Discuss first pass metabolism pptx
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Running Command
mkdir -p /home/daytona/workspace/first-pass-pptx && ls /home/daytona/workspace/first-pass-pptx/
Writing File
~/first-pass-pptx/generate.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "First Pass Metabolism";
pres.author = "Orris Medical";
// Color palette
const DARK_BG = "1A2340"; // deep navy - title/section slides
const MID_BG = "0F3460"; // mid navy - content slides bg accent
const ACCENT = "E94560"; // vivid red accent
const GOLD = "F5A623"; // gold highlights
const LIGHT_BG = "F4F6FB"; // near-white for content slides
const BODY_TEXT = "1A2340"; // dark text on light bg
const WHITE = "FFFFFF";
const LIGHT_GRAY = "D8DEF0";
const TEAL = "16C8B8"; // teal for process steps
// ─────────────────────────────────────────────
// SLIDE 1 — TITLE
// ─────────────────────────────────────────────
let s1 = pres.addSlide();
s1.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: DARK_BG }, line: { color: DARK_BG } });
// Accent bar
s1.addShape(pres.shapes.RECTANGLE, { x: 0, y: 3.9, w: 10, h: 0.08, fill: { color: ACCENT }, line: { color: ACCENT } });
// Gold left strip
s1.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: GOLD }, line: { color: GOLD } });
s1.addText("FIRST PASS", {
x: 0.35, y: 1.05, w: 9.3, h: 0.9,
fontSize: 52, bold: true, color: WHITE, fontFace: "Calibri", align: "left",
charSpacing: 8
});
s1.addText("METABOLISM", {
x: 0.35, y: 1.95, w: 9.3, h: 0.9,
fontSize: 52, bold: true, color: ACCENT, fontFace: "Calibri", align: "left",
charSpacing: 8
});
s1.addText("Definition | Mechanism | Clinical Significance | Drug Examples", {
x: 0.35, y: 3.05, w: 9.3, h: 0.5,
fontSize: 15, color: LIGHT_GRAY, fontFace: "Calibri", align: "left", italic: true
});
s1.addText("Pharmacokinetics Series", {
x: 0.35, y: 4.1, w: 9, h: 0.4,
fontSize: 12, color: GOLD, fontFace: "Calibri", align: "left"
});
s1.addText("Sources: Lippincott Pharmacology | Katzung | Goodman & Gilman", {
x: 0.35, y: 4.9, w: 9, h: 0.35,
fontSize: 9, color: LIGHT_GRAY, fontFace: "Calibri", align: "left", italic: true
});
// ─────────────────────────────────────────────
// SLIDE 2 — OVERVIEW / LEARNING OBJECTIVES
// ─────────────────────────────────────────────
let s2 = pres.addSlide();
s2.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: LIGHT_BG }, line: { color: LIGHT_BG } });
s2.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: ACCENT }, line: { color: ACCENT } });
s2.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 1.0, fill: { color: DARK_BG }, line: { color: DARK_BG } });
s2.addText("LEARNING OBJECTIVES", {
x: 0.35, y: 0.15, w: 9.3, h: 0.65,
fontSize: 24, bold: true, color: WHITE, fontFace: "Calibri"
});
const objectives = [
"Define first-pass metabolism and distinguish it from systemic metabolism",
"Describe the anatomical basis: portal circulation and hepatic extraction",
"Calculate extraction ratio and relate it to oral bioavailability",
"Identify drugs with high and low first-pass effect",
"Explain routes of administration that bypass first-pass metabolism",
"Apply clinical consequences of first-pass effect in disease states"
];
s2.addText(objectives.map((o, i) => [
{ text: `${i + 1}. `, options: { bold: true, color: ACCENT } },
{ text: o + "\n", options: { color: BODY_TEXT } }
]).flat(), {
x: 0.4, y: 1.15, w: 9.2, h: 4.2,
fontSize: 15, fontFace: "Calibri", lineSpacingMultiple: 1.3
});
// ─────────────────────────────────────────────
// SLIDE 3 — DEFINITION
// ─────────────────────────────────────────────
let s3 = pres.addSlide();
s3.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: LIGHT_BG }, line: { color: LIGHT_BG } });
s3.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 1.0, fill: { color: MID_BG }, line: { color: MID_BG } });
s3.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: GOLD }, line: { color: GOLD } });
s3.addText("DEFINITION", {
x: 0.35, y: 0.18, w: 9.3, h: 0.6,
fontSize: 26, bold: true, color: WHITE, fontFace: "Calibri"
});
// Definition box
s3.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.4, y: 1.15, w: 9.2, h: 1.35,
fill: { color: DARK_BG }, line: { color: ACCENT }, rectRadius: 0.1
});
s3.addText("When a drug is absorbed from the GI tract, it enters the portal circulation before entering the systemic circulation. If the drug is rapidly metabolized in the liver or gut wall during this initial passage, the amount of unchanged drug reaching the systemic circulation is decreased.", {
x: 0.55, y: 1.25, w: 8.9, h: 1.15,
fontSize: 14, color: WHITE, fontFace: "Calibri", italic: true, lineSpacingMultiple: 1.4
});
s3.addText([
{ text: "Also called: ", options: { bold: true, color: ACCENT } },
{ text: "Presystemic elimination / hepatic first-pass effect / presystemic metabolism\n", options: { color: BODY_TEXT } },
{ text: "\nKey Point: ", options: { bold: true, color: ACCENT } },
{ text: "Orally administered drugs must traverse the gut wall and liver via the portal vein BEFORE entering systemic circulation. This reduces the fraction of drug available to act at target tissues.", options: { color: BODY_TEXT } }
], {
x: 0.4, y: 2.65, w: 9.2, h: 2.6,
fontSize: 14, fontFace: "Calibri", lineSpacingMultiple: 1.4
});
// ─────────────────────────────────────────────
// SLIDE 4 — ANATOMICAL PATHWAY (Process Flow)
// ─────────────────────────────────────────────
let s4 = pres.addSlide();
s4.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: LIGHT_BG }, line: { color: LIGHT_BG } });
s4.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 1.0, fill: { color: DARK_BG }, line: { color: DARK_BG } });
s4.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: TEAL }, line: { color: TEAL } });
s4.addText("ANATOMICAL PATHWAY OF FIRST-PASS METABOLISM", {
x: 0.35, y: 0.18, w: 9.3, h: 0.6,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri"
});
// Process steps
const steps = [
{ label: "1", title: "Oral Ingestion", desc: "Drug swallowed as tablet/capsule/liquid" },
{ label: "2", title: "GI Absorption", desc: "Drug absorbed across intestinal epithelium; partial gut-wall metabolism by CYP3A4" },
{ label: "3", title: "Portal Vein", desc: "Drug enters mesenteric capillaries → portal vein → travels to liver" },
{ label: "4", title: "Hepatic Extraction", desc: "Liver enzymes (CYP450, conjugation) metabolize a fraction of the drug" },
{ label: "5", title: "Systemic Circulation", desc: "Only remaining unmetabolized drug reaches general circulation and target organs" }
];
const stepColors = [TEAL, GOLD, ACCENT, "9B59B6", MID_BG];
const xStart = 0.25;
const boxW = 1.72;
const gap = 0.04;
steps.forEach((step, i) => {
const x = xStart + i * (boxW + gap);
s4.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y: 1.1, w: boxW, h: 3.8,
fill: { color: stepColors[i] }, line: { color: stepColors[i] }, rectRadius: 0.08
});
s4.addText(step.label, {
x, y: 1.2, w: boxW, h: 0.55,
fontSize: 28, bold: true, color: WHITE, fontFace: "Calibri", align: "center"
});
s4.addText(step.title, {
x: x + 0.05, y: 1.85, w: boxW - 0.1, h: 0.6,
fontSize: 13, bold: true, color: WHITE, fontFace: "Calibri", align: "center"
});
s4.addText(step.desc, {
x: x + 0.08, y: 2.55, w: boxW - 0.16, h: 2.1,
fontSize: 11.5, color: WHITE, fontFace: "Calibri", align: "center", lineSpacingMultiple: 1.3
});
});
// Arrows between boxes
for (let i = 0; i < 4; i++) {
const x = xStart + (i + 1) * (boxW + gap) - 0.05;
s4.addText("→", {
x: x - 0.15, y: 2.4, w: 0.3, h: 0.5,
fontSize: 22, bold: true, color: ACCENT, fontFace: "Calibri", align: "center"
});
}
s4.addText("Bioavailability (F) = Fraction of administered dose reaching systemic circulation unchanged", {
x: 0.25, y: 5.05, w: 9.5, h: 0.45,
fontSize: 11.5, italic: true, color: MID_BG, fontFace: "Calibri", align: "center"
});
// ─────────────────────────────────────────────
// SLIDE 5 — BIOAVAILABILITY & EXTRACTION RATIO
// ─────────────────────────────────────────────
let s5 = pres.addSlide();
s5.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: LIGHT_BG }, line: { color: LIGHT_BG } });
s5.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 1.0, fill: { color: ACCENT }, line: { color: ACCENT } });
s5.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: DARK_BG }, line: { color: DARK_BG } });
s5.addText("BIOAVAILABILITY & EXTRACTION RATIO", {
x: 0.35, y: 0.18, w: 9.3, h: 0.6,
fontSize: 24, bold: true, color: WHITE, fontFace: "Calibri"
});
// Left panel
s5.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.25, y: 1.1, w: 4.45, h: 4.25,
fill: { color: DARK_BG }, line: { color: GOLD }, rectRadius: 0.08
});
s5.addText("BIOAVAILABILITY (F)", {
x: 0.35, y: 1.2, w: 4.25, h: 0.5,
fontSize: 15, bold: true, color: GOLD, fontFace: "Calibri", align: "center"
});
s5.addText([
{ text: "F = AUC(oral) / AUC(IV)\n\n", options: { bold: true, fontSize: 17, color: TEAL } },
{ text: "• IV administration = 100% bioavailability\n\n", options: { color: WHITE, fontSize: 13 } },
{ text: "• Oral bioavailability < 100% due to:\n - Incomplete absorption\n - Gut wall metabolism\n - Hepatic first-pass metabolism\n\n", options: { color: WHITE, fontSize: 13 } },
{ text: "Example: Nitroglycerin F < 10% orally\n(>90% cleared in first pass)", options: { color: GOLD, fontSize: 12, italic: true } }
], {
x: 0.35, y: 1.8, w: 4.25, h: 3.3,
fontFace: "Calibri", lineSpacingMultiple: 1.35
});
// Right panel
s5.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 5.0, y: 1.1, w: 4.75, h: 4.25,
fill: { color: MID_BG }, line: { color: TEAL }, rectRadius: 0.08
});
s5.addText("EXTRACTION RATIO (ER)", {
x: 5.1, y: 1.2, w: 4.55, h: 0.5,
fontSize: 15, bold: true, color: TEAL, fontFace: "Calibri", align: "center"
});
s5.addText([
{ text: "ER = (C_in - C_out) / C_in\n\n", options: { bold: true, fontSize: 17, color: GOLD } },
{ text: "• High ER (>0.7): ", options: { bold: true, color: WHITE, fontSize: 13 } },
{ text: "Propranolol, morphine, lidocaine, verapamil, isoniazid\n → Extensive first-pass, low oral bioavailability\n\n", options: { color: LIGHT_GRAY, fontSize: 12 } },
{ text: "• Low ER (<0.3): ", options: { bold: true, color: WHITE, fontSize: 13 } },
{ text: "Warfarin, diazepam, phenytoin, theophylline\n → Minimal first-pass, high oral bioavailability\n\n", options: { color: LIGHT_GRAY, fontSize: 12 } },
{ text: "F = 1 - ER\n(for hepatically cleared drugs)", options: { bold: true, color: GOLD, fontSize: 13, italic: true } }
], {
x: 5.1, y: 1.8, w: 4.55, h: 3.3,
fontFace: "Calibri", lineSpacingMultiple: 1.3
});
// ─────────────────────────────────────────────
// SLIDE 6 — SITES & ENZYMES
// ─────────────────────────────────────────────
let s6 = pres.addSlide();
s6.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: LIGHT_BG }, line: { color: LIGHT_BG } });
s6.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 1.0, fill: { color: MID_BG }, line: { color: MID_BG } });
s6.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: ACCENT }, line: { color: ACCENT } });
s6.addText("SITES & ENZYMES INVOLVED", {
x: 0.35, y: 0.18, w: 9.3, h: 0.6,
fontSize: 26, bold: true, color: WHITE, fontFace: "Calibri"
});
const sites = [
{
title: "Gut Wall (Enterocytes)",
color: TEAL,
points: [
"CYP3A4 is abundantly expressed in intestinal epithelium",
"Phase I oxidation/reduction reactions",
"P-glycoprotein (P-gp) efflux transporter pumps drug back into gut lumen",
"Example: Cyclosporine, midazolam - extensive gut wall metabolism"
]
},
{
title: "Liver (Hepatocytes)",
color: GOLD,
points: [
"Primary site of first-pass metabolism",
"Phase I: CYP1A2, CYP2C9, CYP2D6, CYP3A4 - oxidation/reduction/hydrolysis",
"Phase II: Glucuronidation, sulfation, acetylation, methylation",
"Depends on hepatic blood flow and enzyme activity"
]
},
{
title: "Lung (Pulmonary)",
color: ACCENT,
points: [
"First-pass site for IV/parenteral drugs",
"Particularly relevant for lipophilic and basic drugs",
"MAO present - metabolizes catecholamines and tyramine",
"Less significant than hepatic first-pass for oral drugs"
]
}
];
sites.forEach((site, i) => {
const x = 0.25 + i * 3.25;
s6.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y: 1.1, w: 3.1, h: 4.3,
fill: { color: "FFFFFF" }, line: { color: site.color, pt: 2 }, rectRadius: 0.08
});
s6.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y: 1.1, w: 3.1, h: 0.55,
fill: { color: site.color }, line: { color: site.color }, rectRadius: 0.08
});
s6.addText(site.title, {
x, y: 1.15, w: 3.1, h: 0.45,
fontSize: 13.5, bold: true, color: WHITE, fontFace: "Calibri", align: "center"
});
s6.addText(site.points.map(p => ({ text: "• " + p + "\n", options: { color: BODY_TEXT } })), {
x: x + 0.12, y: 1.75, w: 2.88, h: 3.5,
fontSize: 12, fontFace: "Calibri", lineSpacingMultiple: 1.35
});
});
// ─────────────────────────────────────────────
// SLIDE 7 — DRUGS WITH HIGH FIRST-PASS
// ─────────────────────────────────────────────
let s7 = pres.addSlide();
s7.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: LIGHT_BG }, line: { color: LIGHT_BG } });
s7.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 1.0, fill: { color: DARK_BG }, line: { color: DARK_BG } });
s7.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: GOLD }, line: { color: GOLD } });
s7.addText("DRUGS WITH HIGH FIRST-PASS EFFECT", {
x: 0.35, y: 0.18, w: 9.3, h: 0.6,
fontSize: 24, bold: true, color: WHITE, fontFace: "Calibri"
});
// Table header
const tableHeaders = ["Drug", "Class", "Oral Bioavailability", "Clinical Note"];
const colWidths = [2.0, 2.2, 2.2, 3.3];
const colX = [0.22, 2.22, 4.42, 6.62];
const rowH = 0.48;
const tableY = 1.05;
// Header row
colX.forEach((x, i) => {
s7.addShape(pres.shapes.RECTANGLE, {
x, y: tableY, w: colWidths[i], h: 0.5,
fill: { color: ACCENT }, line: { color: ACCENT }
});
s7.addText(tableHeaders[i], {
x: x + 0.05, y: tableY + 0.08, w: colWidths[i] - 0.1, h: 0.35,
fontSize: 12.5, bold: true, color: WHITE, fontFace: "Calibri", align: "center"
});
});
// Table rows
const drugs = [
["Nitroglycerin", "Antianginal", "< 10%", "Sublingual/transdermal/IV preferred"],
["Morphine", "Opioid analgesic", "~20-40%", "Higher oral doses needed vs IV"],
["Lidocaine", "Antiarrhythmic", "~35%", "Not given orally (toxic metabolites)"],
["Propranolol", "Beta-blocker", "~25%", "High individual variability"],
["Verapamil", "CCB / antiarrhythmic", "~20-35%", "Extensive hepatic CYP3A4 metabolism"],
["Isoniazid", "Antitubercular", "Variable", "Acetylator phenotype dependent"],
["Naloxone", "Opioid antagonist", "< 2%", "IV/IM/intranasal only"],
["Testosterone", "Hormone", "< 10%", "Requires esterification for oral use"]
];
drugs.forEach((row, ri) => {
const y = tableY + 0.5 + ri * rowH;
const rowColor = ri % 2 === 0 ? "FFFFFF" : "EBF0FB";
colX.forEach((x, ci) => {
s7.addShape(pres.shapes.RECTANGLE, {
x, y, w: colWidths[ci], h: rowH,
fill: { color: rowColor }, line: { color: LIGHT_GRAY }
});
s7.addText(row[ci], {
x: x + 0.06, y: y + 0.06, w: colWidths[ci] - 0.12, h: rowH - 0.1,
fontSize: 11, color: BODY_TEXT, fontFace: "Calibri", align: ci === 0 ? "left" : "center",
bold: ci === 0
});
});
});
// ─────────────────────────────────────────────
// SLIDE 8 — ROUTES BYPASSING FIRST PASS
// ─────────────────────────────────────────────
let s8 = pres.addSlide();
