Give me a 10marks answer about recent ASA difficult airway algorithm from ASA website for md anaesthesia exams
ASA difficult airway algorithm 2022 2023 updated guidelines
"difficult airway" AND "ASA" AND "algorithm"
https://www.asahq.org/~/media/sites/asahq/files/public/resou…
ASA Difficult Airway Algorithm (2022 Update) - 10 Marks Answer
Introduction
Definition of Difficult Airway (ASA 2022)
- Difficulty with patient cooperation or consent
- Difficult face mask ventilation
- Difficult supraglottic airway (SGA) placement
- Difficult laryngoscopy
- Difficult tracheal intubation
- Difficult surgical airway access
The 2022 ASA Difficult Airway Algorithm - Overview
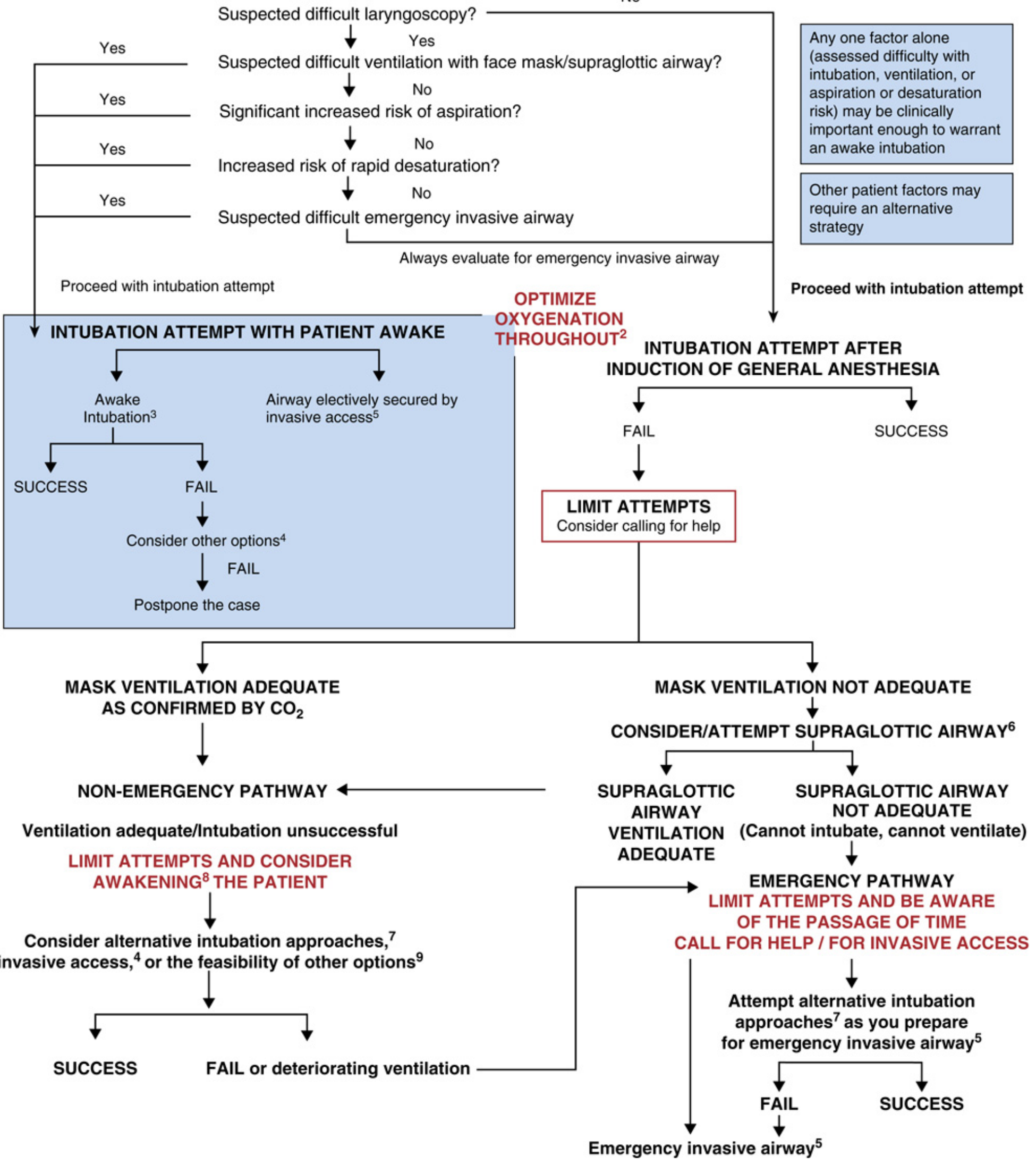
Step-by-Step Components of the Algorithm
Step 1: Pre-Intubation Assessment
- Assess likelihood of the six basic management problems (see above)
- Evaluate for emergency invasive airway access - always
- Decide on awake vs. post-induction strategy
Step 2: Two Primary Pathways
A. AWAKE INTUBATION (Patient Awake)
- Suspected difficult laryngoscopy
- Suspected difficult face mask/SGA ventilation
- Significant increased aspiration risk
- Increased risk of rapid desaturation
- Suspected difficult emergency invasive airway
- Flexible bronchoscopy
- Videolaryngoscopy
- Direct laryngoscopy
- Combined techniques
- Retrograde wire-aided intubation
- Awake elective invasive airway access
B. INTUBATION AFTER INDUCTION OF GENERAL ANESTHESIA
- If intubation succeeds → proceed.
- If intubation fails → LIMIT ATTEMPTS, Consider calling for help.
Step 3: Post-Induction Failure - Two Branches
Branch A: MASK VENTILATION ADEQUATE - NON-EMERGENCY PATHWAY
- Ventilation adequate, intubation unsuccessful
- LIMIT ATTEMPTS AND CONSIDER AWAKENING THE PATIENT
- Consider:
- Alternative intubation approaches (see footnote 7 below)
- Invasive airway access
- Feasibility of other options (e.g., SGA for maintenance, regional technique)
- Success → proceed
- Fail or deteriorating ventilation → transition to Emergency Pathway
Branch B: MASK VENTILATION NOT ADEQUATE - EMERGENCY PATHWAY
- Attempt SGA/Supraglottic airway immediately
- Returns to Non-Emergency Pathway (ventilation adequate)
- EMERGENCY PATHWAY
- LIMIT ATTEMPTS AND BE AWARE OF PASSAGE OF TIME
- CALL FOR HELP / FOR INVASIVE ACCESS
- Attempt alternative intubation approaches simultaneously as you prepare for emergency invasive airway
- Ultimately → Emergency Invasive Airway
Key Footnotes / Algorithm Annotations (2022)
| Annotation | Meaning |
|---|---|
| ¹ | Strategy choice based on experience, equipment, available help, clinical context |
| ² | OPTIMIZE OXYGENATION THROUGHOUT - low or high-flow nasal cannula, head-elevated position, NIV during preoxygenation |
| ³ | Awake intubation: flexible bronchoscopy, VL, DL, combined, retrograde |
| ⁴ | Other options: alternative awake technique, regional/local anesthesia, postpone |
| ⁵ | Invasive airway: surgical cricothyrotomy, needle cricothyrotomy + pressure device, large-bore cannula cricothyrotomy, surgical tracheostomy; also retrograde wire-guided, percutaneous tracheostomy, rigid bronchoscopy, ECMO |
| ⁶ | Consider SGA size, design, positioning; first- vs. second-generation SGAs |
| ⁷ | Alternative difficult intubation approaches: videolaryngoscopy, alternate blades, intubating SGA ± bronchoscopic guidance, flexible bronchoscopy, introducer, lighted stylet |
| ⁸ | Awakening patient = most important patient safety step in non-emergency pathway |
| ⁹ | Other options: proceed with face mask or SGA ventilation for the procedure |
Key Updates in 2022 vs. Previous Versions
| Feature | Previous (2013) | 2022 Update |
|---|---|---|
| Human Factors | Not emphasized | Now explicitly incorporated (team behavior, environmental factors, individual performance) |
| Oxygenation | Supplemental O₂ recommended | "Optimize oxygenation throughout" emphasized - includes HFNO, NIV, head-elevated position |
| Videolaryngoscopy | Listed as alternative | Now listed as primary alternative and an initial approach consideration |
| Calling for Help | Implied | Explicitly stated - "Consider calling for help" and "Call for help / for invasive access" in red on algorithm |
| Limiting Attempts | Mentioned | Prominently highlighted in red - "Limit attempts and be aware of passage of time" |
| SGA role | Rescue device | Explicitly addressed as first-line rescue in emergency pathway |
| Cognitive Aids | Not mentioned | Human factors, checklists, cognitive aids (e.g., Vortex approach) recommended |
| Documentation | Required | Still required - document difficulty, inform patient, follow-up for complications |
Pre-Intubation Airway Physical Examination (ASA Table)
- Relatively long upper incisors
- Prominent overbite (maxillary > mandibular incisors)
- Cannot bring mandibular incisors anterior to maxillary (poor jaw protrusion)
- Interincisor distance < 3 cm
- Mallampati class > 2 (uvula not visible)
- Highly arched or narrow palate
- Stiff, indurated, or occupied mandibular space
- Thyromental distance < 6 cm
- Short, thick neck; limited neck extension
Preoxygenation and Oxygenation During Management
- Apneic oxygenation using nasal cannula at 15 L/min (or high-flow nasal oxygen - HFNO)
- Head-elevated laryngoscopy position (HELP) - 25-30° elevation improves FRC and view
- Non-invasive ventilation (NIV/BiPAP) during preoxygenation in obese or hypoxic patients
- CO₂ monitoring (capnography) to confirm every airway device placement
CICO (Cannot Intubate Cannot Oxygenate) - Emergency Invasive Airway
- Proceed without delay to emergency invasive airway
- Preferred technique: Surgical cricothyrotomy (most reliable)
- Alternatives: Needle cricothyrotomy + pressure-regulated ventilation device; large-bore cannula cricothyrotomy
- Also consider: Rigid bronchoscopy, ECMO (if available)
Documentation and Follow-Up (Mandatory)
- Document the presence and nature of airway difficulty in the medical record
- Inform the patient (or responsible person) of the airway difficulty encountered
- Evaluate and follow up for potential complications (e.g., dental injury, subglottic stenosis, tracheal injury, airway edema)
- Advise the patient of potential clinical signs/symptoms of life-threatening complications
Summary Table: Algorithm Pathway at a Glance
PRE-INTUBATION ASSESSMENT
↓
Difficult airway suspected?
├── YES → AWAKE INTUBATION
│ ├─ Success → Proceed
│ └─ Fail → Other options → Postpone
└── NO → POST-INDUCTION INTUBATION
├─ Success → Proceed
└─ Fail → Limit attempts, Call for help
↓
Mask ventilation adequate?
├── YES → NON-EMERGENCY PATHWAY
│ Limit attempts, Consider awakening
│ Alternative techniques / Invasive access
└── NO → Attempt SGA
├─ SGA adequate → Non-emergency pathway
└─ SGA NOT adequate (CICO)
↓ EMERGENCY PATHWAY
Call for help, Limit time
Alternative intubation + prepare invasive
→ EMERGENCY INVASIVE AIRWAY
References
- ASA Practice Guidelines for Management of the Difficult Airway (2022) - American Society of Anesthesiologists
- Miller's Anesthesia, 10e - Chapter 40, ASA Difficult Airway Algorithm for Adult Patients (Fig. 40.1)
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapter 19, Difficult Airway Algorithm (Fig. 19-29)
- Torossian A. Difficult Airway Management Algorithms - narrative synopsis (2023) - Systematic Review, PMID 36791772
Generate a comparison poster: ASA vs. DAS vs. CAFG difficult airway algorithms
DAS difficult airway society algorithm 2015 steps unanticipated intubation CICO
https://pmc.ncbi.nlm.nih.gov/articles/PMC4650961
CAFG Canadian Airway Focus Group 2021 difficult airway algorithm steps key features
https://pmc.ncbi.nlm.nih.gov/articles/PMC8212585
A detailed medical education comparison poster titled "Difficult Airway Algorithms: ASA vs DAS vs CAFG" designed for MD Anaesthesia exam reference. The poster has a dark navy blue background with clean white and colored text. It is divided into three main columns, one for each society. LEFT COLUMN - ASA 2022 (American Society of Anesthesiologists) in blue: Header: "ASA 2022" with subtitle "Practice Guidelines" Key steps listed as: • PRE-INTUBATION: Assess 6 problems (mask ventilation, SGA, laryngoscopy, intubation, surgical airway, patient cooperation) • Optimize Oxygenation Throughout (HFNO, NIV, head-elevated) • BRANCH A: AWAKE INTUBATION - if suspected difficult laryngoscopy, difficult ventilation, aspiration risk, rapid desaturation risk • BRANCH B: POST-INDUCTION INTUBATION - if no above risks • On failure: Limit attempts, Call for Help • Mask ventilation adequate? → NON-EMERGENCY PATHWAY: consider awakening, alternative techniques • Mask ventilation NOT adequate? → SGA attempt → if SGA fails → EMERGENCY PATHWAY → Emergency Invasive Airway • Confirm every placement with ETCO2 • Document, inform patient, follow-up MIDDLE COLUMN - DAS 2025 (Difficult Airway Society, UK) in green: Header: "DAS 2025" with subtitle "UK Guidelines (Linear Plan A→D)" Key steps listed as: • PLAN A: Tracheal Intubation - Max 3+1 attempts, videolaryngoscope preferred, neuromuscular blockade, apnoeic oxygenation, head-up ramping • PLAN B: Supraglottic Airway Device (SAD/SGA) - 2nd generation preferred, if Plan A fails • PLAN C: Face Mask Ventilation - if SGA fails; if successful → wake patient; if impossible → ensure full paralysis • PLAN D: Emergency Front-of-Neck Airway (eFONA) - scalpel cricothyrotomy (didactic technique), wide-bore cuffed tube, CICO declared • Emphasis: First-pass success, human factors, team briefing, simulation • CICO = Cannot Intubate Cannot Oxygenate RIGHT COLUMN - CAFG 2021 (Canadian Airway Focus Group) in orange/amber: Header: "CAFG 2021" with subtitle "Canadian Consensus" Key steps listed as: • Focus: Anticipation, planning, and physiologically difficult airway • Applies across OR, ICU, ED • UNANTICIPATED DIFFICULT AIRWAY: Use cognitive aid/algorithm • Options: SGA for rescue, temporizing; single further intubation attempt with different technique; OR eFONA • CVCO (Cannot Ventilate Cannot Oxygenate): Confirm NMB → single attempt → eFONA • Limit DL attempts to 2, rapidly move to FB or VL • Call for help EARLY • Strong integration of POCUS for airway assessment • Human factors: avoid freeze/fight/flight response • Post-airway care and extubation planning emphasized BOTTOM COMPARISON TABLE with rows: Row headers | ASA 2022 | DAS 2025 | CAFG 2021 Structure | Decision-tree branches | Linear Plan A→B→C→D | Strategy-based, cognitive aid Setting | OR primarily | OR, RSI | OR, ICU, ED Max intubation attempts | Not specified (limit attempts) | 3+1 | Limit to 2 (DL) VL role | Primary alternative | Strongly recommended | After failed DL SGA (rescue) | Emergency pathway | Plan B | CVCO rescue CICO/CVCO terminology | CICO | CICO | CVCO eFONA technique | Surgical cricothyrotomy | Scalpel cricothyrotomy | eFONA (scalpel preferred) Human factors | Yes (2022 addition) | Strong emphasis | Strong emphasis Oxygenation emphasis | Optimize throughout | Apnoeic oxygenation | Continuous optimization POCUS integration | Limited | Moderate | Strong At the very top of the poster: a bold title bar. At the bottom: small text "Sources: ASA Anesthesiology 2022 | DAS BJA 2025 | CAFG Can J Anesth 2021" The poster uses color-coded columns, clear bold section headers, bullet points, and a clean grid table at the bottom. Professional academic medical poster style, all text clearly readable.
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.