4.4 mm renal calculus in lower calyx management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"renal calculi"[MeSH Terms] AND "lower pole" AND management
Finding Sources
Finding Sources
Searching PubMed
"nephrolithiasis"[MeSH Terms] AND "lower pole" AND "treatment"
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive management overview for a 4.4 mm lower calyx renal calculus.
4.4 mm Lower Calyx Renal Stone — Management
Where This Stone Falls in Guidelines
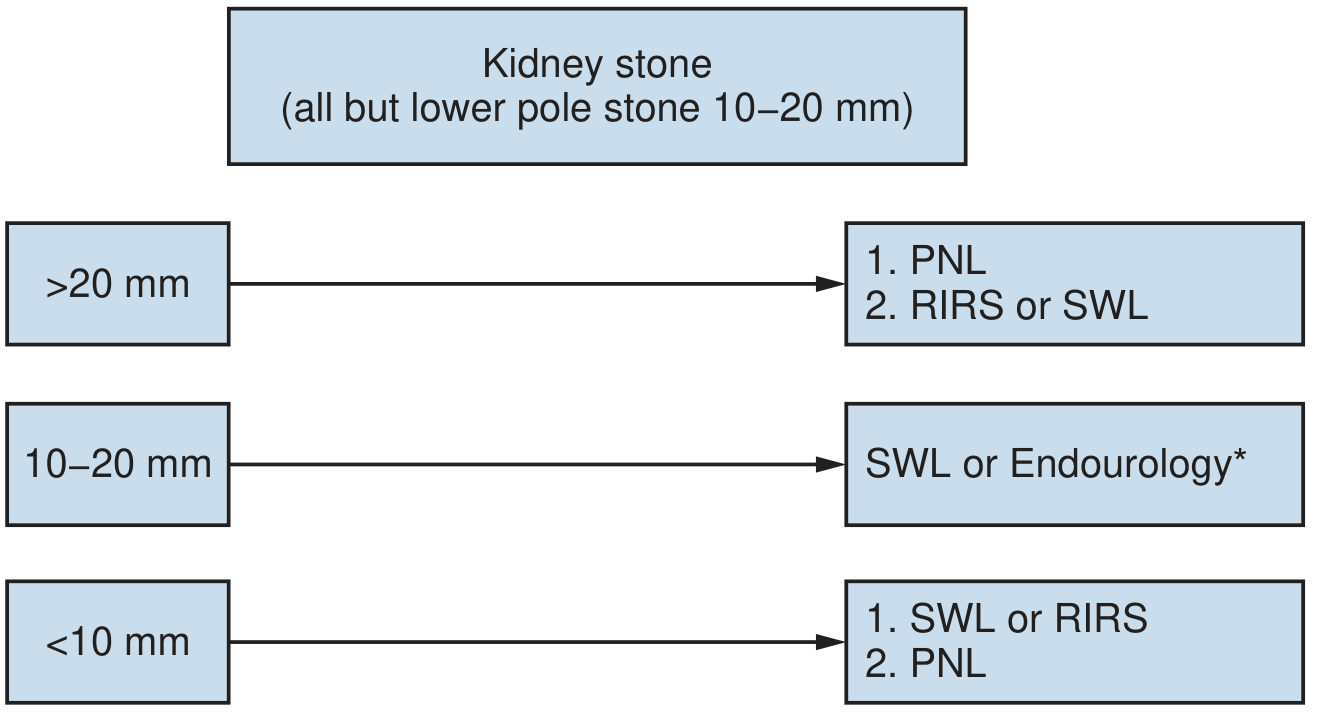
A 4.4 mm lower pole stone is a small (<10 mm) lower pole calculus. Per AUA/EAU guidelines, first-line options are ESWL or ureteroscopy (URS/RIRS); PCNL is reserved for failures or special anatomical situations.