s8.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: LIGHT_BG }, line: { color: LIGHT_BG } });
s8.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 1.0, fill: { color: TEAL }, line: { color: TEAL } });
s8.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: MID_BG }, line: { color: MID_BG } });
s8.addText("ROUTES THAT BYPASS FIRST-PASS METABOLISM", {
x: 0.35, y: 0.18, w: 9.3, h: 0.6,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri"
});
const routes = [
{ route: "Sublingual / Buccal", extent: "Complete bypass", color: TEAL, detail: "Absorbed directly into systemic veins (not portal). Classic example: Sublingual nitroglycerin for angina. Rapid onset (2-5 min)." },
{ route: "Intravenous (IV)", extent: "Complete bypass", color: GOLD, detail: "100% bioavailability - no absorption barrier or first-pass. Drug enters systemic circulation directly." },
{ route: "Transdermal", extent: "Complete bypass", color: ACCENT, detail: "Skin absorption → systemic veins. Used for nitroglycerin patches, fentanyl patches, scopolamine." },
{ route: "Inhalation", extent: "Bypasses hepatic FPM*", color: "9B59B6", detail: "Avoids hepatic first-pass but lung may metabolize drugs. Salbutamol, corticosteroids. *Pulmonary first-pass possible." },
{ route: "Rectal (lower)", extent: "~50% bypass", color: MID_BG, detail: "Inferior rectal veins → IVC (bypasses liver). Upper rectal veins drain to portal. Only ~50% reliably bypasses first-pass." },
{ route: "Intramuscular / SC", extent: "Complete bypass", color: "2E7D32", detail: "Drug enters systemic circulation via capillary absorption. No portal circulation transit. Used for many hormones and vaccines." }
];
const cols = 3;
routes.forEach((r, i) => {
const col = i % cols;
const row = Math.floor(i / cols);
const x = 0.22 + col * 3.25;
const y = 1.1 + row * 2.2;
s8.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w: 3.1, h: 2.0,
fill: { color: "FFFFFF" }, line: { color: r.color, pt: 2 }, rectRadius: 0.08
});
s8.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w: 3.1, h: 0.48,
fill: { color: r.color }, line: { color: r.color }, rectRadius: 0.08
});
s8.addText(r.route, {
x: x + 0.05, y: y + 0.06, w: 3.0, h: 0.35,
fontSize: 12.5, bold: true, color: WHITE, fontFace: "Calibri", align: "center"
});
s8.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: x + 0.08, y: y + 0.55, w: 2.94, h: 0.28,
fill: { color: r.color + "33" }, line: { color: r.color + "55" }, rectRadius: 0.04
});
s8.addText(r.extent, {
x: x + 0.08, y: y + 0.56, w: 2.94, h: 0.26,
fontSize: 10, bold: true, color: r.color, fontFace: "Calibri", align: "center"
});
s8.addText(r.detail, {
x: x + 0.1, y: y + 0.9, w: 2.9, h: 1.0,
fontSize: 11, color: BODY_TEXT, fontFace: "Calibri", lineSpacingMultiple: 1.25
});
});
// ─────────────────────────────────────────────
// SLIDE 9 — CLINICAL CONSEQUENCES
// ─────────────────────────────────────────────
let s9 = pres.addSlide();
s9.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: LIGHT_BG }, line: { color: LIGHT_BG } });
s9.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 1.0, fill: { color: DARK_BG }, line: { color: DARK_BG } });
s9.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: ACCENT }, line: { color: ACCENT } });
s9.addText("CLINICAL CONSEQUENCES", {
x: 0.35, y: 0.18, w: 9.3, h: 0.6,
fontSize: 26, bold: true, color: WHITE, fontFace: "Calibri"
});
// Two columns
// Left
s9.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.25, y: 1.1, w: 4.6, h: 4.25,
fill: { color: DARK_BG }, line: { color: GOLD, pt: 1.5 }, rectRadius: 0.08
});
s9.addText("LIVER DISEASE (Cirrhosis)", {
x: 0.35, y: 1.2, w: 4.4, h: 0.45,
fontSize: 14.5, bold: true, color: GOLD, fontFace: "Calibri", align: "center"
});
s9.addText([
{ text: "• Portosystemic shunting bypasses liver → dramatically increases oral bioavailability of high-ER drugs\n\n", options: { color: WHITE, fontSize: 12.5 } },
{ text: "• Morphine, meperidine, midazolam, nifedipine: bioavailability nearly doubles in cirrhosis\n\n", options: { color: LIGHT_GRAY, fontSize: 12 } },
{ text: "• Propranolol bioavailability may increase 3-5x → risk of bradycardia/hypotension\n\n", options: { color: LIGHT_GRAY, fontSize: 12 } },
{ text: "Action: ", options: { bold: true, color: GOLD, fontSize: 13 } },
{ text: "Reduce doses of high first-pass drugs in liver disease patients", options: { color: WHITE, fontSize: 12.5 } }
], {
x: 0.35, y: 1.75, w: 4.4, h: 3.4,
fontFace: "Calibri", lineSpacingMultiple: 1.3
});
// Right
s9.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 5.15, y: 1.1, w: 4.6, h: 4.25,
fill: { color: MID_BG }, line: { color: TEAL, pt: 1.5 }, rectRadius: 0.08
});
s9.addText("DRUG DOSING IMPLICATIONS", {
x: 5.25, y: 1.2, w: 4.4, h: 0.45,
fontSize: 14.5, bold: true, color: TEAL, fontFace: "Calibri", align: "center"
});
s9.addText([
{ text: "• Oral doses must be higher than IV doses for high first-pass drugs to achieve equivalent effect\n\n", options: { color: WHITE, fontSize: 12.5 } },
{ text: "• Inter-individual variability: genetic differences in CYP2D6 (poor/extensive metabolizers) significantly alter first-pass\n\n", options: { color: LIGHT_GRAY, fontSize: 12 } },
{ text: "• Enzyme inducers (rifampicin, carbamazepine) increase first-pass → reduce bioavailability\n\n", options: { color: LIGHT_GRAY, fontSize: 12 } },
{ text: "• Enzyme inhibitors (clarithromycin, grapefruit juice CYP3A4) reduce first-pass → increase bioavailability → toxicity risk", options: { color: LIGHT_GRAY, fontSize: 12 } }
], {
x: 5.25, y: 1.75, w: 4.4, h: 3.4,
fontFace: "Calibri", lineSpacingMultiple: 1.3
});
// ─────────────────────────────────────────────
// SLIDE 10 — PRODRUGS
// ─────────────────────────────────────────────
let s10 = pres.addSlide();
s10.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: LIGHT_BG }, line: { color: LIGHT_BG } });
s10.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 1.0, fill: { color: ACCENT }, line: { color: ACCENT } });
s10.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: GOLD }, line: { color: GOLD } });
s10.addText("PRODRUGS: EXPLOITING FIRST-PASS METABOLISM", {
x: 0.35, y: 0.18, w: 9.3, h: 0.6,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri"
});
s10.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.25, y: 1.1, w: 9.5, h: 1.2,
fill: { color: DARK_BG }, line: { color: GOLD }, rectRadius: 0.08
});
s10.addText("A prodrug is an inactive compound that is converted to its active form during first-pass metabolism. This strategy is used to improve oral bioavailability, absorption, stability, or palatability.", {
x: 0.4, y: 1.2, w: 9.2, h: 1.0,
fontSize: 14, color: WHITE, fontFace: "Calibri", italic: true, lineSpacingMultiple: 1.4
});
const prodrugs = [
{ prodrug: "Enalapril", active: "Enalaprilat", class: "ACE inhibitor", note: "Oral ester prodrug; hepatic hydrolysis to active form" },
{ prodrug: "Codeine", active: "Morphine", class: "Opioid analgesic", note: "CYP2D6 O-demethylation; poor metabolizers may lack effect" },
{ prodrug: "Levodopa", active: "Dopamine", class: "Antiparkinsonian", note: "Decarboxylated to dopamine in brain (+ periphery)" },
{ prodrug: "Clopidogrel", active: "Active thiol", class: "Antiplatelet", note: "CYP2C19 activation; loss-of-function allele = resistance" },
{ prodrug: "Prednisone", active: "Prednisolone", class: "Corticosteroid", note: "Hepatic reduction to active prednisolone" }
];
const ph = ["Prodrug", "Active Metabolite", "Drug Class", "Mechanism / Note"];
const pw = [2.0, 2.1, 2.2, 3.45];
const px = [0.25, 2.25, 4.35, 6.55];
const pTableY = 2.45;
px.forEach((x, i) => {
s10.addShape(pres.shapes.RECTANGLE, {
x, y: pTableY, w: pw[i], h: 0.45,
fill: { color: MID_BG }, line: { color: MID_BG }
});
s10.addText(ph[i], {
x: x + 0.05, y: pTableY + 0.06, w: pw[i] - 0.1, h: 0.33,
fontSize: 12, bold: true, color: WHITE, fontFace: "Calibri", align: "center"
});
});
prodrugs.forEach((row, ri) => {
const y = pTableY + 0.45 + ri * 0.42;
const bg = ri % 2 === 0 ? "FFFFFF" : "EBF0FB";
const vals = [row.prodrug, row.active, row.class, row.note];
px.forEach((x, ci) => {
s10.addShape(pres.shapes.RECTANGLE, {
x, y, w: pw[ci], h: 0.42,
fill: { color: bg }, line: { color: LIGHT_GRAY }
});
s10.addText(vals[ci], {
x: x + 0.05, y: y + 0.05, w: pw[ci] - 0.1, h: 0.33,
fontSize: 11, color: BODY_TEXT, fontFace: "Calibri",
bold: ci === 0, align: ci === 0 ? "left" : "center"
});
});
});
// ─────────────────────────────────────────────
// SLIDE 11 — FACTORS AFFECTING FIRST-PASS
// ─────────────────────────────────────────────
let s11 = pres.addSlide();
s11.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: LIGHT_BG }, line: { color: LIGHT_BG } });
s11.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 1.0, fill: { color: MID_BG }, line: { color: MID_BG } });
s11.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: TEAL }, line: { color: TEAL } });
s11.addText("FACTORS AFFECTING FIRST-PASS METABOLISM", {
x: 0.35, y: 0.18, w: 9.3, h: 0.6,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri"
});
const factors = [
{
title: "Genetic / Pharmacogenomics",
color: TEAL,
items: ["CYP2D6 polymorphisms: poor vs. ultra-rapid metabolizers", "CYP2C19 variants affect clopidogrel, omeprazole", "Acetylator status (NAT2): isoniazid metabolism"]
},
{
title: "Disease States",
color: ACCENT,
items: ["Liver cirrhosis: reduced enzyme activity + portosystemic shunts", "Congestive heart failure: reduced hepatic blood flow", "Inflammatory bowel disease: altered gut wall metabolism"]
},
{
title: "Drug Interactions",
color: GOLD,
items: ["Enzyme inducers: rifampicin, carbamazepine, phenytoin - ↑ first-pass", "Enzyme inhibitors: clarithromycin, azoles, grapefruit juice - ↓ first-pass", "P-gp inhibitors (e.g., quinidine) - ↑ absorption through gut wall"]
},
{
title: "Physiological Factors",
color: MID_BG,
items: ["Age: neonates/elderly have reduced CYP450 activity", "Sex differences: CYP3A4 activity higher in women", "Food effects: high-fat meals can alter portal blood flow and absorption"]
}
];
const factorCols = 2;
factors.forEach((f, i) => {
const col = i % factorCols;
const row = Math.floor(i / factorCols);
const x = 0.22 + col * 4.88;
const y = 1.08 + row * 2.3;
s11.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w: 4.63, h: 2.15,
fill: { color: "FFFFFF" }, line: { color: f.color, pt: 2 }, rectRadius: 0.08
});
s11.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w: 4.63, h: 0.48,
fill: { color: f.color }, line: { color: f.color }, rectRadius: 0.08
});
s11.addText(f.title, {
x: x + 0.08, y: y + 0.07, w: 4.47, h: 0.35,
fontSize: 13.5, bold: true, color: WHITE, fontFace: "Calibri", align: "center"
});
s11.addText(f.items.map(item => ({ text: "• " + item + "\n", options: { color: BODY_TEXT } })), {
x: x + 0.12, y: y + 0.58, w: 4.4, h: 1.5,
fontSize: 12, fontFace: "Calibri", lineSpacingMultiple: 1.3
});
});
// ─────────────────────────────────────────────
// SLIDE 12 — SUMMARY / KEY POINTS
// ─────────────────────────────────────────────
let s12 = pres.addSlide();
s12.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: DARK_BG }, line: { color: DARK_BG } });
s12.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.2, w: 10, h: 0.425, fill: { color: ACCENT }, line: { color: ACCENT } });
s12.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: GOLD }, line: { color: GOLD } });
s12.addText("KEY TAKEAWAYS", {
x: 0.35, y: 0.2, w: 9.3, h: 0.65,
fontSize: 32, bold: true, color: WHITE, fontFace: "Calibri", charSpacing: 4
});
s12.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 0.9, w: 9.3, h: 0.05, fill: { color: ACCENT }, line: { color: ACCENT } });
const keyPoints = [
{ n: "1", t: "Definition", b: "First-pass metabolism = presystemic elimination of orally ingested drug before reaching systemic circulation, occurring in the gut wall and/or liver." },
{ n: "2", t: "Portal Circulation", b: "Oral drugs travel from GI tract → portal vein → liver before entering systemic blood. This is the anatomical basis of first-pass effect." },
{ n: "3", t: "Bioavailability Impact", b: "High extraction ratio drugs (morphine, lidocaine, nitroglycerin, propranolol) have markedly reduced oral bioavailability. F = 1 − ER." },
{ n: "4", t: "Bypass Routes", b: "Sublingual, transdermal, IV, IM/SC routes bypass hepatic first-pass. Rectal bypasses ~50%. Inhalation bypasses hepatic but not pulmonary first-pass." },
{ n: "5", t: "Clinical Relevance", b: "Liver disease, enzyme polymorphisms, and drug interactions all alter first-pass magnitude. Adjust doses accordingly." }
];
keyPoints.forEach((kp, i) => {
const y = 1.05 + i * 0.88;
s12.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.25, y, w: 0.5, h: 0.65,
fill: { color: ACCENT }, line: { color: ACCENT }, rectRadius: 0.06
});
s12.addText(kp.n, {
x: 0.25, y: y + 0.1, w: 0.5, h: 0.45,
fontSize: 18, bold: true, color: WHITE, fontFace: "Calibri", align: "center"
});
s12.addText([
{ text: kp.t + ": ", options: { bold: true, color: GOLD } },
{ text: kp.b, options: { color: LIGHT_GRAY } }
], {
x: 0.9, y: y + 0.05, w: 8.85, h: 0.7,
fontSize: 13, fontFace: "Calibri", lineSpacingMultiple: 1.3
});
});
s12.addText("Lippincott Pharmacology | Katzung's Basic & Clinical Pharmacology | Goodman & Gilman | Harrison's IM", {
x: 0.25, y: 5.22, w: 9.5, h: 0.35,
fontSize: 10, color: WHITE, fontFace: "Calibri", align: "center", italic: true
});
// ─── SAVE ───
pres.writeFile({ fileName: "/home/daytona/workspace/first-pass-pptx/First_Pass_Metabolism.pptx" })
.then(() => console.log("DONE: First_Pass_Metabolism.pptx created"))
.catch(e => { console.error(e); process.exit(1); });
Running Command
cd /home/daytona/workspace/first-pass-pptx && node generate.js 2>&1
Editing File
~/first-pass-pptx/generate.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/first-pass-pptx/generate.js'
Running Command
cd /home/daytona/workspace/first-pass-pptx && node generate.js 2>&1
Your presentation is ready:
First Pass Metabolism
Presentation · PPTX
What's Inside (12 Slides)
| Slide | Content |
|---|---|
| 1 | Title Slide - Bold navy/red design |
| 2 | Learning Objectives - 6 key goals |
| 3 | Definition - Presystemic elimination explained with textbook-quoted definition |
| 4 | Anatomical Pathway - 5-step process flow: Oral ingestion → GI absorption → Portal vein → Hepatic extraction → Systemic circulation |
| 5 | Bioavailability & Extraction Ratio - Formula panels: F = AUC(oral)/AUC(IV) and ER = (C_in - C_out)/C_in, with drug examples |
| 6 | Sites & Enzymes - Gut wall (CYP3A4, P-gp), Liver (Phase I & II), Lung (pulmonary first-pass) |
| 7 | High First-Pass Drugs Table - Nitroglycerin, Morphine, Lidocaine, Propranolol, Verapamil, Isoniazid, Naloxone, Testosterone |
| 8 | Bypass Routes - Sublingual, IV, Transdermal, Inhalation, Rectal, IM/SC with bypass extent for each |
| 9 | Clinical Consequences - Liver disease (cirrhosis) effects + dosing implications, enzyme inducers/inhibitors |
| 10 | Prodrugs - Enalapril, Codeine, Levodopa, Clopidogrel, Prednisone with activation mechanisms |
| 11 | Factors Affecting First-Pass - Genetics, disease states, drug interactions, physiological factors |
| 12 | Key Takeaways - 5 high-yield summary points |
Sources: Lippincott Pharmacology, Katzung's Basic & Clinical Pharmacology, Goodman & Gilman's, Harrison's Internal Medicine.
Comprehensive notes on first pass metabolism
Finding Sources
Searching PubMed
"first pass metabolism" AND bioavailability
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive content from all major sources. Here are the complete notes:
First Pass Metabolism - Comprehensive Notes
1. Definition & Terminology
First-pass metabolism (also called presystemic elimination or the first-pass effect) refers to the biotransformation of an orally administered drug that occurs before it reaches the systemic circulation. When a drug is absorbed from the GI tract, it enters the portal circulation and passes through the liver before reaching any other tissue. If the drug is rapidly metabolized during this initial passage - in the gut wall or liver - the amount of unchanged (active) drug entering the systemic circulation is reduced.
"Some drugs that are administered orally are absorbed relatively efficiently into the portal circulation but are metabolized by the liver before they reach the systemic circulation. Because of this 'first-pass' or 'presystemic' effect, the oral route may be less suitable than other routes of administration for such drugs."
- Goldman-Cecil Medicine
2. Anatomical Basis
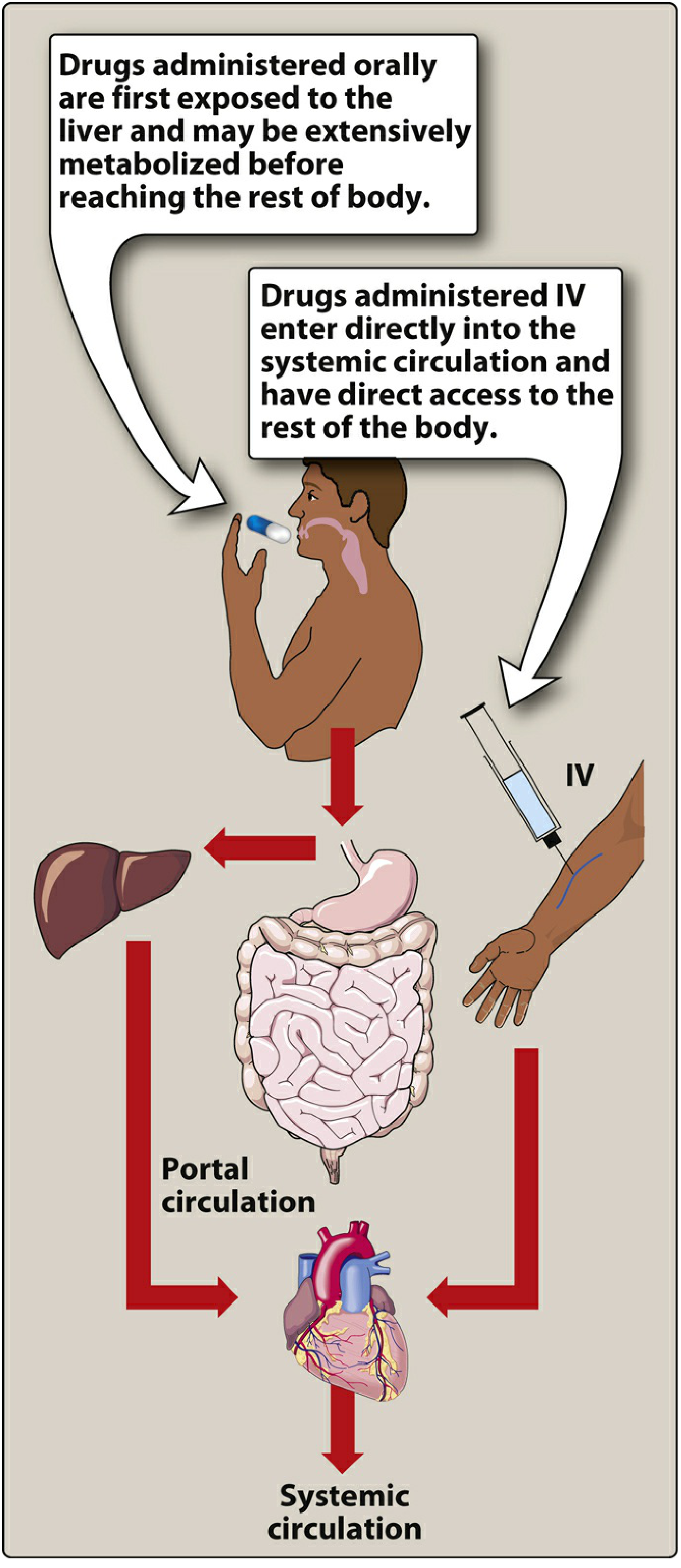
Figure: Oral drugs pass through the portal circulation to the liver before entering systemic circulation, while IV drugs bypass this pathway entirely. - Lippincott Pharmacology, Fig. 1.11
The complete pathway for an oral drug is:
Oral ingestion
↓
GI lumen (dissolution)
↓
Intestinal epithelium (gut wall metabolism, P-gp efflux)
↓
Mesenteric capillaries → Portal vein
↓
Liver (Phase I & II metabolism)
↓
Hepatic veins → Inferior vena cava
↓
Systemic circulation (heart → target organs)
By contrast, IV-administered drugs enter directly into the systemic circulation, bypassing this entire pathway and achieving 100% bioavailability.
3. Sites of First-Pass Metabolism
3.1 Gut Wall (Enterocytes)
- CYP3A4 is highly expressed in intestinal enterocytes and is responsible for significant presystemic metabolism of many drugs (e.g., cyclosporine, midazolam, felodipine).
- P-glycoprotein (P-gp), an efflux transporter, pumps absorbed drug molecules back into the intestinal lumen, reducing net absorption and contributing to first-pass loss. P-gp inhibitors (e.g., quinidine, grapefruit juice) can dramatically increase bioavailability.
- UDP-glucuronosyltransferases (UGTs) in the gut wall also contribute to conjugation reactions.
3.2 Liver (Primary Site)
- The liver receives the portal blood directly and contains the highest concentration of drug-metabolizing enzymes.
- Phase I reactions: Oxidation, reduction, and hydrolysis via cytochrome P450 enzymes (CYP1A2, CYP2C9, CYP2C19, CYP2D6, CYP3A4).
- Phase II reactions: Glucuronidation, sulfation, acetylation, methylation - conjugation reactions that generally render metabolites more water-soluble and inactive (though some conjugates remain active).
- The degree of hepatic first-pass depends on intrinsic clearance (CL_i) - the liver's inherent enzyme capacity - and hepatic blood flow (Q).
3.3 Lung (Pulmonary First-Pass)
- Relevant primarily for drugs administered via non-oral parenteral routes (IV, transdermal).
- Monoamine oxidase (MAO) in the lung degrades catecholamines and tyramine.
- "Although drugs administered by inhalation bypass the hepatic first-pass effect, the lung may also serve as a site of first-pass loss by excretion and possibly metabolism for drugs administered by nongastrointestinal routes." - Katzung's
4. Bioavailability and the First-Pass Effect
Bioavailability (F) is the fraction of an administered dose that reaches the systemic circulation unchanged.
$$F = \frac{AUC_{oral}}{AUC_{IV}} \times 100%$$
- IV administration: F = 100% (by definition)
- Oral administration: F < 100% due to incomplete absorption AND first-pass metabolism
When first-pass metabolism is significant, the modified steady-state equation becomes:
$$F \times \text{Dosing rate} = CL \times C_{ss}$$
This means oral doses must be proportionally higher than IV doses to achieve equivalent plasma concentrations.
Classic example: Nitroglycerin is well absorbed but >90% is cleared during hepatic first-pass. It cannot be given orally in standard doses; sublingual or transdermal routes are required.
5. Extraction Ratio (ER)
The extraction ratio is the fraction of drug removed from the blood during a single pass through the liver:
$$ER = \frac{C_{in} - C_{out}}{C_{in}}$$
Where C_in = drug concentration entering the liver (portal vein), C_out = drug concentration leaving (hepatic vein).
Hepatic clearance is related to hepatic blood flow and ER:
$$CL_H = Q \times ER = Q \times \left(\frac{CL_i}{Q + CL_i}\right)$$
Where Q = hepatic blood flow (~1.5 L/min), CL_i = intrinsic clearance.
Classification by Extraction Ratio
| Category | ER | Bioavailability | Key Determinant | Examples |
|---|---|---|---|---|
| High ER | > 0.7 | Low (< 30%) | Hepatic blood flow | Morphine, propranolol, lidocaine, verapamil, isoniazid, labetalol, metoprolol |
| Intermediate ER | 0.3-0.7 | Variable | Both flow + enzymes | Aspirin, codeine, nortriptyline |
| Low ER | < 0.3 | High (> 70%) | Enzyme activity, protein binding | Warfarin, diazepam, phenytoin, theophylline, tolbutamide, chlorpropamide |
Key relationship: For high-ER drugs:
- Hepatic clearance is flow-dependent - directly proportional to hepatic blood flow
- Any change in blood flow (heart failure, cirrhosis, surgery) dramatically changes clearance
- Increasing intrinsic clearance (enzyme induction) has little effect on clearance once ER is already near 1.0
For low-ER drugs:
- Hepatic clearance is capacity-limited (restrictive)
- Affected by enzyme inducers/inhibitors, protein binding, age, liver disease
- NOT significantly affected by hepatic blood flow changes
"Drugs with a high extraction ratio (greater than 0.7) undergo extensive first-pass metabolism, which alters their bioavailability after oral administration. Regardless of the route of administration, drugs with high extraction ratios are significantly affected by alteration in hepatic blood flow." - Barash's Clinical Anesthesia
6. Specific Drug Examples
| Drug | Class | Oral Bioavailability | Reason for Low Bioavailability |
|---|---|---|---|
| Nitroglycerin | Antianginal | < 10% | >90% hepatic first-pass; given SL/transdermal/IV |
| Morphine | Opioid | ~20-40% | Extensive glucuronidation in liver |
| Lidocaine | Antiarrhythmic | ~35% | Never given orally; toxic metabolites (MEGX, GX) accumulate |
| Propranolol | Beta-blocker | ~25% | High ER; marked inter-individual variability |
| Verapamil | CCB/antiarrhythmic | ~20-35% | CYP3A4 metabolism; oral dose > IV dose for same effect |
| Isoniazid | Antitubercular | Variable | Acetylation polymorphism (NAT2 gene) |
| Naloxone | Opioid antagonist | < 2% | Near-complete first-pass; IV/IM/intranasal use only |
| Testosterone | Androgen | < 10% | Extensive hepatic first-pass; requires esterification |
| Meperidine | Opioid | Variable | Active metabolite normeperidine accumulates |
"Lidocaine and verapamil are both used to treat cardiac arrhythmias and have bioavailability less than 40%, but lidocaine is never given orally because its metabolites are believed to contribute to central nervous system toxicity." - Katzung's
7. Routes Bypassing First-Pass Metabolism
| Route | Bypass of Hepatic FPM | Mechanism | Examples |
|---|---|---|---|
| Sublingual / Buccal | Complete | Absorbed into systemic veins, not portal | Nitroglycerin SL, buprenorphine |
| Intravenous (IV) | Complete (100% F) | Direct systemic delivery | Morphine IV, lidocaine IV |
| Intramuscular (IM) | Complete | Systemic capillary absorption | Vaccines, depot formulations |
| Subcutaneous (SC) | Complete | Systemic capillary absorption | Insulin, heparin |
| Transdermal | Complete | Absorbed into systemic veins | Nitroglycerin patch, fentanyl patch, scopolamine |
| Inhalation | Bypasses hepatic FPM* | Pulmonary circulation direct to heart | Salbutamol, inhaled steroids |
| Rectal (lower) | ~50% bypass | Inferior rectal veins → IVC; upper rectum drains to portal | Suppositories |
Note on rectal route: "Drugs absorbed from suppositories in the lower rectum enter vessels that drain into the inferior vena cava, thus bypassing the liver. However, suppositories tend to move upward in the rectum into a region where veins that lead to the liver predominate. Thus, only about 50% of a rectal dose can be assumed to bypass the liver." - Katzung's
Note on inhaled corticosteroids: "Although a majority of the inhaled dose is deposited in the oropharynx and swallowed, inhaled corticosteroids are subject to first-pass metabolism in the liver and thus are remarkably free of other short-term complications in adults." - Katzung's
8. Prodrugs: Exploiting First-Pass Metabolism
Some drugs are administered as inactive prodrugs and rely on first-pass (or systemic) metabolism to generate the active compound. This strategy is used to improve oral bioavailability, GI tolerability, or tissue targeting.
| Prodrug | Active Form | Activating Enzyme | Clinical Note |
|---|---|---|---|
| Enalapril | Enalaprilat | Hepatic esterases | Oral ester; enalaprilat itself has <10% oral bioavailability |
| Codeine | Morphine | CYP2D6 (O-demethylation) | Poor metabolizers (10% of Caucasians) lack analgesic effect |
| Clopidogrel | Active thiol metabolite | CYP2C19 | Loss-of-function allele = reduced platelet inhibition ("clopidogrel resistance") |
| Levodopa | Dopamine | DOPA decarboxylase | Given with carbidopa to reduce peripheral conversion |
| Prednisone | Prednisolone | Hepatic 11β-HSD | Avoid in severe liver disease; give prednisolone directly |
| Tamoxifen | Endoxifen | CYP2D6 | Poor CYP2D6 metabolizers may have reduced efficacy |
9. Factors Modifying First-Pass Metabolism
9.1 Genetic Polymorphisms (Pharmacogenomics)
- CYP2D6: Controls metabolism of codeine, metoprolol, tamoxifen, nortriptyline. Phenotypes: poor (PM), intermediate (IM), extensive (EM), ultra-rapid (UM) metabolizers.
- UMs may have dangerously high codeine → morphine conversion (toxicity risk)
- PMs may have exaggerated propranolol/metoprolol effects
- CYP2C19: Affects clopidogrel, omeprazole, voriconazole. Loss-of-function alleles common in East Asians (~15-20%)
- NAT2 acetylation polymorphism: Determines isoniazid first-pass in slow vs. fast acetylators
9.2 Hepatic Disease
- Cirrhosis: Portosystemic shunting + reduced hepatocyte mass = dramatically increased oral bioavailability of high-ER drugs
- "The oral bioavailability for high first-pass drugs such as morphine, meperidine, midazolam, and nifedipine is almost doubled in patients with cirrhosis, compared to those with normal liver function. Therefore, the size of the oral dose of such drugs should be reduced in this setting." - Harrison's, 22nd Ed
- "Drugs with a low extraction ratio (less than 0.3) have restrictive hepatic clearance. Clearance of drugs in this class is affected by protein binding, the induction or inhibition of hepatic enzymes, age, and hepatic pathology, but clearance is not significantly affected by hepatic blood flow." - Barash's
9.3 Heart Failure & Hemodynamic Changes
- Reduced hepatic blood flow → reduced clearance of high-ER drugs
- Decreased gut perfusion → reduced drug absorption and first-pass exposure
- During liver surgery with hepatic inflow clamping: first-pass drugs accumulate significantly
9.4 Chronic Kidney Disease (CKD)
- "Increased absorption in patients with CKD from reduced first-pass metabolism is seen with some β-blockers, dextropropoxyphene, and dihydrocodeine." - Comprehensive Clinical Nephrology
- Uremia can also alkalinize gastric pH (via salivary urea) and alter absorption
- Metallic phosphate binders (Al/Ca/Mg salts) form nonabsorbable complexes, reducing absorption
9.5 Drug Interactions
| Interaction | Effect on First-Pass | Clinical Consequence |
|---|---|---|
| Enzyme inducers (rifampicin, carbamazepine, phenytoin, St. John's Wort) | ↑ First-pass | ↓ Bioavailability → treatment failure |
| Enzyme inhibitors (clarithromycin, itraconazole, HIV protease inhibitors) | ↓ First-pass | ↑ Bioavailability → toxicity |
| Grapefruit juice (inhibits CYP3A4 + P-gp in gut) | ↓ First-pass | ↑ Bioavailability of felodipine, simvastatin, midazolam |
| P-gp inhibitors (quinidine, cyclosporine) | ↓ Efflux from gut | ↑ Absorption of P-gp substrates |
9.6 Age
- Neonates: CYP enzymes incompletely developed at birth; first-pass may be reduced, leading to accumulation
- Elderly: Reduced liver mass and hepatic blood flow → lower first-pass for many drugs → higher bioavailability; doses should start lower
- Sex: CYP3A4 activity is higher in women than men, leading to some sex-based pharmacokinetic differences
9.7 Food Effects
- High-fat meals can increase portal blood flow and alter hepatic extraction
- Food can either increase or decrease first-pass depending on the drug (e.g., food increases propranolol bioavailability by increasing hepatic blood flow)
10. Clinical Implications & Dosing
10.1 Oral-to-IV Dose Conversion
For high-ER drugs, the oral dose must be much larger than the IV dose to achieve the same effect:
Oral dose = IV dose / F
Example - Morphine: F ≈ 0.3 → Oral:IV ratio ≈ 3:1 (30 mg oral ≈ 10 mg IV)
10.2 Toxic Metabolite Accumulation
- Even if therapeutic blood concentrations are reached by large oral doses, metabolite concentrations may be proportionally higher compared to IV administration
- This is why lidocaine is never given orally - high oral doses needed for arrhythmia control would generate toxic levels of glycinexylidide (GX) and monoethylglycinexylidide (MEGX), causing CNS toxicity
- Similarly, meperidine orally accumulates normeperidine (pro-convulsant)
10.3 Inter-individual Variability
- "Drugs with high extraction ratios will show marked variations in bioavailability between subjects because of differences in hepatic function and blood flow." - Katzung's
- This variability complicates dosing of propranolol, verapamil, metoprolol, and other high-ER drugs orally
10.4 Route Selection Strategy
- When reliable drug delivery is required, bypass first-pass: use IV, sublingual, transdermal, or IM/SC
- When prodrug activation is desired, oral route with intact hepatic function is needed (e.g., prednisone, enalapril)
11. Summary Table
| Concept | Key Point |
|---|---|
| Definition | Metabolism of drug before reaching systemic circulation, primarily in gut wall and liver |
| Anatomical route | Oral → GI absorption → portal vein → liver → systemic |
| Main site | Liver (also gut wall; lung for parenteral drugs) |
| Main enzymes | CYP3A4, CYP2D6, CYP2C9, CYP2C19; Phase II: UGT, SULT |
| Bioavailability (F) | F = AUC_oral / AUC_IV; reduced by first-pass |
| Extraction ratio | ER = (C_in - C_out)/C_in; High ER = flow-dependent; Low ER = capacity-limited |
| High-ER drugs | Morphine, propranolol, lidocaine, verapamil, nitroglycerin, naloxone, isoniazid |
| Low-ER drugs | Warfarin, diazepam, phenytoin, theophylline, tolbutamide |
| Bypass routes | IV, SL, transdermal, IM/SC (complete); rectal ~50%; inhalation bypasses hepatic FPM |
| Liver disease | ↑ Bioavailability of high-ER drugs (portosystemic shunts + reduced enzyme activity) → dose reduction needed |
| Prodrugs | Some drugs intentionally require first-pass activation (enalapril, codeine, clopidogrel) |
| Drug interactions | Enzyme inducers ↑ first-pass; inhibitors ↓ first-pass; grapefruit inhibits gut CYP3A4/P-gp |
Sources:
- Lippincott Illustrated Reviews: Pharmacology - Routes of administration & bioavailability
- Katzung's Basic and Clinical Pharmacology, 16th Ed - Extraction ratio & bypass routes
- Goodman & Gilman's The Pharmacological Basis of Therapeutics - Bioavailability equations
- Goldman-Cecil Medicine - First-pass effect clinical definition
- Harrison's Principles of Internal Medicine, 22nd Ed (2025) - Liver disease implications
- Barash's Clinical Anesthesia, 9th Ed - Hepatic drug clearance kinetics
- Comprehensive Clinical Nephrology, 7th Ed - CKD effects on first-pass
Pediatrics complete history taking
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
The library database is exhausted on searches - it doesn't have a dedicated pediatric history-taking textbook chapter. I'll now deliver comprehensive notes from my medical knowledge, which is well-established and standardized for this topic.
Pediatric Complete History Taking
Pediatric history taking differs fundamentally from adult history taking. The clinician must simultaneously obtain information from the caregiver (parent/guardian) and, depending on age, the child themselves. The history must cover several domains unique to children: birth/perinatal history, developmental milestones, immunization status, feeding history, and school performance.
Structure of the Pediatric History
1. Identifying Data
2. Chief Complaint (CC)
3. History of Present Illness (HPI)
4. Birth & Perinatal History
5. Feeding & Nutritional History
6. Developmental History
7. Immunization History
8. Past Medical History (PMH)
9. Surgical History
10. Medications & Allergies
11. Family History (FH)
12. Social History (SH)
13. Review of Systems (ROS)
1. Identifying Data
Collected before the formal history begins:
- Patient's full name
- Age and date of birth (note: in neonates/infants, use days/weeks; in children <2 years, use months)
- Sex / gender
- Weight, height, head circumference (plotted on growth chart)
- Race/ethnicity (relevant for certain genetic conditions: sickle cell, G6PD, Tay-Sachs)
- Informant: Who is providing the history? Parent, guardian, grandparent, foster carer? Reliability of the historian should be noted.
- Referred by: GP, specialist, self-referred?
2. Chief Complaint (CC)
- Recorded in the informant's own words (not medical terminology)
- "What brings your child here today?"
- Note the duration alongside the complaint
- In older children (>6-8 years), ask the child directly as well
Example: "My son has been running a high fever and pulling at his right ear for 3 days."
3. History of Present Illness (HPI)
Use SOCRATES or OLDCARTS framework, adapted for children:
| Mnemonic | Component | Pediatric Adaptation |
|---|---|---|
| S | Site | Where is the pain/symptom? (ask child to point) |
| O | Onset | Sudden vs. gradual; time of day; what was child doing |
| C | Character | Burning, aching, colicky? Use child-friendly language |
| R | Radiation | Does it spread anywhere? |
| A | Associations | Fever, vomiting, rash, diarrhea, cough, feeding changes |
| T | Time course | Constant, intermittent, getting better/worse |
| E | Exacerbating/Relieving | What makes it better or worse? Feeding, position, time |
| S | Severity | Use pain scale (0-10 for >3 years; FLACC/Wong-Baker for younger) |
Additional HPI Questions Specific to Children:
- Sick contacts: playmates, siblings, school/daycare contacts with similar illness
- Recent travel: domestic or international - relevant for infectious/parasitic disease
- Animal/insect exposure: pets, farm animals, tick/mosquito bites
- Recent medications given: paracetamol, ibuprofen, home remedies, traditional medicines
- Change in feeding/appetite: breast/bottle refusal is a critical red flag in infants
- Change in activity level: lethargy, irritability, change in cry (high-pitched = meningism)
- Urinary output: number of wet nappies/diapers per day (key dehydration indicator in infants)
- Bowel habits: frequency, consistency, blood/mucus in stool
4. Birth and Perinatal History
This section is unique to pediatrics and essential for infants and young children. It becomes less relevant but still noteworthy in older children with developmental/neurological problems.
4.1 Antenatal History
- Maternal age at time of pregnancy
- Gravida and Para: G_P_ (number of pregnancies, deliveries)
- Prenatal care: When did antenatal care begin? Regular or irregular?
- Maternal health during pregnancy:
- Infections: TORCH (Toxoplasma, Rubella, CMV, HSV, Syphilis, HIV, Varicella, Zika)
- Gestational diabetes: risk of macrosomia, neonatal hypoglycemia
- Hypertension / pre-eclampsia: risk of IUGR, preterm delivery
- Thyroid disease, epilepsy (teratogenic medications)
- Urinary tract infections
- Medications and substances during pregnancy:
- Folic acid supplementation (neural tube defect prevention)
- Teratogens: alcohol (FAS), valproate, warfarin, isotretinoin, thalidomide
- Illicit drug use: opioids (neonatal abstinence syndrome), cocaine
- Smoking: IUGR, SIDS risk
- Investigations during pregnancy:
- Anomaly scans (20-week scan): structural abnormalities
- First trimester screening (nuchal translucency, PAPP-A, βhCG): Down syndrome risk
- Amniocentesis/CVS if indicated: chromosomal abnormalities
- GBS (Group B Streptococcus) swab status
- Polyhydramnios: suggests GI obstruction (esophageal atresia, duodenal atresia), neuromuscular condition
- Oligohydramnios: renal agenesis, IUGR, post-dates, Potter sequence
4.2 Birth History
- Gestational age at delivery: term (37-42 weeks), preterm (<37 weeks), post-term (>42 weeks)
- Preterm: classify as: extremely preterm (<28 wks), very preterm (28-32 wks), moderate/late preterm (32-37 wks)
- Mode of delivery: Spontaneous vaginal delivery (SVD), instrumental (forceps/ventouse), emergency LSCS, elective LSCS
- Reason for operative delivery: fetal distress, failure to progress, breech presentation, maternal indications
- Presentation: vertex, breech, transverse
- Prolonged/obstructed labor: risk of birth asphyxia
- Maternal analgesia/anaesthesia: epidural, opioids (can cause neonatal respiratory depression)
4.3 Neonatal History
- Birth weight: normal (2.5-4.0 kg), low birth weight (LBW <2.5 kg), very LBW (<1.5 kg), macrosomia (>4 kg)
- APGAR scores: at 1 minute and 5 minutes
- Score 7-10: normal; 4-6: moderate depression; 0-3: severe depression
| APGAR Component | 0 | 1 | 2 |
|---|---|---|---|
| Appearance (color) | Blue/pale all over | Blue extremities, pink body | Pink all over |
| Pulse (heart rate) | Absent | <100 bpm | ≥100 bpm |
| Grimace (reflex irritability) | No response | Grimace | Cry/cough/sneeze |
| Activity (muscle tone) | Limp | Some flexion | Active motion |
| Respiration | Absent | Weak/irregular | Strong cry |
- Resuscitation required: oxygen, bag-mask ventilation, chest compressions, intubation, epinephrine
- Admission to NICU/SCBU: reason, duration
- Jaundice: onset (physiological ≥24h vs. pathological <24h), treatment (phototherapy, exchange transfusion)
- Feeding in first days: breast/bottle; any difficulties; supplementation needed
- Congenital abnormalities identified at birth: cleft palate, cardiac defects, limb abnormalities
- Neonatal screening tests (heel prick/Guthrie): PKU, congenital hypothyroidism, sickle cell disease, CF, MCADD, homocystinuria (varies by country)
- Hearing screening: newborn hearing screen result
- Pulse oximetry screening: for critical congenital heart disease
- Length of hospital stay
5. Feeding and Nutritional History
One of the most critical sections in pediatric history - especially in infants and toddlers.
For Infants (0-12 months):
- Breastfeeding:
- Exclusive breastfeeding? Mixed?
- Frequency and duration of feeds
- Difficulties: poor latch, painful feeds, low supply (maternal), poor weight gain (infant)
- When weaned (if applicable)
- Formula feeding:
- Which formula? (standard, hydrolysed, soy, amino acid-based)
- Volume per feed, frequency
- Correct preparation (dilution errors cause hyponatremia or overfeeding)
- Weaning/complementary feeding: When introduced? What foods?
- Concerns: regurgitation/vomiting, refusal to feed, colic, blood in stool
For Toddlers and Older Children:
- Dietary variety: fruits, vegetables, proteins, dairy, grains
- Portion sizes and meal frequency
- Fussy eating: food jags, texture aversion
- Juice/sugary drink intake: caries, obesity risk
- Vitamin/mineral supplementation: vitamin D, iron, fluoride
- Special diets: vegetarian, vegan, gluten-free, elimination diet
- Food allergies/intolerances: peanut, egg, milk, wheat - onset, reaction type, documented?
- Appetite changes with current illness
Growth Monitoring:
- Weight, length/height, head circumference (and BMI in older children) plotted on age/sex-appropriate growth charts
- Growth velocity (centile crossing is more significant than absolute values)
- Failure to thrive (FTT): weight consistently <2nd centile or crossing centiles downward
6. Developmental History
Assessing development is a cornerstone of pediatric history. Use the four developmental domains:
Developmental Domains
| Domain | Description |
|---|---|
| Gross Motor | Large muscle movements: rolling, sitting, standing, walking, running |
| Fine Motor / Adaptive | Hand-eye coordination, grasping, drawing, self-care |
| Language / Speech | Receptive (understanding) and expressive (speaking) |
| Social / Emotional | Smiling, interaction, play, separation anxiety, peer relationships |
Key Developmental Milestones
| Age | Gross Motor | Fine Motor | Language | Social |
|---|---|---|---|---|
| 6 weeks | Lifts chin prone | Hands fisted | Cooing | Social smile |
| 3 months | Holds head up | Follows object 180° | Cooing, laughing | Recognises parents |
| 6 months | Sits with support, rolls | Palmar grasp, transfers | Babbling, razzes | Stranger anxiety begins |
| 9 months | Stands with support, crawls | Pincer grasp developing | "Mama/dada" non-specific | Waves bye-bye |
| 12 months | Walks with support/cruising | Neat pincer grasp | 1-2 words with meaning | Separation anxiety |
| 18 months | Walks independently, runs | Tower of 3-4 cubes | 10-20 words, jargon | Parallel play |
| 2 years | Runs, kicks ball | Tower of 6 cubes | 2-word phrases, 50+ words | Parallel play, copies adults |
| 3 years | Climbs stairs (alternating), tricycle | Copies circle, uses scissors | 3-word sentences, 300+ words | Cooperative play begins |
| 4 years | Hops on one foot, skips | Copies cross, holds pencil | Full sentences, tells stories | Imaginative play |
| 5 years | Skips, catches ball | Copies triangle, writes name | Fluent speech, counts to 10 | Friends, understands rules |
Developmental Red Flags (Immediate Concern)
| Age | Red Flag |
|---|---|
| Any age | Loss/regression of previously acquired milestones |
| 6 weeks | No social smile |
| 3 months | Not fixing/following with eyes |
| 6 months | No babbling, no reaching |
| 9 months | No sitting with support |
| 12 months | No single words, no pointing |
| 18 months | Fewer than 6 words, no functional play |
| 2 years | No 2-word phrases |
| 3 years | Speech not understandable to strangers |
| Any age | No eye contact, no interest in social interaction (autism screening) |
Additional Developmental Questions:
- School performance: grade appropriate? IEP/special education needs?
- Behavioral concerns: ADHD, oppositional defiant behavior, anxiety
- Autism spectrum screening: MCHAT-R (18-24 months)
- Speech therapy, occupational therapy, physiotherapy: current or previous involvement
- Hearing and vision: formal testing results
- Sleep: hours, sleep problems (night terrors, sleep apnea, bedwetting)
7. Immunization History
Critical in all pediatric consultations, particularly for infectious disease presentations.
Information to Obtain:
- Up to date? Review immunization card/record
- Which vaccines received? (compare against national schedule)
- Any missed doses? Catch-up schedule needed?
- Reactions to previous vaccines: local reactions, fever, anaphylaxis
- Parental concerns or vaccine hesitancy: document and address sensitively
- Special vaccines received: BCG (at-risk countries), Hepatitis B (birth dose), Varicella, Meningococcal ACWY/B, Rotavirus
- Travel vaccines: Typhoid, Hepatitis A, Yellow Fever, Japanese Encephalitis
Standard UK/US Childhood Immunization Schedule (Core):
| Age | Vaccines |
|---|---|
| Birth | Hepatitis B (if not universal, then at-risk infants) |
| 6-8 weeks | DTaP/IPV/Hib/HepB, Rotavirus, PCV13, MenB |
| 3-4 months | DTaP/IPV/Hib/HepB, Rotavirus, MenB |
| 12-13 months | MMR, PCV13, MenB, Hib/MenC |
| 2-6 years | Annual influenza (nasal) |
| 3-4 years | MMR booster, DTaP/IPV booster |
| 11-14 years | HPV (2 doses), Td/IPV booster, MenACWY |
8. Past Medical History (PMH)
- Previous illnesses: hospitalisations, serious infections, febrile convulsions
- Chronic conditions: asthma, eczema, epilepsy, diabetes, CHD, IBD, renal disease
- Neonatal problems: jaundice, hypoglycemia, respiratory distress, NEC
- Recurrent infections: suggest immunodeficiency (recurrent otitis media, pneumonia, abscesses)
- Previous investigations: ECGs, echo, EEGs, imaging, blood tests
- Transfusions: blood products received?
- Accidents and injuries: note frequency (child protection consideration if recurrent)
9. Surgical History
- Operations performed, age at time, hospital
- Complications (anesthetic reactions, wound infections, bleeding)
- Common pediatric surgeries to ask about: circumcision, herniotomy, orchidopexy, pyloromyotomy, tonsillectomy/adenoidectomy, grommets, appendectomy, cardiac surgery
10. Medications and Allergies
Current Medications:
- Name, dose, route, frequency, duration
- OTC/home remedies: paracetamol, ibuprofen, antihistamines, herbal preparations
- Vitamins/supplements: iron, vitamin D, omega-3
- Controlled medications: methylphenidate (ADHD), growth hormone, anticonvulsants
Allergies:
- Drug, food, environmental, insect venom
- Nature of reaction: rash, urticaria, angioedema, anaphylaxis, GI symptoms
- Documented or suspected?
- Has adrenaline auto-injector (EpiPen) been prescribed?
11. Family History (FH)
In pediatrics, family history is particularly important as many conditions are genetic.
- Parental health: age, health status
- Consanguinity: first-cousin marriages (increases risk of autosomal recessive conditions)
- Siblings: ages, health; any similar illness in siblings?
- Genetic conditions in family: CF, sickle cell, thalassemia, muscular dystrophy, PKU
- Cardiac conditions: congenital heart disease, arrhythmias (Long QT syndrome - ask about unexplained sudden death in young family members)
- Metabolic conditions: familial hypercholesterolemia, diabetes
- Neurological: epilepsy, intellectual disability, learning difficulties
- Atopic triad: asthma, eczema, allergic rhinitis (in patient and first-degree relatives)
- Malignancy: especially childhood cancers, hereditary cancer syndromes
- Neonatal deaths / stillbirths: may indicate metabolic or genetic conditions
- Mental health: depression, anxiety, ADHD, autism spectrum
12. Social History (SH)
The social context of a child's life has profound effects on health outcomes.
Family Structure:
- Who does the child live with? (both parents, single parent, grandparents, foster care)
- Parents' relationship status
- Number of siblings, their ages
- Primary caregiver: who looks after the child during the day?
Housing:
- Type of accommodation (house, flat, temporary housing)
- Overcrowding (TB, meningitis, respiratory infection risk)
- Heating, ventilation, damp/mold (asthma, respiratory disease)
- Pets at home (allergies, zoonoses)
- Smoking in the household: passive smoke exposure (asthma, otitis media, SIDS)
Socioeconomic Status:
- Parental occupation(s)
- Financial difficulties / benefits received
- Food security
- Access to healthcare
Childcare / Education:
- Nursery, daycare, school attendance
- School year/grade
- Absenteeism and reason
- Bullying concerns
Child's Activities & Interests:
- Sports and physical activity
- Screen time (TV, tablets, phones) - recommended <1 hr/day under 5
- Hobbies
Child Protection Considerations (SAFEGUARDING):
Always consider child maltreatment. Risk factors include:
- History inconsistent with injury pattern
- Delay in seeking medical attention
- Multiple unexplained injuries
- Concerning bruising (non-mobile infants, unusual sites: ear, neck, buttocks)
- Poor hygiene, neglect signs
- Child appears fearful of parent
- Document factually and report per local safeguarding protocol
For Adolescents - HEADSS Assessment:
| Domain | Questions |
|---|---|
| Home | Who do you live with? How are things at home? |
| Education/Employment | How is school going? Any problems? |
| Activities | What do you do in your free time? |
| Drugs | Do your friends use drugs/alcohol? Do you? |
| Sexuality | Have you started dating? Are you sexually active? (confidentiality) |
| Suicide/Depression | How are you feeling in yourself? Any thoughts of harming yourself? |
13. Review of Systems (ROS)
A systematic enquiry to detect symptoms not volunteered. Adapted for age.
General:
- Fever, night sweats, weight loss/gain
- Fatigue, lethargy, change in activity
- Growth concerns (too tall, too short, too fat, too thin)
Head, Eyes, Ears, Nose, Throat (HEENT):
- Headaches: site, frequency, severity, associated nausea/vomiting/photophobia, aura
- Visual problems: squint (strabismus), decreased vision, photophobia
- Ear: hearing loss, recurrent otitis media, discharge, ear pain, grommets
- Nose: recurrent colds, rhinorrhea, epistaxis (nosebleeds), nasal obstruction
- Throat: recurrent tonsillitis, streptococcal sore throat, mouth ulcers
- Teeth/oral: dental hygiene, caries, thumb sucking
Respiratory:
- Cough: duration, productive/dry, nocturnal, post-exercise (asthma), pertussis-like (whooping)
- Wheeze: first episode vs. recurrent
- Shortness of breath, exercise intolerance
- Cyanosis: peripheral vs. central
- Stridor: inspiratory (upper airway) vs. expiratory (lower airway)
- Apnea episodes (infants)
Cardiovascular:
- Cyanosis, pallor
- Exercise intolerance, poor feeding (infants - equivalent of exercise intolerance)
- Palpitations, syncope
- Known murmur: innocent vs. pathological
- Chest pain (uncommon in children; consider costochondritis, arrhythmia, rarely ischaemic)
- Oedema
Gastrointestinal:
- Abdominal pain: site (periumbilical - functional; RIF - appendicitis), character, frequency
- Nausea, vomiting: bilious (must exclude obstruction), projectile (pyloric stenosis), hematemesis
- Diarrhea: duration, frequency, consistency, blood/mucus, urgency
- Constipation: frequency, stool consistency, soiling/overflow (encopresis), pain
- Jaundice: eyes, skin, dark urine, pale stools
- Rectal bleeding: bright red (anal fissure, intussusception, Meckel's), dark/melena
- Hernia: inguinal (common in boys), umbilical
- Swallowing difficulties: dysphagia, drooling
Genitourinary:
- Urinary frequency, urgency, dysuria (UTI)
- Haematuria: frank or microscopic
- Polyuria/polydipsia (diabetes mellitus/insipidus)
- Enuresis: nocturnal (bedwetting) - age, primary vs. secondary, nocturnal only vs. daytime also
- Genital abnormalities: undescended testes, hypospadias (usually detected at birth)
- In adolescent girls: menstrual history (age of menarche, cycle regularity, dysmenorrhea, LMP)
Musculoskeletal:
- Joint pain, swelling, stiffness (morning stiffness: JIA)
- Limp: painful vs. painless; acute vs. chronic
- Bone pain: nocturnal pain (osteosarcoma)
- Muscle weakness, fatigue, Gowers sign (DMD)
- Back pain (rare in children; investigate if present)
Neurological:
- Seizures: type, duration, frequency, postictal state, triggers, febrile vs. afebrile
- Headaches (see HEENT above)
- Developmental regression (always a red flag)
- Tremor, abnormal movements, tics
- Balance problems, ataxia
- Weakness, paralysis, abnormal gait
- Speech and language concerns (see Developmental History)
- Behavioral changes, mood changes
Skin:
- Rashes: morphology, distribution, onset, itching, association with fever
- Eczema: sites, severity, triggers, treatment used
- Urticaria, angioedema
- Birthmarks, pigmentation changes (café-au-lait spots: neurofibromatosis)
Endocrine:
- Growth concerns: short stature, tall stature, growth velocity changes
- Puberty: precocious (<8 years girls, <9 years boys) or delayed (>13 girls, >14 boys)
- Thyroid symptoms: heat/cold intolerance, weight change, tremor, goiter, exophthalmos
- Polyuria, polydipsia, weight loss (T1DM)
Haematology/Oncology:
- Pallor, fatigue (anemia)
- Bruising, petechiae, bleeding tendency
- Lymphadenopathy: site, duration, tenderness, size (>1 cm generalized is abnormal)
- Splenomegaly, hepatomegaly symptoms
14. Special Considerations by Age Group
| Age Group | Key Extra Considerations |
|---|---|
| Neonate (0-28 days) | Full birth/perinatal history dominant; feeding (breast/bottle); jaundice; umbilical stump; circumcision; maternal GBS status; TORCH |
| Infant (1-12 months) | Feeding, growth, developmental milestones, immunisations, safeguarding (non-accidental injury) |
| Toddler (1-3 years) | Feeding problems, language development, toilet training, tantrums, safety (ingestion, falls) |
| Pre-school (3-6 years) | School readiness, speech, social development, behavioural issues |
| School age (6-12 years) | Academic performance, friendships, bullying, screen time, physical activity |
| Adolescent (12-18 years) | HEADSS assessment, confidentiality, puberty, sexual health, mental health, substance use |
15. Confidentiality in Adolescents
- Adolescents have the right to confidentiality from age 16 in most jurisdictions (Fraser competence/Gillick competence applies to younger adolescents)
- Inform the adolescent what you can keep confidential and what you may need to share (safeguarding disclosures are never confidential)
- Conduct part of the history without the parent in the room for adolescents
- Document who provided the history and any confidentiality arrangements made
Summary Checklist
| Section | Key Elements |
|---|---|
| Identifying data | Name, age, DOB, informant |
| Chief complaint | In informant's own words + duration |
| HPI | SOCRATES + sick contacts, feeding changes, urine output |
| Birth/perinatal | Antenatal, delivery, neonatal period, Apgar, NBS |
| Feeding/nutrition | Breast/formula/diet, weaning, growth |
| Development | Four domains + milestones + red flags |
| Immunizations | Up to date per schedule, reactions |
| PMH | Hospitalizations, chronic illness, recurrent infections |
| Surgical history | Operations, complications |
| Medications/allergies | Current drugs, OTC, vitamins; allergy type/severity |
| Family history | Genetic, atopy, cardiac, sudden death in young |
| Social history | Family structure, housing, school, HEADSS (adolescents), safeguarding |
| Review of systems | All organ systems, age-adapted |
Pediatrics physical examination 80/20
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Excellent - I have rich clinical content from Rosen's Emergency Medicine. Now I have everything needed for a high-yield 80/20 pediatric physical exam guide.
Pediatric Physical Examination - 80/20 Guide
The 80/20 principle here means: master these core concepts and you will handle the vast majority of pediatric clinical encounters competently.
THE GOLDEN RULE: START FROM THE DOOR
In pediatrics, your most valuable assessment happens before you touch the child. The Pediatric Assessment Triangle (PAT) from across the room tells you immediately if the child is sick or well.
1. The Pediatric Assessment Triangle (PAT)
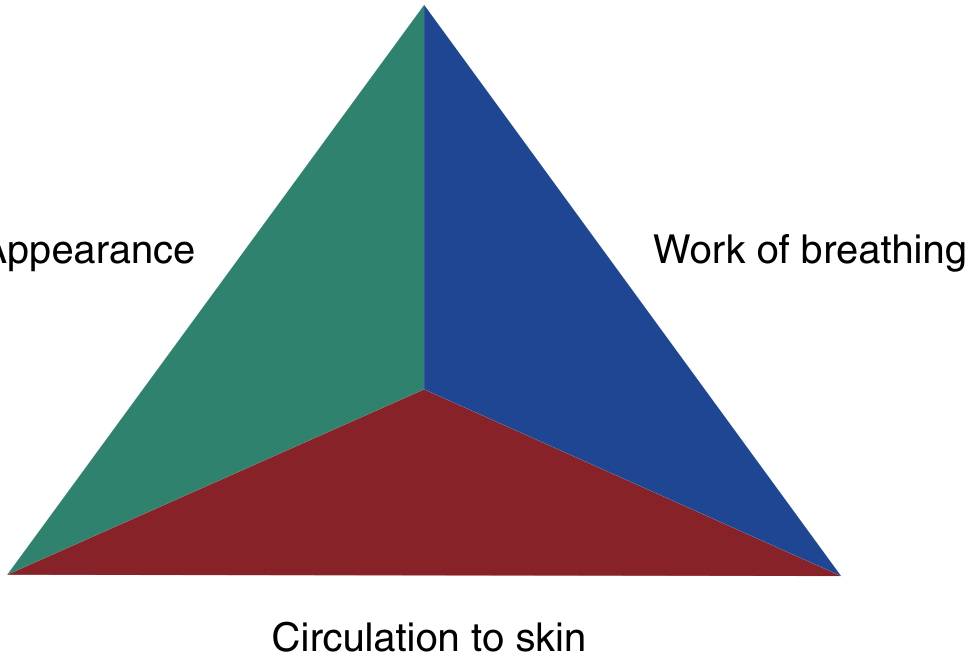
Rosen's Emergency Medicine - assess from the doorway before the child sees you
Three sides assessed visually, without touching:
Side 1: Appearance - TICLS
| Letter | Component | What to observe |
|---|---|---|
| T | Tone | Floppy infant? Moving limbs? Posture? |
| I | Interactivity | Responding to environment? Making eye contact? |
| C | Consolability | Can parent calm the child? Inconsolable = concerning |
| L | Look/Gaze | Alert, tracking? Vacant/glazed? |
| S | Speech/Cry | Normal cry? Weak, high-pitched (meningitis), or no cry? |
Side 2: Work of Breathing
- Abnormal sounds without stethoscope: stridor (upper), wheeze (lower), grunting (lung collapse/fluid)
- Abnormal positioning: sniffing position, tripod (severe - arms forward, leaning), refusal to lie flat
- Retractions: suprasternal, supraclavicular, intercostal, subcostal - more sites = more severe
- Nasal flaring: reducing airway resistance
- Head bobbing, seesaw breathing = impending respiratory failure
Side 3: Circulation to Skin
- Pallor: anemia, shock
- Mottling: poor peripheral perfusion
- Cyanosis: central (mucous membranes) vs. peripheral
- Petechiae: meningococcemia until proven otherwise
PAT Interpretation - Key Clinical States
| PAT Finding | Appearance | Work of Breathing | Circulation | Diagnosis |
|---|---|---|---|---|
| Respiratory distress | Normal | Abnormal | Normal | Airway/lung problem, child compensating |
| Respiratory failure | Abnormal | Abnormal | Normal-abnormal | Exhausted, needs immediate airway support |
| Compensated shock | Normal | Normal | Abnormal | Perfusion failing, brain still protected |
| Decompensated shock | Abnormal | Normal-abnormal | Abnormal | Critical - imminent arrest |
| Brain dysfunction | Abnormal | Normal | Normal | CNS pathology (seizure, meningitis, encephalitis) |
| Cardiopulmonary failure | Abnormal | Abnormal | Abnormal | Pre-arrest - resuscitate immediately |
"On the basis of the initial PAT, the emergency clinician can distinguish the 'sick' from the 'well' child rapidly." - Rosen's Emergency Medicine
2. Vital Signs - Age-Specific Normal Values
The single most commonly tested knowledge in pediatric exams. Values decrease with age.
Heart Rate (beats/min)
| Age | 5th %ile | 50th %ile (Normal) | 95th %ile |
|---|---|---|---|
| 0-3 months | 113 | 140 | 171 |
| 3-6 months | 108 | 135 | 169 |
| 6-9 months | 106 | 134 | 167 |
| 9-12 months | 104 | 132 | 165 |
| 12-18 months | 102 | 128 | 163 |
| 2-3 years | 92 | 117 | 151 |
| 4-6 years | 80 | 103 | 133 |
| 6-8 years | 72 | 94 | 122 |
| 8-12 years | 67 | 87 | 113 |
| 12-15 years | 62 | 82 | 107 |
Source: Rosen's / Roberts and Hedges' Clinical Procedures in Emergency Medicine (Bonafide et al, Pediatrics 2013)
Respiratory Rate (breaths/min)
| Age | 5th %ile | 50th %ile (Normal) | 95th %ile |
|---|---|---|---|
| 0-3 months | 27 | 41 | 62 |
| 3-6 months | 25 | 38 | 58 |
| 6-12 months | 22 | 33 | 51 |
| 1-2 years | 20 | 29 | 45 |
| 2-3 years | 18 | 27 | 42 |
| 3-6 years | 17 | 24 | 37 |
| 6-8 years | 16 | 23 | 35 |
| 8-12 years | 15 | 21 | 31 |
| 12-18 years | 13 | 18 | 26 |
80/20 memory rule: Newborn ~40, halves to ~20 by age 2, approaches adult (~15) by school age.
"Normal pediatric respiratory rates are inversely related to age due to younger children's increased metabolic rates and lower tidal volume reserves." - Rosen's
Blood Pressure (mmHg) - Simplified
| Age | Systolic (approx.) | Diastolic (approx.) |
|---|---|---|
| Neonate | 65-85 | 45-55 |
| 1-12 months | 70-100 | 50-65 |
| 1-3 years | 80-110 | 55-70 |
| 3-6 years | 85-110 | 55-70 |
| 6-12 years | 90-120 | 60-75 |
| Adolescent | 100-130 | 65-80 |
Quick formula for minimum acceptable systolic BP in children >1 year:
Minimum systolic BP = 70 + (2 × age in years) mmHg (Below this = hypotension requiring immediate action)
Temperature
- Normal: 36.5-37.5°C (axillary); 37-38°C (rectal, 0.5°C higher)
- Fever: ≥38.0°C rectal / ≥37.5°C axillary
- Fever in neonate <28 days: ≥38.0°C = sepsis workup (LP, blood culture, IV antibiotics) regardless of appearance
- Hyperpyrexia: >40.5°C - consider CNS pathology, heat stroke
Oxygen Saturation
- Normal SpO₂: ≥95% in room air (≥96% ideal)
- 90-94%: concerning, supplemental O₂ needed
- <90%: hypoxia, urgent intervention
3. General Appearance
After PAT, formally assess:
- Well or unwell? Trust your gut - experienced clinicians identify sick children rapidly
- Nutritional status: wasted, normal, obese
- Growth: plot weight, height/length, head circumference on growth chart
- Alertness: GCS (adapted for pediatrics) or AVPU scale
- Hydration (see Section 9)
- Dysmorphic features: Down syndrome (upslanted palpebral fissures, flat nasal bridge, single palmar crease), Turner, Marfan
- Hygiene and dress: signs of neglect
AVPU Scale (rapid consciousness assessment)
| Level | Description |
|---|---|
| A | Alert |
| V | Responds to Voice |
| P | Responds to Pain |
| U | Unresponsive |
P or U in a child = emergency
4. Head and Fontanelles
The anterior fontanelle is the single most important structure in infant examination.
| Fontanelle | Closes | Normal size |
|---|---|---|
| Anterior (diamond-shaped) | 12-18 months | Up to 2.5 cm diameter |
| Posterior (triangular) | 6-8 weeks | Fingertip-sized |
Anterior fontanelle assessment - must do with infant upright and calm:
| Finding | Interpretation |
|---|---|
| Bulging (tense, non-pulsatile) | ↑ intracranial pressure: meningitis, hydrocephalus, subdural, vitamin A toxicity |
| Sunken | Dehydration |
| Normal (slightly pulsatile, flat) | Normal |
| Delayed closure (>18 months) | Hypothyroidism, hydrocephalus, rickets, Down syndrome |
| Early closure (<3 months) | Craniosynostosis |
Head shape:
- Plagiocephaly: asymmetric flattening (positional - common)
- Microcephaly (<2 SD): TORCH infections, genetic, fetal alcohol syndrome
- Macrocephaly (>2 SD): hydrocephalus, storage diseases, benign familial
Head circumference normal values:
- Newborn: ~34 cm
- 3 months: ~41 cm
- 6 months: ~44 cm
- 12 months: ~47 cm
- 2 years: ~49 cm
- Grows ~2 cm/month in first 3 months, then ~1 cm/month to 6 months, then ~0.5 cm/month to 12 months
5. Eyes
- Conjunctivae: pallor (anemia), jaundice
- Pupils: equal, round, reactive to light (PEARL); unequal = herniation/CN3 palsy
- Red reflex: must be checked in all infants and children - absent red reflex = retinoblastoma, cataract, glaucoma (urgent ophthalmology referral)
- Squint (strabismus): corneal light reflex test (Hirschberg) + cover test
- Constant squint at any age: abnormal
- Pseudostrabismus (epicanthic folds): normal variant in infants
- Nystagmus: cerebellar, vestibular, or congenital
- Periorbital edema: nephrotic syndrome (bilateral, non-pitting, worse in morning), orbital/periorbital cellulitis
6. Ears, Nose, Throat
Ears
- Otoscopy: examine last (will upset the child - save upsetting examinations for the end)
- Normal TM: pearly grey, cone of light (anteroinferiorly), visible handle of malleus
- Otitis media: red, bulging, opaque TM, ± perforation with discharge
- Otitis media with effusion ("glue ear"): dull, grey-yellow TM, absent light reflex, air-fluid level
- Preauricular pits/tags: associated with renal anomalies (consider renal USS)
- Low-set ears: Down syndrome, Turner syndrome, renal agenesis
Nose
- Nasal flaring: respiratory distress
- Discharge: clear (viral/allergy), purulent (bacterial sinusitis, foreign body)
- Nasal polyps in child: think cystic fibrosis
Throat / Mouth
- Examine last in the cooperative child, or save for end in infants
- Tonsils: grade 0-4 (grade 4 = "kissing tonsils" meeting midline)
- Grading: 1 = within pillars; 2 = touching pillars; 3 = beyond pillars; 4 = touching midline
- Exudate: bacterial tonsillitis (strep), EBV (mononucleosis - look for petechiae at junction of hard/soft palate)
- Peritonsillar abscess: unilateral tonsillar swelling, uvular deviation, "hot potato" voice, trismus
- Koplik spots: pathognomonic of measles (white spots on buccal mucosa opposite molars)
- Dental caries: neglect marker, prolonged bottle feeding
- Cleft palate: can be subtle (submucous) - run finger along hard palate
- Thrush (white plaques on mucosa): Candida - remove with spatula (unlike milk)
- Strawberry tongue: scarlet fever, Kawasaki disease
7. Neck and Lymph Nodes
Lymphadenopathy assessment:
- Normal: cervical nodes up to 1 cm, inguinal up to 1.5 cm in children
- Significant: >1 cm generalized; >2 cm localized; firm/hard/fixed/non-tender
- Tender, mobile, soft = reactive (viral infection)
- Hard, fixed, painless = malignancy (lymphoma)
- Fluctuant = abscess
Neck stiffness:
- In infants: a bulging fontanelle is more reliable than neck stiffness (meningism may be absent <18 months)
- Kernig's sign: with hip flexed 90°, unable to extend knee >135° due to pain
- Brudzinski's sign: passive neck flexion causes involuntary hip/knee flexion
- Both signs have poor sensitivity in young children - clinical judgment + LP if concerned
Other neck findings:
- Thyroid: goiter - hypothyroidism, hyperthyroidism, Hashimoto's
- Torticollis: lateral neck tilt - muscular (SCM fibrosis), Sandifer syndrome (GERD), atlantoaxial subluxation (Down syndrome - check before manipulation)
- Webbed neck: Turner syndrome
- Cystic hygroma/branchial cyst: soft, transilluminable neck mass
8. Respiratory System
Observe before auscultating:
- Respiratory rate: count for full 60 seconds in infants (irregular)
- Accessory muscle use: sternomastoid, scalene
- Chest shape: barrel chest (chronic air trapping - asthma), pectus excavatum/carinatum
- Symmetry of movement: reduced on side of pneumonia, effusion, or pneumothorax
Auscultation - most important findings:
| Sound | Interpretation |
|---|---|
| Wheeze (expiratory, musical) | Bronchospasm: asthma, bronchiolitis, foreign body |
| Crackles (crepitations, fine) | Alveolar: pneumonia, pulmonary edema |
| Coarse crackles | Secretions in large airways: bronchitis, CF |
| Stridor (inspiratory, harsh) | Upper airway obstruction: croup, epiglottitis, foreign body |
| Reduced/absent breath sounds | Consolidation, pleural effusion, pneumothorax |
| Bronchial breathing | Consolidation (air bronchograms on CXR) |
Percussion:
- Dull: consolidation, effusion
- Hyperresonant: pneumothorax, air trapping
80/20 key distinguishing findings:
| Condition | Key Sign |
|---|---|
| Bronchiolitis | Wheeze + crackles in infant <2 years, after URTI |
| Asthma | Wheeze ± hyperinflation, worse at night/with exercise, good response to salbutamol |
| Croup | Barking cough + inspiratory stridor, low-grade fever, hoarse voice |
| Epiglottitis | High fever + stridor + drooling + "hot potato" voice + toxic appearance (do NOT examine throat) |
| Pneumonia | Fever + tachypnea + reduced air entry + dullness to percussion + crackles |
| Foreign body | Unilateral wheeze + reduced air entry unilaterally + sudden onset in toddler |
9. Cardiovascular System
Inspection:
- Cyanosis (central = oral mucosa/tongue), clubbing (chronic hypoxia: cyanotic CHD, CF)
- Precordial bulge (cardiomegaly)
- Scars (previous cardiac surgery)
- Respiratory distress + poor feeding in infant = heart failure equivalent
Palpation:
- Apex beat: normally 4th intercostal space, midclavicular line in children <7 years; 5th ICS, MCL in older children
- Displaced laterally = cardiomegaly
- Heaves and thrills: thrill = palpable murmur (grade ≥4)
Auscultation - heart sounds:
- S1 (mitral/tricuspid closure) + S2 (aortic/pulmonary closure): normal
- S3 gallop: volume overload, heart failure (normal in thin children)
- Fixed split S2: ASD (pathognomonic)
- Loud P2: pulmonary hypertension
Murmurs - the critical differentiation:
Innocent vs. Pathological Murmur
| Feature | Innocent | Pathological |
|---|---|---|
| Timing | Systolic only | Systolic, diastolic, or continuous |
| Quality | Soft, musical, vibratory | Harsh, blowing |
| Grade | 1-2/6 | Often ≥3/6 |
| Location | Variable | Fixed to specific valve area |
| Radiation | No | Often radiates (e.g., to carotids/axilla) |
| Changes with position | Decreases lying, increases sitting/standing | May not change |
| Symptoms | None | Failure to thrive, cyanosis, exercise intolerance |
| S2 | Normal | May be abnormal |
The 6 "S's" of innocent murmurs: Soft, Short, Systolic, Sensitive to position, no Symptoms, no thrill
Common innocent murmurs:
- Still's murmur: vibratory, musical, grade 2-3/6, lower left sternal edge, most common (2-7 years)
- Pulmonary flow murmur: ejection systolic, left upper sternal edge, normal in neonates
- Venous hum: continuous, infraclavicular, disappears when jugular vein compressed or child lies flat
Pathological murmur patterns:
| Condition | Murmur Character |
|---|---|
| VSD | Pansystolic, harsh, lower left sternal border |
| ASD | Ejection systolic + fixed split S2, upper left sternal border |
| PDA | Continuous "machinery" murmur, left infraclavicular |
| Pulmonary stenosis | Ejection systolic + ejection click, upper left sternal border, radiates to back |
| Aortic stenosis | Ejection systolic, upper right sternal border, radiates to carotids |
| Coarctation | Systolic murmur, left infrascapular; radio-femoral delay; upper > lower limb BP |
Peripheral pulses:
- Always palpate femoral pulses in neonates/infants - absent/weak femoral + upper limb hypertension = coarctation of aorta
- Radio-femoral delay: >0.2 second delay = coarctation
Capillary refill time (CRT): Press sternum for 5 seconds, release
- Normal: <2 seconds
-
2 seconds = poor perfusion / dehydration / shock
10. Dehydration Assessment
The most clinically tested pediatric examination skill.
| Sign | Mild (3-5%) | Moderate (5-10%) | Severe (>10%) |
|---|---|---|---|
| Mucous membranes | Dry ± | Dry + | Very dry + |
| Anterior fontanelle | Normal | Sunken + | Sunken + |
| Skin turgor (pinch abdomen) | Normal | Reduced ± | Tenting + |
| Sunken eyes | - | + | + |
| Mental status | Alert | Irritable | Lethargic |
| Heart rate | Normal | Tachycardia | Tachycardia |
| Capillary refill | <2 sec | >2 sec | >2 sec |
| Hypotension | - | Orthostatic ± | Present |
| Urine output | Normal | Reduced | Oliguria/anuria |
Source: Rosen's Emergency Medicine, adapted from Barkin & Rosen, Emergency Pediatrics
"The three most useful signs to determine dehydration of more than 5% are prolonged capillary refill time, abnormal skin turgor, and abnormal respiratory pattern." - Rosen's Emergency Medicine
Skin turgor test: Pinch skin on abdomen (not dorsum of hand in infants) - normal returns immediately, tenting (>2 second) = >10% dehydration
Special skin signs in dehydration:
- Skin tenting (slow recoil): suggests hyponatremic dehydration
- Doughy texture: hypernatremic dehydration (water shifts from cells to interstitium)
11. Abdomen
Order: Inspect → Auscultate → Percuss → Palpate (palpate last - pressing on a tender area upsets child)
Inspection:
- Distension: obstruction, ascites, organomegaly, constipation
- Scars
- Visible peristalsis: pyloric stenosis (wave from left hypochondrium to right - olive mass palpable)
- Umbilical hernia (common, usually resolves by age 2-4 years)
- Inguinal region: hernias, undescended testes
Auscultation:
- Bowel sounds: absent = ileus/peritonitis; hyperactive = obstruction
- Count before palpating
Palpation - technique in children:
- Kneel to child's level; warm hands; distract the child ("take a deep breath", look at the ceiling)
- Use child's own hand over yours if very anxious
- Start in the area AWAY from the reported pain
- Tenderness: localize to quadrant
- Guarding: voluntary (anxiety) vs. involuntary (peritoneal irritation)
- Rebound tenderness: Rovsing's sign (right iliac fossa pain on pressing left iliac fossa) = appendicitis
Organomegaly:
- Liver: normally palpable 1-2 cm below right costal margin in infants and young children (normal finding)
- Hepatomegaly if >3.5 cm below RCM in neonates, >2 cm in children
- Causes: hepatitis, storage disease, right heart failure, leukaemia
- Spleen: usually not palpable; if palpable in a child = significant
- Causes: infections (EBV, malaria), haemolytic anaemia, portal hypertension, leukaemia/lymphoma
- Kidneys: ballottable in neonates/infants; enlarged = hydronephrosis, Wilms' tumour
Key abdominal conditions:
| Condition | Age | Key Exam Finding |
|---|---|---|
| Intussusception | 3 months-3 years | Sausage-shaped mass in RUQ/central abdomen; "redcurrant jelly" stool; intermittent colicky pain |
| Pyloric stenosis | 2-8 weeks | Olive-shaped mass in epigastrium/right of midline; visible peristalsis; projectile non-bilious vomiting |
| Appendicitis | >2 years | Tenderness + guarding at McBurney's point (RIF); Rovsing's sign; fever |
| Hirschsprung | Neonate-infant | Delayed passage of meconium; abdominal distension; empty rectum on PR exam |
| Wilms' tumour | 1-5 years | Smooth, firm unilateral flank/abdominal mass; does NOT cross midline |
12. Genitalia
- Boys: check testes are descended bilaterally (undescended testes need orchidopexy <1 year)
- Hydrocele: fluctuant scrotal swelling, transilluminates - common in infants, usually resolves
- Inguinal hernia: does not transilluminate; may be reducible; urgent if incarcerated
- Testicular torsion: sudden onset severe unilateral scrotal pain, absent cremasteric reflex, high-riding testis = SURGICAL EMERGENCY
- Phimosis: non-retractile foreskin - normal until age 3-4 years; becomes pathological if causing obstruction
- Girls: labial adhesions (common, usually resolve spontaneously); vaginal discharge in prepubertal girls - exclude abuse
- Both sexes: Tanner staging (puberty assessment) - stages 1-5 for breast, pubic hair, genitalia
Tanner Stages (simplified)
| Stage | Breast (girls) | Pubic hair | Genitalia (boys) |
|---|---|---|---|
| 1 | Prepubertal | None | Prepubertal |
| 2 | Breast bud | Fine hair at base | Testicular enlargement (begin puberty) |
| 3 | Enlargement | Darker, spreads | Penile elongation |
| 4 | Areola secondary mound | Adult type, not spread to thighs | Adult size, no spread to thighs |
| 5 | Adult | Adult including medial thighs | Adult |
Normal onset of puberty:
- Girls: breast development 8-13 years (mean 10)
- Boys: testicular enlargement 9-14 years (mean 11.5)
13. Neurological System
Conscious level: AVPU or GCS (modified pediatric GCS for infants)
Tone: hypotonia (floppy infant) vs. hypertonia/spasticity
Primitive reflexes (present in neonates, should disappear by stated age):
| Reflex | Elicited by | Normal disappearance |
|---|---|---|
| Moro (startle) | Sudden head drop | 4-6 months |
| Rooting | Touch corner of mouth | 3-4 months (awake) |
| Sucking | Object in mouth | 4 months (voluntary by then) |
| Palmar grasp | Object in palm | 3-4 months |
| Plantar grasp | Touch sole | 8-12 months |
| Asymmetric Tonic Neck (ATNR/"fencing") | Head turn to one side | 4-6 months |
| Babinski (plantar extensor) | Stroke lateral sole | Normal up to 2 years |
Persistent primitive reflexes beyond expected age = central neurological damage (cerebral palsy)
Cerebellar assessment in children:
- Finger-nose test, heel-shin (adapt: "touch my finger, now touch your nose")
- Gait: wide-based, ataxic = cerebellar; scissor gait = spastic diplegia (CP)
Cranial nerves - rapid pediatric assessment:
- CN II: red reflex, pupil responses, visual tracking
- CN III/IV/VI: eye movements, squint
- CN VII: facial symmetry (smile, raise eyebrows)
- CN VIII: hearing (distraction test <6 months; audiometry in older)
- CN XII: tongue movement (fasciculations = lower motor neuron)
14. Skin
The skin is often the fastest route to diagnosis in children.
| Rash | Key Features | Diagnosis |
|---|---|---|
| Maculopapular + fever | Starts head, spreads down, Koplik spots | Measles |
| Vesicular + fever | Crops of lesions, different stages simultaneously, very itchy | Varicella |
| Petechiae / purpura | Non-blanching, fever, toxic | Meningococcaemia (emergency) |
| Blanching maculopapular | Fever, strawberry tongue, "sandpaper" texture | Scarlet fever |
| Target lesion | Concentric rings (bull's eye) | Erythema multiforme / Lyme disease |
| Salmon-pink evanescent | Fever, comes and goes | Systemic JIA (Still's disease) |
| Butterfly rash | Malar rash, photosensitive | SLE |
| Flexural eczema | Antecubital/popliteal fossa, cheeks in infants | Atopic dermatitis |
| Café-au-lait spots | >6 spots >0.5 cm | Neurofibromatosis type 1 |
| Ash-leaf macules | Hypopigmented, Wood's lamp | Tuberous sclerosis |
Blanching test: press glass firmly on rash - if disappears = blanching (inflammatory/allergic). If persists = non-blanching = petechiae/purpura = possible meningococcaemia until proven otherwise.
15. Musculoskeletal - The Limping Child
One of the highest-yield pediatric exam topics.
| Age | Condition | Key Features |
|---|---|---|
| Neonate | Developmental dysplasia of hip (DDH) | Barlow + Ortolani tests (mandatory in all neonates) |
| <2 years | Septic arthritis | Fever, hot swollen joint, refusal to move, elevated CRP/WCC |
| 2-10 years | Transient synovitis ("irritable hip") | Afebrile, mild pain, internal rotation restricted - diagnosis of exclusion |
| 4-8 years | Perthes' disease (avascular necrosis) | Painless limp, insidious onset, Trendelenburg gait |
| 10-15 years | Slipped capital femoral epiphysis (SCFE) | Obese adolescent, hip pain referred to knee, external rotation, leg shortened |
| Any age | Osteomyelitis | Point tenderness over bone, fever, raised inflammatory markers |
| Any age | Juvenile idiopathic arthritis | Morning stiffness, swollen joints, iridocyclitis (eye screening mandatory) |
Barlow test (infant): hip adducted + posteriorly directed force - hip dislocates posteriorly = positive (unstable)
Ortolani test (infant): hip abducted + anterior pressure on greater trochanter - clunk = hip reducing = positive (dislocated)
Trendelenburg test: stand on one leg - if opposite pelvis drops = weak hip abductors (gluteus medius) ipsilateral to standing leg = Perthes, DDH, any hip pathology
16. The Practical Approach: Age-Adapted Examination Sequence
| Age | Strategy |
|---|---|
| Neonate | Examine fully undressed; warm room; all reflexes + red reflex + femoral pulses + hip exam mandatory |
| Infant (1-12m) | Start on parent's lap; distract with toy; examine chest/abdomen first; save throat/ears for last |
| Toddler (1-3y) | Most challenging; stay at eye level; allow to hold a toy; examine on parent's lap; approach slowly |
| Preschool (3-5y) | Engage with play; explain in simple terms; demonstrate on teddy bear |
| School age (6-12y) | Treat as adult with clear explanations; privacy important |
| Adolescent | Offer chaperone; examine appropriate privacy; separate from parent for sensitive issues |
80/20 High-Yield Summary
| What | Why it matters |
|---|---|
| PAT from the door | Sick vs. well determination in seconds |
| Age-appropriate vital signs | Tachycardia/tachypnoea are the earliest signs of illness in children |
| Fontanelle assessment | Bulging = ↑ICP; Sunken = dehydration |
| Red reflex | Retinoblastoma/cataract - must check in every infant |
| Femoral pulses in neonates | Coarctation of aorta - treatable but missed if not checked |
| Non-blanching rash | Meningococcaemia - 15-minute window for IV antibiotics |
| Capillary refill >2 sec | Best single sign of clinically significant dehydration |
| Fixed split S2 | ASD - can be missed for years |
| Moro/primitive reflexes | Persisting beyond expected age = CP or brain injury |
| Barlow/Ortolani | DDH - treat before walking; missed = lifelong hip problems |
Sources: Rosen's Emergency Medicine (Pediatric Assessment Triangle, PAT interpretation, dehydration signs); Roberts and Hedges' Clinical Procedures in Emergency Medicine (vital sign tables - Bonafide et al, Pediatrics 2013); Barash's Clinical Anesthesia (hepatic pharmacokinetics); clinical standard references.
Head to toe example scenario example examine then give the findings..made easy
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I have rich clinical content. Now I'll build the full immersive scenario-based guide.
Pediatric Head-to-Toe Physical Examination
3 Scenarios: Examine → Find → Interpret
The format for each section: What you DO → What you FIND → What it MEANS
🧒 SCENARIO 1: "Ahmed, 8 months old, fever and not feeding well"
Mum brings Ahmed to the clinic. He was well 2 days ago. Now has fever, crying more than usual, and refused his last two bottle feeds.
STEP 1 — FROM THE DOORWAY (PAT)
What you DO: Before entering, stand at the door and observe for 10 seconds. Don't touch. Don't speak. Just look.
| What you observe | What you find |
|---|---|
| Appearance (TICLS) | Ahmed is lying in mum's arms. He's awake. He looks at you briefly but doesn't track. Mum jiggles him but he doesn't smile or reach out. Cry is weak when he fusses. |
| Work of breathing | Shirt is on - ask mum to lift it. You see mild subcostal recession. Nostrils flare slightly with each breath. No stridor. |
| Circulation to skin | Skin looks pale. No rash visible yet. |
What it MEANS: PAT is ABNORMAL on all three sides.
- Abnormal appearance + abnormal breathing + abnormal circulation = Cardiopulmonary compromise or severe illness. This baby is SICK. Move quickly.
STEP 2 — GENERAL IMPRESSION & VITAL SIGNS
What you DO: Lay Ahmed on the examination couch. Count respiratory rate for 60 seconds (watch chest/abdomen without touching). Then measure HR, temperature, SpO₂, weight.
| Vital sign | Finding | Normal for 8 months | Interpretation |
|---|---|---|---|
| Respiratory rate | 58 breaths/min | 22-54 (5th-95th %ile) | Tachypnoeic - at upper limit of normal; with recession = significant |
| Heart rate | 168 bpm | 106-167 (5th-95th %ile) | Tachycardic |
| Temperature | 38.9°C rectal | 36.5-38.0°C | Fever |
| SpO₂ | 91% in room air | ≥95% | Hypoxic - apply O₂ now |
| Weight | 7.2 kg | Expected ~8.5 kg for age | Below expected - check growth chart |
| CRT (sternum) | 3 seconds | <2 seconds | Prolonged - poor perfusion |
STEP 3 — HEAD
What you DO: With Ahmed lying flat, place two fingers gently over the anterior fontanelle. Ask mum to hold him upright and calm for 30 seconds, then reassess the fontanelle.
| What you find | What it MEANS |
|---|---|
| Anterior fontanelle: bulging, tense, non-pulsatile when upright and calm | ↑ Intracranial pressure - meningitis, encephalitis, subdural haematoma. Red flag - do not delay. |
| Head circumference: 44 cm | Normal for 8 months |
| Posterior fontanelle: closed | Normal (closes by 6-8 weeks) |
⚠️ Key rule: Assess fontanelle with baby UPRIGHT and CALM. Crying raises ICP and causes false-positive bulging. A bulging fontanelle when calm and upright = pathological until proven otherwise.
STEP 4 — EYES
What you DO: Shine torch at each eye from 30 cm. Check pupils. Shine through ophthalmoscope for red reflex. Observe eye movement.
| What you find | What it MEANS |
|---|---|
| Pupils equal, 3mm, reacting briskly to light | Normal - no herniation |
| Red reflex present bilaterally (orange glow) | Normal - no cataract/retinoblastoma |
| Eyes appear mildly sunken | Dehydration |
| Mucous membranes: dry | Confirms dehydration |
STEP 5 — EARS, NOSE, THROAT
What you DO: This will upset Ahmed - save for near the end. Wrap him in mum's arms ("headlock" position). Use otoscope on each ear. Depress tongue gently to see posterior pharynx - 5 seconds max.
| What you find | What it MEANS |
|---|---|
| Right tympanic membrane: red, bulging, opaque, no light reflex | Acute otitis media (AOM) right ear - common precipitant of fever and irritability |
| Left TM: pearly grey, cone of light visible | Normal |
| Posterior pharynx: mild erythema, no exudate | Non-specific inflammation |
| Mouth: mucous membranes very dry, no thrush | Confirms dehydration |
STEP 6 — NECK
What you DO: With Ahmed lying flat, place your hand under his head and gently flex the neck forward. Watch his face and hips/legs. Then test Kernig's: flex hip 90° and try to extend the knee.
| What you find | What it MEANS |
|---|---|
| Neck: stiff - resistance and crying on flexion | Meningism - possible meningitis |
| Brudzinski's sign: positive - hips and knees flex when neck is flexed | Meningism confirmed |
| Kernig's sign: positive - unable to extend knee beyond 100° | Meningism |
| Cervical lymphadenopathy: 2-3 small tender nodes bilaterally (~0.5 cm) | Reactive - consistent with infection |
⚠️ Key rule in infants: Meningeal signs can be absent in infants <18 months even with proven meningitis. A bulging fontanelle + fever + irritability in an infant = treat as meningitis even without neck stiffness.
STEP 7 — SKIN (do this early if not done at door)
What you DO: Fully undress Ahmed. Examine all skin systematically in good light. Use a glass (or press firmly with finger) to test any spots.
| What you find | What it MEANS |
|---|---|
| Scattered petechiae on trunk and lower limbs - do not blanch under glass | Non-blanching rash = meningococcaemia until proven otherwise. EMERGENCY. |
| Two petechiae above the nipple line | Above nipple line in a well child after vomiting = may be benign Valsalva. In this case - child is unwell, so still urgent |
| Skin pale, mottled on lower limbs | Poor peripheral perfusion - compensated shock |
🚨 STOP THE EXAM. This child has:
- Fever + non-blanching rash + meningeal signs + bulging fontanelle + tachycardia + prolonged CRT
- Give IV/IM benzylpenicillin NOW. Do not wait for LP. Call senior. Transfer.
STEP 8 — CHEST / RESPIRATORY
What you DO: Expose chest. Observe, then auscultate all zones (2 anterior, 2 lateral, 4 posterior).
| What you find | What it MEANS |
|---|---|
| Subcostal + mild intercostal recession | Increased work of breathing |
| Respiratory rate 58/min | Tachypnoea - compensating for metabolic acidosis (sepsis) |
| Auscultation: clear air entry bilaterally, no wheeze, no crackles | Lungs are clear - respiratory distress is FROM SEPSIS, not primary lung pathology |
| Percussion: resonant bilaterally | No consolidation, no effusion |
Teaching point: Tachypnoea without primary lung findings = suspect metabolic acidosis / sepsis / shock. Not everything tachypnoeic has a respiratory cause.
STEP 9 — CARDIOVASCULAR
What you DO: Palpate apex beat. Auscultate all 4 areas (aortic, pulmonary, tricuspid, mitral). Feel femoral pulses (always in infants).
| What you find | What it MEANS |
|---|---|
| Apex beat: 4th ICS, MCL | Normal for age |
| Heart sounds: S1 + S2, no murmur | No structural heart disease contributing |
| Femoral pulses: present but weak bilaterally | Reduced cardiac output from septic shock |
| Peripheral pulses (brachial): fast, weak, thready | Shock - poor perfusion |
| CRT (sternum): 3 sec | Shock confirmed |
STEP 10 — ABDOMEN
What you DO: Warm your hands. Ahmed is now lying on the couch. Kneel to his level. Auscultate first (5 seconds), then gently palpate all 9 zones starting away from areas of tenderness.
| What you find | What it MEANS |
|---|---|
| Bowel sounds: present, active | Normal |
| Abdomen: soft, not distended | No obstruction, no peritonitis |
| No organomegaly palpable | No hepatosplenomegaly at this stage |
| No palpable masses |
STEP 11 — NEUROLOGY (rapid, targeted)
What you DO: Observe tone and movement. AVPU assessment. Check if primitive reflexes persist normally for age.
| What you find | What it MEANS |
|---|---|
| AVPU: V (responds to voice only, sluggishly) | Altered consciousness - serious CNS involvement |
| Tone: normal | No focal neurological deficit yet |
| Moro reflex: exaggerated | Non-specific irritability/hyperexcitability (meningeal irritation) |
| No focal weakness, moves all limbs | No focal CNS lesion yet |
🔍 PUTTING IT ALL TOGETHER — Ahmed's Findings Summary
| System | Finding | Flag |
|---|---|---|
| General | Unwell, pale, mottled, poor response | 🔴 Sick |
| Vitals | HR 168, RR 58, Temp 38.9, SpO₂ 91%, CRT 3s | 🔴 Septic shock |
| Head | Bulging AF when upright and calm | 🔴 ↑ICP |
| Eyes | Sunken, dry mucosae | 🟡 Dehydration |
| Ears | AOM right ear | 🟡 Source of infection |
| Neck | Neck stiffness, Kernig's +, Brudzinski's + | 🔴 Meningism |
| Skin | Non-blanching petechiae trunk/legs, mottling | 🔴 Meningococcaemia |
| Chest | Tachypnoea, recession, clear lung fields | 🟡 Sepsis-driven |
| CVS | Tachycardia, weak pulses, no murmur | 🔴 Septic shock |
| Abdomen | Soft, normal | 🟢 |
| Neuro | AVPU = V, hyperexcitable | 🔴 CNS involvement |
Diagnosis: Bacterial Meningitis / Meningococcal Septicaemia
Immediate Management:
- IV/IM benzylpenicillin (or ceftriaxone) NOW - do not delay for LP
- High-flow O₂ (target SpO₂ ≥94%)
- IV access + blood culture, FBC, CRP, U&E, glucose, clotting, blood gas
- 20 mL/kg 0.9% NaCl fluid bolus for shock
- Urgent paediatric intensive care transfer
👧 SCENARIO 2: "Layla, 3 years old, barking cough and noisy breathing"
Mum brings Layla at 2am. She had a mild cold for 2 days. Tonight she suddenly woke up with a harsh, barking cough and noisy breathing. She's scared but recognises mum.
FROM THE DOOR — PAT
| Component | Finding | Meaning |
|---|---|---|
| Appearance | Layla is scared, clinging to mum, crying. She tracks you with her eyes. Consolable when mum holds her. | Appearance: mostly normal - brain is perfusing |
| Work of breathing | You hear inspiratory stridor from the door without a stethoscope. You can see mild suprasternal retraction. | Abnormal - upper airway obstruction |
| Circulation to skin | Pink skin, no mottling, no petechiae | Normal |
PAT interpretation: Abnormal work of breathing + normal appearance + normal circulation = Respiratory distress, child compensating. Not immediately life-threatening but needs assessment.
⚠️ Critical distinction: Layla is distressed but consolable. If she were toxic-appearing, sitting forward, drooling, and refusing to lie down → suspect epiglottitis not croup. Do NOT examine throat in that scenario.
VITAL SIGNS
| Sign | Finding | Meaning |
|---|---|---|
| RR | 34 breaths/min | Mildly elevated (normal ~24 at age 3) |
| HR | 126 bpm | Mildly elevated (normal ~117 at 3 years - consistent with distress) |
| Temp | 37.8°C | Low-grade fever |
| SpO₂ | 96% in air | Adequate but monitor |
| CRT | <2 sec | Normal perfusion |
HEAD & NECK
What you DO → What you FIND → What it MEANS:
| Step | Finding | Meaning |
|---|---|---|
| General head | No swelling, fontanelles not relevant (closed at 3 years) | Normal |
| Mouth - at distance only | Moist mucous membranes, no drooling | Reassuring - epiglottitis less likely |
| Voice quality | Hoarse voice when she speaks | Hoarse voice = laryngeal/subglottic involvement = croup |
| Neck | No neck stiffness, no lymphadenopathy >1 cm | No meningism, reactive nodes |
| Throat - defer | Do NOT instrument or aggressively examine the throat yet | If epiglottitis risk: can cause complete obstruction |
RESPIRATORY EXAM
What you DO: Undress upper body. Observe then auscultate.
| Finding | Meaning |
|---|---|
| Inspiratory stridor, musical, heard without stethoscope | Upper airway obstruction - subglottic (croup) |
| Mild suprasternal + supraclavicular recession | Increased negative intrathoracic pressure to pull air past obstruction |
| No intercostal/subcostal recession | Mild-moderate, not severe |
| No seesaw breathing, no head bobbing | Not impending respiratory failure |
| Auscultation: transmitted stridor throughout, clear air entry bilaterally, no wheeze, no crackles | Subglottic not lower airway - confirms croup, not bronchiolitis |
| Percussion: resonant | Normal |
Croup Severity Scoring (Westley Score simplified)
| Feature | Layla | Score |
|---|---|---|
| Stridor | At rest | 2 |
| Retraction | Mild (suprasternal) | 1 |
| Air entry | Normal | 0 |
| Cyanosis | None | 0 |
| Consciousness | Normal | 0 |
| Total | 3 = MODERATE CROUP |
(0-2 = mild; 3-7 = moderate; ≥8 = severe)
CARDIOVASCULAR & ABDOMEN
| Finding | Meaning |
|---|---|
| Heart: regular, no murmur, normal S1+S2 | No cardiac cause of distress |
| Abdomen: soft, non-tender, no organomegaly | Normal |
| Skin: no rash | No viral exanthem to suggest specific diagnosis, but consistent with parainfluenza |
🔍 LAYLA'S FINDINGS SUMMARY
| System | Finding | Flag |
|---|---|---|
| General | Scared but alert, consolable, pink | 🟢 Well-appearing |
| Vitals | Mild tachycardia, low-grade fever, SpO₂ 96% | 🟡 Monitoring needed |
| Voice | Hoarse | 🟡 Laryngeal involvement |
| Breathing | Inspiratory stridor, mild suprasternal recession, clear lungs | 🟡 Upper airway obstruction |
| Skin | Pink, warm, no rash | 🟢 |
Diagnosis: Moderate Viral Croup (Laryngotracheobronchitis)
Most likely causative agent: Parainfluenza virus
Management:
- Single dose oral/IM dexamethasone 0.15-0.6 mg/kg (reduces airway oedema, works within 30-60 min)
- If moderate-severe: nebulised adrenaline (epinephrine) 0.5 mL/kg of 1:1000, max 5 mL
- Nurse in position of comfort - do NOT force supine
- Reassess after 30 minutes
- Admit if stridor at rest persists, SpO₂ falls, severe recession develops
👦 SCENARIO 3: "Omar, 10 years old, right-sided abdominal pain for 18 hours"
Omar comes with his dad. Started with pain around his belly button yesterday. Now the pain has moved to the right side. He vomited twice. He doesn't want to eat. He walked into the room slowly and hunched slightly forward.
FROM THE DOOR — PAT
| Component | Finding | Meaning |
|---|---|---|
| Appearance | Omar is alert, talking to dad, answers your questions. Looks pale and uncomfortable. | Appearance: mildly abnormal - pain/systemic illness |
| Work of breathing | Normal rate, no recession | Normal |
| Circulation | Pale but no mottling, no rash | Mildly abnormal |
PAT: Mildly unwell. Stable enough for systematic examination. Not immediately life-threatening - but this presentation demands urgent assessment.
VITAL SIGNS
| Sign | Finding | Normal (10 years) | Meaning |
|---|---|---|---|
| Temp | 38.1°C | <37.5°C | Low-grade fever |
| HR | 108 bpm | ~87 (50th %ile) | Tachycardia - pain + early sepsis |
| RR | 20 breaths/min | ~21 | Normal |
| SpO₂ | 99% | ≥95% | Normal |
| CRT | 1.5 sec | <2 sec | Normal |
GENERAL INSPECTION
What you DO → What you FIND → What it MEANS:
| Observation | Finding | Meaning |
|---|---|---|
| Gait entering room | Walking hunched forward, slightly antalgic | Peritoneal irritation - straightening the abdomen stretches peritoneum and causes pain |
| Preferred position on couch | Lying still, knees slightly flexed | Flexion reduces abdominal wall tension - peritoneal irritation |
| Facial expression | Grimacing when moving, pale | Pain and systemic illness |
| Skin | Pale, no rash | Systemic effect of infection |
HEAD / EYES / MOUTH
| Finding | Meaning |
|---|---|
| Mucous membranes: slightly dry | Reduced oral intake ± vomiting - mild dehydration |
| No conjunctival pallor | No significant anaemia |
| Sclera: white | No jaundice |
| Tongue: furred | Non-specific, reduced intake |
CHEST
| Finding | Meaning |
|---|---|
| Clear air entry bilaterally, no wheeze | No respiratory pathology (right lower lobe pneumonia can mimic appendicitis - important to exclude) |
| Normal percussion | No consolidation |
| No tachypnoea | Respiratory not primary |
⚠️ Always auscultate the chest in a child with abdominal pain. Right lower lobe pneumonia frequently presents as right-sided abdominal pain in children - and treatment is completely different.
CARDIOVASCULAR
| Finding | Meaning |
|---|---|
| Tachycardia 108 bpm | Pain + early systemic inflammation |
| Normal S1+S2, no murmur | No cardiac pathology |
| Peripheral pulses normal | Adequate perfusion |
| CRT <2 sec | Not shocked |
ABDOMEN — The Key Section
Technique tips:
- Warm hands. Kneel to Omar's level.
- Ask "can you point with one finger where it hurts most?" → RIF
- Start palpation away from the pain (left iliac fossa first)
- Watch his FACE not your hands - his expression will tell you more
- Ask him to cough or take a deep breath while you observe
| Step | What you DO | What you FIND | What it MEANS |
|---|---|---|---|
| Inspection | Look at abdomen | Flat, moves with breathing, no distension, no scars | No obstruction, no perforation yet |
| Auscultation | 10 seconds per quadrant | Present, mildly hypoactive | Mild ileus - consistent with inflammation |
| Percussion | All 9 zones | Percussion tenderness RIF | Localised peritoneal irritation |
| Light palpation - LIF | Gentle superficial palpation | Soft, non-tender | Normal |
| Light palpation - RIF | Gentle superficial palpation | Guarding - involuntary muscle rigidity | Peritoneal irritation - appendix wall or peritoneum inflamed |
| Deep palpation - McBurney's point (1/3 from ASIS to umbilicus) | Press firmly and slowly | Maximal tenderness at McBurney's point | Appendicitis - 68% of cases have tenderness here |
| Rovsing's sign | Press left iliac fossa firmly | Pain felt in RIGHT iliac fossa (not left) | Referred peritoneal irritation = appendicitis |
| Rebound tenderness | Press RIF slowly, release suddenly | Pain worse on release | Peritoneal inflammation |
| Heel strike test | Ask Omar to stand on tiptoes and drop onto heels | RIF pain on landing | Peritoneal irritation (less distressing for child than rebound) |
| Jump test | Ask him to jump up and down | Worsening RIF pain | "The three most useful tests: cough, walk, and jump" - Tintinalli's |
| Psoas sign | Left lateral decubitus, extend right hip against resistance | RIF pain | Retrocaecal appendix irritating psoas muscle |
| Organomegaly | Palpate for liver/spleen | Not palpable | Normal |
| Hernial orifices | Inguinal rings bilaterally | No hernia | Normal - important to check |
| Testes (vital in boys) | Gentle palpation of scrotal contents | Non-tender, both testes present and normally positioned | Testicular torsion excluded - always check in boys with lower abdominal pain |
From Tintinalli's Emergency Medicine: "Assessing pain when the child coughs, walks, and jumps is useful for detecting peritoneal inflammation. Rebound tenderness and guarding are more common with perforation and may be absent in early appendicitis."
NEUROLOGY / MUSCULOSKELETAL
| Finding | Meaning |
|---|---|
| Alert and oriented | Normal CNS |
| Gait: antalgic, hunched | Peritoneal guarding |
| Normal tone and power | No neuromuscular pathology |
🔍 OMAR'S FINDINGS SUMMARY
| System | Finding | Flag |
|---|---|---|
| General | Pale, antalgic posture, hunched gait | 🟡 Unwell |
| Vitals | Low-grade fever, tachycardia, otherwise stable | 🟡 |
| Chest | Clear - pneumonia excluded | 🟢 |
| Abdomen | Maximal RIF tenderness, guarding, Rovsing's +, rebound +, positive jump/cough test | 🔴 Appendicitis |
| Testes | Normal - torsion excluded | 🟢 |
Diagnosis: Acute Appendicitis
Alvarado Score (MANTRELS) for Omar:
| Feature | Present? | Score |
|---|---|---|
| Migration of pain to RIF | Yes | 1 |
| Anorexia | Yes | 1 |
| Nausea/vomiting | Yes | 1 |
| Tenderness RIF | Yes | 2 |
| Rebound tenderness | Yes | 1 |
| Elevated temperature (>37.3°C) | Yes | 1 |
| Leukocytosis (to be confirmed) | Pending | 2 |
| Shift to left on WCC | Pending | 1 |
| Total | 7/10 = HIGH RISK |
Score ≥7 = high probability of appendicitis → urgent surgical referral
Management:
- IV access, blood tests: FBC (expect leukocytosis), CRP (elevated), U&E, LFTs, amylase, urine dipstick (exclude UTI/urolithiasis)
- IV fluid resuscitation (nil by mouth)
- Analgesia (do NOT withhold - does NOT mask signs)
- Ultrasound abdomen (first-line imaging in children - no radiation; appendix >6mm diameter + non-compressible = diagnostic)
- If US inconclusive + high clinical suspicion → CT or surgical exploration
- Urgent surgical consultation for appendicectomy
🎓 Master Comparison Table — The 3 Scenarios
| Feature | Ahmed (8m) | Layla (3y) | Omar (10y) |
|---|---|---|---|
| PAT | All 3 abnormal | WOB abnormal only | Mildly abnormal appearance |
| Key finding | Bulging AF + petechiae + neck stiffness | Inspiratory stridor + hoarse voice | RIF guarding + Rovsing's + migration |
| Diagnosis | Meningococcaemia | Moderate croup | Appendicitis |
| Do NOT do | Delay antibiotics for LP | Examine throat if epiglottitis suspected | Withhold analgesia |
| Do immediately | Benzylpenicillin IM/IV + O₂ | Dexamethasone ± nebulised adrenaline | Surgical consult + USS |
| Life-threatening risk | Death in hours if untreated | Complete airway obstruction if severe | Perforation + peritonitis if delayed |
🔑 The 5 Exam Rules That Apply to Every Child
| Rule | Why |
|---|---|
| 1. Assess from the door first | PAT saves lives - you know sick vs. well before touching |
| 2. Undress fully | Petechiae, recession, abdominal distension are missed through clothing |
| 3. Save upsetting exams last | Throat, ears, rectal exam - do these last or the child will cry through everything else |
| 4. Watch the face, not your hands | A child's grimace tells you more than your fingers |
| 5. Age-appropriate normal values | A HR of 168 is normal in a neonate but shock in a 10-year-old |
Discuss infectious disease in pediatrics upto their ideal management 80/20
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Excellent - I have comprehensive data from the Harriet Lane Handbook and Red Book directly. Now I can write the definitive 80/20 notes.
Pediatric Infectious Diseases — 80/20 Guide
The conditions that fill 80% of wards, clinics, and exams
THE MASTER FRAMEWORK
Before any specific disease, know these 4 universal rules of pediatric infectious disease:
| Rule | Principle |
|---|---|
| 1. Age defines the pathogen | A 2-week-old with meningitis ≠ a 5-year-old with meningitis - organisms differ completely |
| 2. Fever + age <28 days = emergency | Any fever ≥38°C in a neonate → full sepsis workup + empiric antibiotics. No exceptions. |
| 3. Viral > bacterial | Most pediatric respiratory and GI infections are viral. Antibiotics often NOT needed. |
| 4. Immunization gaps = high-yield diagnoses | The unimmunized child is your clue: Hib meningitis, epiglottitis, pertussis, measles |
SECTION 1 — CNS INFECTIONS
1.1 Bacterial Meningitis
The one you cannot miss.
Age-Based Pathogens (memorize this table)
| Age | Top Pathogens | Empiric Treatment |
|---|---|---|
| <1 month (neonate) | Group B Strep (GBS), E. coli, Listeria monocytogenes | Ampicillin + Cefotaxime (ceftriaxone contraindicated <1 month - displaces bilirubin) |
| 1-23 months | S. pneumoniae, N. meningitidis, GBS, H. influenzae | Vancomycin + Ceftriaxone |
| 2+ years | S. pneumoniae, N. meningitidis, H. influenzae | Vancomycin + Ceftriaxone |
"Initiate antibiotics as soon as the possibility of bacterial meningitis is considered; do not delay antibiotics for head CT or LP." - Harriet Lane Handbook, 23rd Ed
Clinical Presentation
- Neonates: fever OR hypothermia, lethargy, poor feeding, vomiting, high-pitched cry, bulging fontanelle, seizures (classic neck stiffness often ABSENT)
- Infants/children: fever + headache + neck stiffness + photophobia + vomiting
- Kernig's sign (can't extend knee from 90° hip flexion) + Brudzinski's sign (neck flex → hip flex) - unreliable <18 months
- Meningococcal disease: non-blanching petechiae/purpura = septicaemia - give penicillin IMMEDIATELY
Investigations
- LP (lumbar puncture): Gram stain, culture, CSF analysis
| Parameter | Normal | Bacterial | Viral | TB |
|---|---|---|---|---|
| Appearance | Clear | Turbid/cloudy | Clear | Fibrin web |
| WCC | <5 | >1000 (neutrophils) | 10-500 (lymphocytes) | 50-500 (lymphocytes) |
| Protein | 0.15-0.45 | ↑↑ (>1) | Mildly ↑ | ↑↑ |
| Glucose | >60% serum | Low (<40% serum) | Normal | Very low |
| Gram stain | Negative | Often positive | Negative | Negative |
- CT head before LP only if: immunocompromised, known CNS disease, papilloedema, focal neurological deficit - but DO NOT delay antibiotics for CT
Management
- Antibiotics immediately - vancomycin + ceftriaxone (>1 month)
- Dexamethasone 0.15 mg/kg IV q6h × 2 days: reduce hearing loss in H. influenzae meningitis; also benefit in pneumococcal meningitis in adults/older children. Give with FIRST antibiotic dose.
- Manage raised ICP: head of bed 30°, restrict fluids initially, avoid hypotonic fluids
- Seizure management: benzodiazepines acutely
- Duration: S. pneumoniae: 10-14 days | N. meningitidis: 5-7 days | GBS: 14-21 days | Listeria: 21 days
Meningococcal Septicaemia - separate emergency track
- Non-blanching rash + fever → give benzylpenicillin/ceftriaxone IM before transfer
- Dose: Benzylpenicillin: <1 year 300mg IM, 1-9 years 600mg IM, >10 years 1200mg IM
- Fluid resuscitation 20 mL/kg 0.9% NaCl bolus for shock
- PICU referral
- Chemoprophylaxis for close contacts: rifampicin or ciprofloxacin or ceftriaxone IM (single dose)
SECTION 2 — RESPIRATORY INFECTIONS
2.1 Upper Respiratory Tract Infection (URTI / Common Cold)
Most common childhood illness. Most important skill: knowing when NOT to treat.
- Cause: Rhinovirus (most common), coronavirus, RSV, parainfluenza, adenovirus
- Management: supportive only - fluids, paracetamol/ibuprofen for fever/discomfort
- No antibiotics: viral cause, antibiotics cause harm (resistance, C. diff, allergy)
- Average child has 6-8 URTIs per year - this is NORMAL
- Amber flag → consider bacterial secondary infection if: symptoms worsening after 5 days, fever persisting >5 days, localising symptoms (ear pain, facial pain)
2.2 Acute Otitis Media (AOM)
Most common reason antibiotics are prescribed in children.
Diagnosis
- Red, bulging, opaque tympanic membrane ± perforation with discharge
- +/- Fever, irritability, ear tugging (non-specific in infants)
- Must distinguish from otitis media with effusion (OME/"glue ear") - dull, amber TM, no acute infection, no antibiotics
Pathogens
S. pneumoniae, H. influenzae (nontypeable), M. catarrhalis
Management — The Key Decision Tree
AOM confirmed
↓
Age <6 months → ALWAYS TREAT with antibiotics
↓
Age 6-23 months, bilateral AOM → TREAT
↓
Age 6-23 months, unilateral AOM, NO otorrhoea, NO severe symptoms → Watchful waiting 48-72h
↓
Age ≥24 months, unilateral/bilateral AOM, NO severe symptoms → Watchful waiting 48-72h
↓
ANY AGE, severe symptoms (fever >39°C, otalgia >48h, toxic appearance) → TREAT
"Consider watchful waiting if: 6-23 months - unilateral AOM without otorrhea or severe symptoms; 24+ months - unilateral or bilateral AOM without otorrhea or severe symptoms" - Harriet Lane Handbook
Antibiotic choice
| Scenario | Drug | Duration |
|---|---|---|
| First line | Amoxicillin 80-90 mg/kg/day in 2 divided doses (high dose to overcome resistant pneumococcus) | 10 days (<2 years), 5-7 days (≥2 years) |
| Treatment failure at 48-72h | Amoxicillin-clavulanate 90 mg/kg/day | 10 days |
| PCN allergy (non-severe) | Cephalexin or cefdinir | 10 days |
| PCN allergy (severe/anaphylaxis) | Azithromycin × 5 days | 5 days |
| Recurrent AOM (≥3 in 6 months) | ENT referral for grommets | - |
2.3 Croup (Laryngotracheobronchitis)
Most common cause of acute upper airway obstruction in children.
Quick Facts
- Age: 6 months - 3 years (peak 2 years)
- Cause: Parainfluenza virus type 1 (most common), also types 2, 3, RSV, influenza
- Season: Autumn
- Pathology: Subglottic oedema → narrowed airway → turbulent flow → stridor
Clinical Features
- Barking "seal-like" cough (pathognomonic)
- Hoarse voice (laryngeal involvement)
- Inspiratory stridor (worsens with agitation)
- Low-grade fever
- Onset often at night after 1-2 days of mild URTI
- Child is ANXIOUS but CONSOLABLE - if toxic and drooling → think epiglottitis
Westley Croup Score
| Feature | 0 | 1 | 2 | 3 | 5 |
|---|---|---|---|---|---|
| Stridor | None | At rest (mild) | - | - | - |
| Retractions | None | Mild | Moderate | Severe | - |
| Air entry | Normal | Mildly decreased | Severely decreased | - | - |
| Cyanosis | None | - | With agitation | - | At rest |
| Consciousness | Normal | - | - | - | Altered |
- 0-2: Mild - manage at home
- 3-7: Moderate - treat, observe in ED
- ≥8: Severe - may need intubation
Management
| Severity | Treatment |
|---|---|
| All croup | Single dose oral dexamethasone 0.15-0.6 mg/kg (reduces oedema; onset 30-60 min; works for 24-48h) |
| Moderate-severe | Add nebulised adrenaline (epinephrine) 0.5 mL/kg of 1:1000, max 5 mL via face mask - onset 10-30 min, duration 2 hours (rebound possible) |
| Severe/impending failure | Humidified O₂, call anaesthetics, prepare for intubation; intubate with tube 0.5-1mm smaller than usual |
| Antibiotics | NOT indicated (viral cause) |
If child improves with nebulised adrenaline: observe 2-4 hours minimum for rebound. Discharge when stridor resolved and SpO₂ normal.
Epiglottitis vs. Croup - Critical Distinction:
| Feature | Croup | Epiglottitis |
|---|---|---|
| Age | 6m-3 years | Any (post-Hib vaccination: adolescents/adults) |
| