: Large or irregularly shaped foreign body (e.g., ingested toy part, bezoar)
- Obstruction is most common at anatomical narrowings: pylorus, terminal ileum, ileocaecal junction
- In neonates: rare; more often iatrogenic (feeding tube, calcified meconium fragments)
- Gallstone ileus: Erosion of gallstone from gallbladder into intestine → obstruction of terminal ileum; gas in biliary tree on X-ray (Rigler's triad: pneumobilia + small bowel obstruction + ectopic gallstone)
- Bezoar: Phytobezoar (vegetable matter) or lactobezoar (milk) in neonates/infants
Clinical Features
- Symptoms of small bowel obstruction (pain, vomiting, distension, constipation)
- Foreign body may be visible on plain X-ray if radio-opaque
Management
- Plain X-ray first: identifies radio-opaque foreign bodies
- CT abdomen: Identifies level and nature of obstruction; gas in biliary tree if gallstone ileus
- Endoscopic retrieval if in accessible location
- Surgical removal if causing complete obstruction/perforation
SUMMARY TABLE: Neonatal Causes Compared
| Feature | Intestinal Atresia | Meconium Ileus | Meckel's Diverticulum | Foreign Body |
|---|---|---|---|---|
| Timing | Hours after birth | Shortly after birth | Any age (usually <2y) | Any age |
| Vomiting | Bilious (early) | Bilious (intermittent) | Bilious (if obstruction) | Bilious |
| Distension | Yes (degree by level) | Yes (dilated loops palpable) | Variable | Variable |
| Meconium | Absent / pale | Absent | Normal initially | Normal |
| Key X-ray | Air-fluid levels, dilated loops | Ground glass, no fluid levels, microcolon on enema | Usually normal | FB visible if radio-opaque |
| Key investigation | Contrast enema | Contrast enema (Gastrografin) + CFTR gene analysis | Tc-99m scan (if bleeding) | Plain X-ray / CT |
| Association | Down syndrome (duodenal) | Cystic fibrosis (100%) | Ectopic gastric mucosa | None specific |
| Management | Surgery (primary anastomosis) | Gastrografin enema → surgery if failed | Diverticulectomy | Endoscopy / surgery |
- Bailey & Love's Short Practice of Surgery, 28th Ed, Ch. 78 - pp. 1399-1410
- Schwartz's Principles of Surgery, 11th Ed, Ch. 39 - pp. 1752-1755
- Pye's Surgical Handicraft, 22nd Ed, Ch. 27 - pp. 408-410
- S. Das - Manual on Clinical Surgery, 13th Ed, pp. 479-481
- Robbins & Kumar Basic Pathology - p. 561
- Robbins, Cotran & Kumar Pathologic Basis of Disease - pp. 1490-1503
- Sleisenger & Fordtran's GI and Liver Disease - pp. 1396-1420
Dr Rashide's questions (week 3) 1. Read about *pancreatitis* , liver segments, IBD, Colorectal CA 2. Liver pathologies (CA, abscess, hepatitis) 3. Complications of pancreatitis: Hypovolemic shock, septic SIRS, DIVC, bleeding, perforation
Dr. Rashide's Week 3 - Complete Study Notes
TOPIC 1 - PANCREATITIS
Definition
Aetiology ("GET SMASHED")
| Cause | Details |
|---|---|
| Gallstones | 50-70% of cases - most common; passage of stones obstructs common channel → bile reflux |
| Ethanol (Alcohol) | 25% of cases; direct toxicity, hypersecretion, duct obstruction |
| Trauma | Blunt abdominal trauma |
| Steroids | Corticosteroids |
| Mumps / viruses | Coxsackievirus, EBV, mumps |
| Autoimmune | IgG4-related disease |
| Scorpion sting | Rare |
| Hypercalcaemia / Hyperlipidaemia | Check calcium and fasting lipids in idiopathic cases |
| ERCP | 1-3% post-ERCP pancreatitis |
| Drugs | Corticosteroids, azathioprine, asparaginase, valproic acid, thiazides, oestrogens |
| Hereditary | Mutations in cationic trypsinogen gene (PRSS1); teens onset, high risk of pancreatic CA by age 70 |
| Idiopathic | <20% of cases after thorough investigation |
Pathophysiology
- Obstruction/injury → premature activation of trypsinogen → trypsin within acinar cells
- Trypsin activates other zymogens (phospholipase A2, elastase, lipase)
- Autodigestion → pancreatic oedema, haemorrhage, fat necrosis, parenchymal necrosis
- Release of inflammatory mediators (cytokines, bradykinin, PAF) → systemic effects: SIRS → MODS
Clinical Presentation (Bailey & Love)
Symptoms
- Pain: Cardinal symptom - epigastric, sudden onset reaching maximum within minutes (not hours), severe, constant, lasts hours to days; radiates to back in 50%; relieved by leaning forward; does NOT improve with vomiting
- Nausea and vomiting: Marked, persistent retching; vomiting does not relieve pain (unlike peptic ulcer)
- Hiccoughs: Due to gastric distension or diaphragmatic irritation
Signs
| Sign | Detail |
|---|---|
| Tachycardia, tachypnoea | Common |
| Hypotension | May be present - indicates shock |
| Fever | Often initially normal/subnormal; rises as inflammation develops |
| Jaundice | Mild; biliary obstruction in gallstone pancreatitis |
| Grey Turner's sign | Bluish discoloration of flanks (retroperitoneal haemorrhage) |
| Cullen's sign | Bluish discoloration of periumbilical region |
| Abdominal guarding | Upper abdomen; rigidity unusual |
| Mass in epigastrium | Inflammatory phlegmon or pseudocyst |
| Pleural effusion | Present in 10-20%; typically left-sided |
| Subcutaneous fat necrosis | Small red tender nodules on legs (enzymatic fat necrosis) |
Investigations
- Is the diagnosis correct?
- How severe is the attack?
- What is the aetiology?
| Investigation | Finding / Purpose |
|---|---|
| Serum amylase | >3× upper limit of normal = diagnostic; may be normal if delayed presentation or in hyperlipidaemia (spuriously low) |
| Serum lipase | More sensitive and specific than amylase; remains elevated longer |
| FBC | Leukocytosis; haematocrit elevation indicates haemoconcentration |
| U&E | Urea elevation (dehydration); monitor renal function |
| LFTs / Bilirubin | Biliary aetiology; jaundice |
| Serum calcium | Hypocalcaemia (saponification of fat by lipase) = marker of severity; also exclude hypercalcaemia as cause |
| Blood glucose | Hyperglycaemia = severity marker |
| LDH | Elevation = severity marker |
| CRP | >150 mg/L at 48 hours = severe attack indicator |
| ABGs | Hypoxaemia; pO₂ <60 mmHg = severity marker; ARDS |
| USS abdomen | First-line for gallstones; limited for pancreas (bowel gas) |
| CT abdomen with contrast | Best single imaging investigation for severity and necrosis assessment; CT Severity Index (CTSI); done at 48-72 hours |
| MRCP | Non-invasive ductal imaging; evaluate for choledocholithiasis |
| ERCP | Therapeutic: gallstone pancreatitis with cholangitis/jaundice/dilated CBD within 72 hours |
| Chest X-ray | Pleural effusion, pneumonia, ARDS |
Severity Scoring (Revised Atlanta Classification 2013)
| Category | Criteria |
|---|---|
| Mild AP | No organ failure; no local or systemic complications |
| Moderately Severe AP | Transient organ failure (<48h); and/or local/systemic complications without persistent organ failure |
| Severe AP | Persistent organ failure (>48h); single or multiple organ failure |
- Mild AP: 80-90% of cases; mortality ~1%
- Severe AP: 5-10% of cases; mortality 20-50%
Ranson & Glasgow Scoring (Score ≥3 = Severe)
| Ranson (on admission) | Glasgow (within 48h) |
|---|---|
| Age >55 years | Age >55 years |
| WBC >16 × 10⁹/L | WBC >15 × 10⁹/L |
| Blood glucose >11 mmol/L | Blood glucose >10 mmol/L (no DM) |
| LDH >350 units/L | LDH >600 units/L or AST >200 units/L |
| AST >250 units/L | Albumin <32 g/L |
| At 48h (Ranson): | Urea >16 mmol/L |
| Base deficit >4 mEq/L | Calcium <2 mmol/L |
| Haematocrit fall >10% | pO₂ <60 mmHg |
| Urea rise >1.8 mmol/L | |
| Serum calcium <2 mmol/L | |
| pO₂ <60 mmHg | |
| Fluid sequestration >6L |
TOPIC 2 - COMPLICATIONS OF PANCREATITIS
Systemic Complications (First Week)
1. Hypovolaemic Shock
- Massive third-space fluid loss into retroperitoneum and peritoneal cavity (up to 6-8L)
- Vomiting and nasogastric losses
- Vasodilation from inflammatory mediators (bradykinin, PAF)
- Haemorrhage from erosion of peripancreatic vessels
- Result: reduced circulating volume → decreased cardiac output → shock
2. Septic SIRS (Systemic Inflammatory Response Syndrome)
- Heart rate >90/min
- Core temperature <36°C or >38°C
- Respirations >20/min or pCO₂ <32 mmHg
- WBC <4000 or >12,000/mm³
- Early SIRS = sterile inflammatory mediator release (cytokines, IL-1, IL-6, TNF-α)
- Late septic SIRS = infection superimposed (translocation of gut bacteria into necrotic pancreas)
- Infected pancreatic necrosis = bacteraemia → septic shock → MODS; mortality up to 50%
- Organisms: E. coli, Klebsiella, Pseudomonas, Enterococcus (gut flora translocation)
- Early: supportive (no prophylactic antibiotics routinely - controversial)
- Late infected necrosis: CT/USS-guided fine needle aspiration → if purulent: drainage (endoscopic transgastric or percutaneous) + targeted antibiotics (imipenem/meropenem)
- Pancreatic necrosectomy as last resort
3. DIC (Disseminated Intravascular Coagulation)
- Activated pancreatic enzymes (trypsin, elastase, phospholipase A2) enter systemic circulation
- Trigger the extrinsic coagulation pathway → widespread microthrombi
- Consumption of clotting factors (V, VIII, fibrinogen) and platelets
- Secondary activation of fibrinolysis → uncontrolled bleeding
- Simultaneous thrombosis (multi-organ ischaemia) AND bleeding (skin petechiae, GI bleed, haematuria, oozing from venepuncture sites)
- Labs: ↓ platelets, ↓ fibrinogen, ↑ PT/APTT, ↑ D-dimer, ↑ FDPs (fibrin degradation products)
- Treat underlying cause (pancreatitis resuscitation)
- Fresh frozen plasma (FFP) for coagulopathy
- Platelet transfusion if <50,000/mm³ and bleeding
- Cryoprecipitate for fibrinogen replacement
- Heparin rarely used (controversial)
4. Gastrointestinal Haemorrhage / Bleeding
- Erosion of peripancreatic vessels (splenic artery most common) → haemorrhage into pseudocyst = "sentinel bleed" → potentially catastrophic
- Stress ulceration of gastric/duodenal mucosa (Curling's ulcer) due to shock and impaired mucosal perfusion
- Haemorrhagic pancreatitis - Grey Turner's sign, Cullen's sign
- Splenic vein thrombosis → gastric varices → haematemesis
- Portal hypertension from splenic vein compression
- Haemodynamic resuscitation
- Stress ulcer prophylaxis (PPI/H2 blocker)
- CT angiography to identify bleeding vessel → interventional radiology (embolisation)
- Surgery if refractory
5. Perforation
- Rare direct complication of acute pancreatitis
- Occurs secondary to enzymatic digestion of adjacent viscera (duodenum, transverse colon)
- More often: perforation is in the differential diagnosis (perforated peptic ulcer can simulate pancreatitis and vice versa)
- Also: infected pancreatic necrosis can erode into adjacent bowel → internal fistula or free perforation
- Colon (transverse colon) is most susceptible to enzymatic injury → colonic fistula
- Management: surgical repair; colostomy if colon involved
Systemic Complications Table (Bailey & Love)
| System | Complication |
|---|---|
| Cardiovascular | Shock, arrhythmias |
| Pulmonary | ARDS, pleural effusion, atelectasis, pneumonitis |
| Renal | Acute renal failure (ATN) |
| Haematological | DIC, haemorrhage |
| Metabolic | Hypocalcaemia, hyperglycaemia |
| GI | Haemorrhage, ileus, gastric/duodenal erosions |
| Hepatic | Jaundice, hepatocellular dysfunction |
Local Complications Table
| Complication | Timing | Features |
|---|---|---|
| Acute peripancreatic fluid collection (APFC) | <4 weeks | No wall; mostly resolve spontaneously |
| Pseudocyst | >4 weeks | Encapsulated fluid collection; no solid debris |
| Acute necrotic collection (ANC) | <4 weeks | Mixed fluid + necrotic tissue |
| Walled-off necrosis (WON) | >4 weeks | Well-defined capsule around necrotic material |
| Pancreatic abscess | Weeks | Infected fluid with little necrosis |
| Pancreatic duct disruption | Late | Pancreatic ascites/fistula |
TOPIC 3 - LIVER SEGMENTS (Couinaud Classification)
Concept
Anatomical Landmarks
- Cantlie's line: Plane through the middle hepatic vein and the IVC - divides liver into right and left hemilobes
- The right and left hepatic veins subdivide each hemilobe into two sectors
- Portal pedicles further divide sectors into segments
Couinaud Segments
| Segment | Location | Notes |
|---|---|---|
| I | Caudate lobe | Posterior; receives portal inflow from both right and left; drains directly into IVC via multiple small veins (caudate veins) |
| II | Left lobe, superior posterior | |
| III | Left lobe, inferior anterior | |
| IVa | Left medial, superior (quadrate lobe upper) | |
| IVb | Left medial, inferior (quadrate lobe lower) | |
| V | Right lobe, inferior anterior | |
| VI | Right lobe, inferior posterior | |
| VII | Right lobe, superior posterior | |
| VIII | Right lobe, superior anterior |
Functional Divisions
| Division | Segments |
|---|---|
| Left hemiliver | II, III, IV (IVa + IVb) |
| Right hemiliver | V, VI, VII, VIII |
| Caudate lobe | I (unique - independent drainage) |
Key Portal Anatomy
- Portal vein = confluence of superior mesenteric vein + splenic vein (at the neck of pancreas)
- Left portal vein is longer, more horizontal; right portal vein shorter
- Common hepatic artery → from coeliac axis → proper hepatic artery → right and left hepatic arteries (arterial variation in 40%)
- Replaced right hepatic artery arises from SMA (13% of patients) - must be identified at surgery
Clinical Relevance of Segments
| Surgery | Segments Removed |
|---|---|
| Left lateral sectionectomy | II + III |
| Left hepatectomy | II + III + IV |
| Right hepatectomy | V + VI + VII + VIII |
| Extended right hepatectomy | V + VI + VII + VIII + IV |
| Trisectionectomy | Any 6 segments |
TOPIC 4 - INFLAMMATORY BOWEL DISEASE (IBD)
Definition
| Feature | Ulcerative Colitis (UC) | Crohn's Disease (CD) |
|---|---|---|
| Distribution | Colon only; starts in rectum, extends proximally; continuous | Any part of GI tract (mouth to anus); skip lesions |
| Extent | Rectum always involved | Rectum often spared |
| Layer | Mucosa + submucosa only | Transmural (all layers) |
| Pattern | Continuous, confluent | Skip lesions (discontinuous) |
| Gross appearance | Pseudopolyps, friable mucosa, loss of haustra | Cobblestone mucosa, aphthous ulcers, fat wrapping, strictures, fistulas, fissures |
| Histology | Crypt abscesses, goblet cell depletion | Non-caseating granulomas (50%), transmural inflammation |
| Smoking | Protective | Risk factor |
| Rectal bleeding | Major feature | Less common |
| Diarrhoea | Bloody, mucoid | May be non-bloody; steatorrhoea if small bowel |
| Abdominal pain | Left lower quadrant | Right lower quadrant (terminal ileum) |
| Perianal disease | Rare | Common: fissures, fistulas, abscesses, skin tags |
| Fistulas | Rare | Common: enteroenteric, enterovesical, enterocutaneous, rectovaginal |
| Malabsorption | Uncommon | Common (small bowel involvement, B12 deficiency) |
| Serology | pANCA positive | ASCA positive |
| Surgery | Total colectomy = curative | NOT curative; high recurrence after surgery |
| CRC risk | Significantly elevated (10% after 10yr, rising 10%/decade) | Elevated (4-20× general population) |
Extra-intestinal Manifestations (Both)
| System | Manifestation |
|---|---|
| Joints | Peripheral arthritis (correlates with disease activity); Ankylosing spondylitis, sacroiliitis (independent of activity) |
| Skin | Erythema nodosum (correlates with activity); Pyoderma gangrenosum (independent) |
| Eyes | Episcleritis (correlates); Uveitis/iritis (independent) |
| Liver/biliary | Primary sclerosing cholangitis (PSC) - strongly associated with UC; hepatitis; cholangiocarcinoma |
| Renal | Nephrolithiasis (calcium oxalate and uric acid stones) |
| Haematological | Anaemia (iron deficiency in UC; B12/folate in CD) |
Complications
| Disease | Specific Complications |
|---|---|
| UC | Toxic megacolon, massive haemorrhage, perforation, colorectal cancer, stricture |
| Crohn's | Stricture (small bowel obstruction), fistulas, abscesses, perianal disease, malabsorption, short bowel syndrome |
Management Overview
| Step | UC | Crohn's |
|---|---|---|
| Mild-Moderate | Mesalazine (5-ASA) oral/rectal | Corticosteroids |
| Moderate-Severe | Oral corticosteroids, azathioprine/6-MP | Azathioprine, methotrexate |
| Severe/Refractory | IV hydrocortisone; ciclosporin; infliximab | Infliximab, adalimumab |
| Surgery | Proctocolectomy (curative) | Resection (not curative); fistula repair |
TOPIC 5 - COLORECTAL CARCINOMA (CRC)
Epidemiology
- 3rd most common cancer worldwide; 2nd most common cause of cancer death
- Peak incidence: 60-70 years; males slightly more than females
- Incidence increasing in young adults with IBD or Lynch syndrome
Risk Factors
| Category | Risk Factors |
|---|---|
| Diet | High red/processed meat, low fibre, high fat, obesity |
| Lifestyle | Physical inactivity, alcohol, smoking |
| Pre-malignant lesions | Adenomatous polyps (especially villous, >1 cm, high-grade dysplasia) |
| IBD | UC and Crohn's colitis (dysplasia → carcinoma sequence) |
| Genetic | FAP (APC mutation; 100% risk by age 40); Lynch syndrome/HNPCC (MLH1, MSH2, MSH6 mismatch repair mutations; 50-80% lifetime risk) |
| Family history | First-degree relative with CRC |
Adenoma-Carcinoma Sequence
Clinical Features
Symptoms vary by location:
| Location | Typical Presentation |
|---|---|
| Right colon | Occult blood, iron deficiency anaemia, weight loss, mass in RIF; rarely obstruction (large lumen) |
| Left colon | Change in bowel habit, alternating constipation/diarrhoea, rectal bleeding, narrowing of stool calibre, obstruction more common |
| Rectum | Tenesmus, rectal bleeding (bright red), feeling of incomplete evacuation, mucus PR |
Staging
Dukes Classification (Modified):
| Stage | Description | 5-Year Survival |
|---|---|---|
| A | Confined to bowel wall (not through muscularis propria) | ~90% |
| B | Through bowel wall, NO lymph node involvement | ~65-75% |
| C | Regional lymph node involvement | ~30-40% |
| D | Distant metastases (liver, lung, peritoneum) | <5% |
TNM Staging (AJCC 8th Edition - current standard):
| Stage | TNM | Equivalent |
|---|---|---|
| 0 | Tis N0 M0 | Carcinoma in situ |
| I | T1-T2, N0, M0 | Dukes A |
| II | T3-T4, N0, M0 | Dukes B |
| III | Any T, N1-N2, M0 | Dukes C |
| IV | Any T, Any N, M1 | Dukes D (distant mets) |
Investigations
- Colonoscopy + biopsy: Gold standard; identifies synchronous lesions (~50% of patients)
- CT colonography (virtual colonoscopy): For patients unable to tolerate colonoscopy
- CT chest/abdomen/pelvis: Staging for metastases
- MRI pelvis: Rectal cancer staging - T-stage, circumferential resection margin (CRM)
- CEA (carcinoembryonic antigen): Not for diagnosis; used for post-operative surveillance (rising CEA = recurrence)
- FBC: Anaemia (iron deficiency)
- LFTs: Liver metastases
Surgical Management
- Right hemicolectomy: Caecal, ascending colon, hepatic flexure
- Left hemicolectomy: Descending colon
- Anterior resection: Sigmoid and upper rectum
- Abdominoperineal resection (APR): Low rectal; permanent colostomy
- Hartmann's procedure: Emergency obstruction/perforation; colostomy + rectal stump
- Total mesorectal excision (TME): Standard for rectal cancer; reduces local recurrence
TOPIC 6 - LIVER PATHOLOGIES
A. HEPATOCELLULAR CARCINOMA (HCC)
Epidemiology
- Most common primary liver tumour globally; 5th most common cancer worldwide
- M:F = 4-8:1; peak in 5th-6th decade (earlier in endemic areas)
Risk Factors
- Cirrhosis (any cause) - most important; 70-90% of HCC arises in cirrhotic liver
- Hepatitis B (HBsAg carriers - risk even without cirrhosis via direct oncogenic mechanisms; HBx protein)
- Hepatitis C (cirrhosis required for carcinogenesis)
- Aflatoxin B1 (Aspergillus-contaminated food - endemic in Africa/Asia)
- Alcohol-related cirrhosis
- NAFLD/NASH-related cirrhosis
- Haemochromatosis, Wilson's disease, α1-antitrypsin deficiency
Clinical Features
- Often silent until advanced (pre-existing cirrhosis masks symptoms)
- Right upper quadrant pain / dull ache
- Hepatomegaly - hard, nodular liver; hepatic bruit in 25%
- Weight loss, anorexia, malaise
- Jaundice - late feature
- Ascites - usually haemorrhagic
- Decompensation of previously stable cirrhosis
- Paraneoplastic syndromes: Hypoglycaemia (insulin-like factors), hypercalcaemia, erythrocytosis, polycythaemia
Investigations
| Test | Finding |
|---|---|
| AFP (α-fetoprotein) | Elevated in 70-80%; normal <20 ng/mL; very high levels (>400 ng/mL) highly suggestive; monitor in cirrhosis every 6 months with USS |
| Ultrasound | Screening tool; hypoechoic mass |
| CT with contrast (triphasic) | Arterial enhancement + venous washout = diagnostic pattern (no biopsy needed if classic) |
| MRI | Better soft tissue characterization |
| Liver biopsy | If imaging inconclusive; risk of seeding (1%) |
| LFTs + PT | Assess underlying liver function |
| Child-Pugh score | Assess severity of cirrhosis (guides resectability): bilirubin, albumin, INR, ascites, encephalopathy |
Staging (BCLC - Barcelona Clinic Liver Cancer):
- Stage 0/A: Very early/early - resection or transplantation curative
- Stage B: Intermediate - TACE (transarterial chemoembolisation)
- Stage C: Advanced - Sorafenib/Lenvatinib
- Stage D: Terminal - palliative
Milan Criteria for Transplantation:
- Single tumour ≤5 cm OR up to 3 tumours each ≤3 cm, no vascular invasion, no extrahepatic spread
B. LIVER ABSCESS
Two main types:
| Feature | Pyogenic Liver Abscess | Amoebic Liver Abscess |
|---|---|---|
| Causative organism | E. coli, Klebsiella (most common), Streptococcus, Bacteroides | Entamoeba histolytica |
| Origin | Ascending cholangitis, portal pyaemia, biliary disease, direct extension | Faeco-oral route; amoeba from colon disseminates via portal vein |
| Geography | Worldwide | Tropics/subtropics (India, Africa, Mexico) |
| Number | Often multiple | Usually single, right lobe |
| Content | Pus (thick, yellow-green) | "Anchovy sauce" - reddish-brown, odourless |
| Pain | RUQ/hepatic; referred to right shoulder | RUQ; referred to right shoulder |
| Fever | Swinging, high-grade, rigors | High-grade with sweating |
| Jaundice | Present (if biliary obstruction) | Rare |
| Diarrhoea | Absent | May have history of amoebic dysentery |
| Serology | - | Amoebic serology (ELISA/IHA) positive in >95% |
| Diagnosis | USS/CT + blood cultures | USS/CT + serology |
| Treatment | IV antibiotics (cephalosporin + metronidazole) + percutaneous drainage | Metronidazole 400-800 mg TDS × 5-10 days + luminal agent (diloxanide furoate); drainage usually NOT needed |
| Complication | Septicaemia, rupture into peritoneum/pleura | Rupture into pleura (empyema), pericardium |
C. HEPATITIS
Viral Hepatitis Overview
| Feature | Hep A | Hep B | Hep C | Hep D | Hep E |
|---|---|---|---|---|---|
| Virus type | RNA (HAV) | DNA (HBV) | RNA (HCV) | RNA (HDV) | RNA (HEV) |
| Transmission | Faeco-oral | Parenteral, sexual, perinatal | Parenteral (IVDU), sexual | Parenteral (requires HBV) | Faeco-oral |
| Incubation | 2-6 weeks | 6 weeks - 6 months | 6-12 weeks | Same as HBV | 2-9 weeks |
| Chronicity | NEVER | 5-10% adults; 90% neonates | 85% → chronic | Co-infection rarely; superinfection 80% | NEVER (except immunosuppressed) |
| Cirrhosis risk | No | Yes (20-30% chronic) | Yes (20-30% in 20 years) | High (superinfection) | No (except HEV in immunosuppressed) |
| HCC risk | No | Yes (200× increased) | Yes | Yes | No |
| Vaccine | Yes | Yes | No | Prevented by HBV vaccine | Yes (not widely available) |
| Specific treatment | Supportive | Tenofovir, entecavir (nucleoside analogues) | Direct-acting antivirals (DAAs): sofosbuvir, ledipasvir; >95% cure | Peginterferon-α | Supportive |
Hepatitis B Serology
| Marker | Meaning |
|---|---|
| HBsAg | Current infection (acute or chronic) |
| Anti-HBs | Past infection (cleared) or vaccination - protective |
| HBeAg | Active replication - highly infectious |
| Anti-HBe | Viral replication declining |
| HBcAg | Core antigen - NOT detectable in serum |
| Anti-HBc IgM | Acute infection (diagnostic window) |
| Anti-HBc IgG | Past or chronic infection |
| HBV DNA | Viral load - monitors treatment response |
Acute Hepatitis - Clinical Features (all types)
- Pre-icteric phase: Malaise, anorexia, nausea, vomiting, fever, myalgia, RUQ discomfort; smokers lose desire to smoke; dark urine (bilirubinuria)
- Icteric phase: Jaundice (yellow sclera first), pale stools, dark urine, pruritus, hepatomegaly (tender), splenomegaly (25%)
- Resolution phase: Symptoms improve, jaundice fades
Fulminant Hepatic Failure (FHF)
- Encephalopathy within 8 weeks of onset in previously healthy liver
- Features: coagulopathy (INR >1.5), encephalopathy, cerebral oedema
- Most common causes: Hep B, paracetamol toxicity (in UK), Wilson's disease
- Management: ICU, liver transplantation if criteria met (King's College Criteria)
Chronic Hepatitis - Consequences
- Fibrosis → Cirrhosis → Portal hypertension, varices, ascites, encephalopathy, hepatorenal syndrome, HCC
- Bailey & Love's Short Practice of Surgery, 28th Ed, Ch. 72 (Pancreatitis), pp. 1290-1300
- Mulholland & Greenfield's Surgery, 7th Ed, Ch. 57 (Liver Anatomy), pp. 2775-2780
- Sleisenger & Fordtran's GI and Liver Disease - IBD and CRC chapters
- Robbins & Kumar Basic Pathology / Pathologic Basis of Disease
- Schwartz's Principles of Surgery, 11th Ed, Ch. 39/15
Definition of intestinal obstruction Classification: Dynamic (mechanical) Adynamic (non-mechanical) Overview of importance and complications
Intestinal Obstruction - Complete Notes
DEFINITION
- Tintinalli's Emergency Medicine: "Intestinal obstruction is the inability of the intestinal tract to allow for regular passage of food and bowel contents secondary to mechanical obstruction or adynamic ileus."
- Pye's Surgical Handicraft: Intestinal obstruction may result from vascular occlusion, mechanical, or neuromuscular factors - all preventing the normal aboral flow of bowel contents.
CLASSIFICATION
TYPE 1: DYNAMIC (MECHANICAL) OBSTRUCTION
Peristalsis is present and active - it is working against a physical block. Also called mechanical obstruction.
- Initially shows increased peristalsis (attempt to overcome the block → produces colicky pain and audible bowel sounds)
- With time, dilates, then undergoes flaccidity and paralysis (due to fatigue)
- The bowel distal to the obstruction continues normal peristalsis and absorption until it empties and collapses
Sub-classification by location of the block:
| Mechanism | Examples |
|---|---|
| Intraluminal (inside the lumen) | Faecal impaction, gallstones (gallstone ileus), bezoars (phytobezoar, trichobezoar), foreign bodies, worms |
| Intramural (in the bowel wall) | Malignancy (carcinoma), stricture (Crohn's disease, TB, radiation), intussusception, volvulus (twisting of bowel on its mesentery), congenital atresia |
| Extramural (outside the bowel wall) | Adhesions and bands, hernias (inguinal, femoral, umbilical, incisional, internal), external compression by tumour, abscess, or pregnancy |
Sub-classification by urgency/blood supply:
| Type | Definition | Clinical significance |
|---|---|---|
| Simple obstruction | Bowel lumen blocked; blood supply intact | Less immediately life-threatening |
| Strangulating / Strangulated obstruction | Lumen blocked AND blood supply compromised | Surgical emergency - rapidly fatal |
| Closed-loop obstruction | Bowel blocked at both proximal and distal ends simultaneously | Very high pressure builds up; rapid progression to gangrene; e.g., colonic obstruction with competent ileocaecal valve, incarcerated hernia |
Further classification by onset:
- Acute: Sudden complete blockage
- Chronic / Subacute: Gradual narrowing (tumour, stricture) - incomplete or intermittent obstruction
TYPE 2: ADYNAMIC (NON-MECHANICAL) OBSTRUCTION
There is no physical block. Instead, peristalsis is absent or inadequate due to failure of neuromuscular transmission in the bowel wall.
Sub-types:
A. Paralytic Ileus
| Cause | Detail |
|---|---|
| Postoperative | Most common; degree of ileus follows any abdominal procedure; normally self-limiting within 24-72 hours; prolonged by hypoproteinaemia or metabolic disturbance |
| Intra-abdominal infection/peritonitis | Local or generalised ileus from peritoneal irritation |
| Metabolic | Hypokalaemia (most important), uraemia, hyponatraemia, hypomagnesaemia |
| Reflex ileus | Retroperitoneal haemorrhage, fractured spine/ribs, plaster jacket application |
| Drugs | Opioids, anticholinergics |
| Ischaemia / vascular | Mesenteric vascular occlusion |
| Trauma | Blunt abdominal trauma |
| Systemic illness | Sepsis, pneumonia, myocardial infarction |
- Clinically significant if at 72 hours post-laparotomy: no return of bowel sounds AND no passage of flatus
- Abdominal distension - tympanic, progressive
- Effortless vomiting (no colic - distinguishes from mechanical obstruction)
- Absent bowel sounds (silent abdomen)
- Absolute constipation
- Diffuse, mild abdominal discomfort (not colicky)
- X-ray: gas-filled loops of both small and large bowel with fluid levels; no single point of transition
- Nasogastric suction (not routinely post-elective surgery but needed if prolonged)
- Nil by mouth until bowel sounds return and flatus passed
- IV fluid replacement and electrolyte correction (especially K⁺)
- Treat underlying cause (infection, metabolic)
- Neostigmine 0.5 mg subcutaneously: acetylcholinesterase inhibitor → increases acetylcholine → stimulates peristalsis (especially for colonic pseudo-obstruction)
- CT scan if paralytic ileus prolonged (to exclude mechanical cause or intra-abdominal sepsis)
B. Pseudo-obstruction (Ogilvie's Syndrome)
- Conservative first: NBM, IV fluids, electrolytes, encourage mobility, stop offending drugs
- Colonoscopic decompression (first-line intervention)
- IV Neostigmine 2mg IV over 3-5 minutes: highly effective for acute colonic pseudo-obstruction; requires cardiac monitoring (risk of bradycardia)
- Surgery (caecostomy or colostomy) only if above fails or perforation occurs
COMPARISON: DYNAMIC vs ADYNAMIC OBSTRUCTION
| Feature | Dynamic (Mechanical) | Adynamic (Paralytic Ileus) |
|---|---|---|
| Mechanism | Physical block in/around bowel | Neuromuscular failure; no physical block |
| Peristalsis | Present (working against block) | Absent |
| Pain | Colicky, severe, intermittent waves | No colic; mild diffuse discomfort |
| Vomiting | Present, progressive (bilious → faeculent) | Effortless vomiting |
| Bowel sounds | High-pitched, tinkling rushes | Absent / Quiet ("silent abdomen") |
| Distension | Present (degree depends on site) | Present (usually generalised) |
| Constipation | Absolute (complete) | Present |
| X-ray | Dilated loops with transition point; stepladder fluid levels; collapsed bowel distal to block | Generalised gas throughout small AND large bowel; no transition point |
| Treatment | Usually surgical | Usually conservative (treat cause) |
| Urgency | High (especially if strangulated) | Lower (unless pseudo-obstruction with caecal dilatation) |
OVERVIEW OF IMPORTANCE AND COMPLICATIONS
Why Intestinal Obstruction Matters
- Common surgical emergency - accounts for ~3% of all acute abdominal pain admissions
- Progressive and potentially lethal - mortality rises with each passing hour; untreated complete obstruction is fatal
- May mask serious underlying pathology (malignancy, hernia, ischaemia)
- Mimics many other conditions: pancreatitis, perforated peptic ulcer, MI, pneumonia
- Adhesions (~60%) - post-surgical
- Hernias (~20%)
- Neoplasms (~5%)
- Inflammatory (Crohn's, diverticulitis)
- Others (volvulus, intussusception, gallstone ileus)
PATHOPHYSIOLOGY (How Complications Arise)
- Gas accumulation: bacterial overgrowth produces gas (90% nitrogen after O₂/CO₂ reabsorption); swallowed air
- Fluid accumulation: digestive secretions (saliva 500 mL + bile 500 mL + pancreatic 500 mL + gastric 1 L/day = ~2.5 L/day minimum) accumulate as absorption fails
COMPLICATIONS
A. Fluid and Electrolyte Complications
| Complication | Mechanism |
|---|---|
| Dehydration | Vomiting, reduced oral intake, sequestration in lumen and peritoneal cavity, transudation |
| Hyponatraemia | Loss of Na⁺-rich secretions |
| Hypokalaemia | Vomiting, alkalosis (H⁺ lost → K⁺ shifts into cells), deficient intake |
| Metabolic alkalosis | Loss of HCl in vomitus (especially in proximal obstruction) |
| Metabolic acidosis | Bowel ischaemia, lactic acidosis (late) |
| Hypovolaemic shock | Massive fluid loss → reduced circulating volume → organ failure |
| Acute kidney injury (AKI) | Pre-renal failure from dehydration and shock |
B. Strangulation and Ischaemia
- Hernial orifices (direct compression)
- Volvulus (twisted mesenteric vessels)
- Intussusception (trapped mesentery)
- Closed-loop obstruction (elevated intraluminal pressure)
- Venous return compromised first (low pressure) → venous congestion → oedema
- Raised capillary pressure → impaired local perfusion
- Arterial supply compromised → haemorrhagic infarction → necrosis
- Bacterial translocation from ischaemic bowel → endotoxaemia → sepsis
C. Perforation
- Bowel wall necrosis → full-thickness gangrene → perforation
- Most dangerous site: caecum in large bowel obstruction (thinnest wall + largest diameter)
- Caecal perforation risk when diameter >12 cm
- Perforation → faecal peritonitis → septicaemia → mortality >50%
D. Septic Complications
| Complication | Mechanism |
|---|---|
| Septicaemia / bacteraemia | Translocation of gut flora through ischaemic bowel wall |
| Peritonitis | Perforation or transmural bacterial migration |
| Abdominal abscess | Localised peritonitis |
| Endotoxaemia | Gram-negative bacterial endotoxin → SIRS → MODS |
E. Systemic / Multi-organ Complications
| System | Complication |
|---|---|
| Cardiovascular | Hypovolaemic shock, septic shock, arrhythmias |
| Respiratory | Diaphragmatic splinting from distension → atelectasis, pneumonia; ARDS (sepsis) |
| Renal | Pre-renal AKI (dehydration); intrinsic AKI (sepsis, endotoxaemia) |
| Haematological | DIC (from sepsis/endotoxaemia) |
| Hepatic | Hepatic dysfunction from portal bacteraemia |
| CNS | Confusion, encephalopathy (metabolic or septic) |
F. Complications Specific to Treatment/Surgery
| Complication | Details |
|---|---|
| Anastomotic leak | Post-resection and anastomosis |
| Wound infection | Common post-emergency laparotomy |
| Short bowel syndrome | Extensive bowel resection for gangrene |
| Post-operative adhesions | Ironically, surgery for obstruction creates more adhesions → risk of future episodes |
| Stoma complications | Prolapse, retraction, skin excoriation |
Summary of Key Points
Intestinal Obstruction
│
├── DYNAMIC (Mechanical) ─── Peristalsis present, fighting a block
│ ├── Intraluminal (faeces, FB, gallstone, bezoar)
│ ├── Intramural (CA, stricture, intussusception, volvulus)
│ └── Extramural (adhesions, hernia)
│ ├── Simple (blood supply intact)
│ └── Strangulated (blood supply compromised - EMERGENCY)
│
└── ADYNAMIC (Non-mechanical) ─── Peristalsis absent/inadequate
├── Paralytic ileus (post-op, sepsis, metabolic, reflex)
└── Pseudo-obstruction / Ogilvie's syndrome (colonic)
Complications (untreated):
Dehydration → Hypovolaemic shock
Distension → Ischaemia → Strangulation → Gangrene → Perforation
Bacterial translocation → Septicaemia → SIRS → MODS → Death
- Bailey & Love's Short Practice of Surgery, 28th Ed, Ch. 78, pp. 1394-1412
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Ch. 83, pp. 685-727
- S. Das - Manual on Clinical Surgery, 13th Ed, pp. 478-484
- Pye's Surgical Handicraft, 22nd Ed, pp. 9001-9061
- Robbins & Kumar Basic Pathology, p. 561
Thyroid ca 101