Step 1 — Conservative / Watchful Waiting (Reasonable First Step)
For a 4.4 mm asymptomatic or minimally symptomatic lower pole stone:
- Spontaneous passage occurs in ~21% of lower pole calculi (mean size ~8.8 mm in studies; smaller stones pass more readily)
- Stones ≤5 mm have a higher chance of passage; spontaneous passage is expected in up to 80% of stones <4 mm
- ~46% of lower pole stones enlarge over time; ~11% eventually require intervention
- The risk of eventual surgical intervention is ~10–20% at 3–4 years
Conservative management includes:
- Increased fluid intake (>2.5 L/day urine output)
- Dietary modification (low sodium, normal calcium, low oxalate if calcium oxalate)
- Regular imaging follow-up (USS or low-dose CT) at 6–12 months
Step 2 — Medical Expulsive Therapy (MET)
If the stone is in/near the ureter or causing symptoms:
- Tamsulosin 0.4 mg once daily (alpha blocker) — aids passage, especially for distal ureteral stones <10 mm
- Nifedipine 30 mg once daily (calcium channel blocker) — alternative
- Evidence is mixed for purely renal (calyceal) stones; MET is most effective for ureteral stones
- Most guidelines still recommend MET for small distal ureteral stones
Step 3 — Indications for Active Intervention
Intervene if any of the following apply:
- Persistent pain >72 hours despite adequate analgesia
- Obstruction with risk of renal impairment (single kidney, pre-existing CKD)
- Associated UTI / urosepsis
- Stone growth on follow-up imaging
- Patient preference or occupational requirement (e.g., pilot, military)
- Failed conservative management after 4–6 weeks
Step 4 — Surgical Options for Lower Pole <10 mm Stone
| Modality | Stone-free Rate | Notes |
|---|---|---|
| ESWL (SWL) | ~46–74% for lower pole | Poor clearance due to gravity-dependent position; narrow infundibulopelvic angle worsens results; stone attenuation ≥1000 HU, skin-to-stone >10 cm reduce success |
| Flexible URS / RIRS (laser lithotripsy) | ~80–100% in experienced centers | Preferred over ESWL for lower pole; holmium laser dusting improves clearance; Lower Pole II trial showed 50% SFR by CT — newer technology improves this |
| PCNL / Mini-PCNL | >95% | Reserved for failure of ESWL/URS, anatomic anomalies, or stone burden requiring single-session clearance |
Key lower pole-specific considerations for ESWL (factors negatively affecting success):
- Narrow infundibulopelvic angle (<70°)
- Narrow infundibular diameter (<4 mm)
- Long lower pole calyx (>3 cm)
- Stone attenuation ≥1000 HU on CT
- Skin-to-stone distance >10 cm
If these unfavorable anatomic factors are present, flexible URS/RIRS is preferred over ESWL even for a small stone.
Practical Recommendation Summary
| Scenario | Recommended Approach |
|---|---|
| Asymptomatic, no unfavorable anatomy | Conservative: fluids + dietary advice + surveillance imaging |
| Symptomatic (colic, recurrent UTI) | MET trial (tamsulosin) + consider active intervention if no passage in 4–6 weeks |
| Active intervention needed, favorable anatomy | ESWL or flexible URS (RIRS with holmium laser) |
| Unfavorable lower pole anatomy | Flexible URS/RIRS preferred |
| ESWL/URS failure | Mini-PCNL or standard PCNL |
Recent Evidence
- Cochrane review (2023) comparing ESWL vs PCNL vs RIRS confirms PCNL has highest stone-free rates but greater morbidity; ESWL and RIRS are comparable for small stones with RIRS having fewer repeat procedures (PMID: 37526261)
- Flexible URS for lower pole review (2023) highlights that with modern flexible scopes and dusting techniques, lower pole access is no longer a major challenge (PMID: 37728745)
Sources: Campbell-Walsh Wein Urology, 11e | Comprehensive Clinical Nephrology, 7e (Table 63.3, AUA/EAU Guidelines)
This is a shared conversation. Sign in to Orris to start your own chat.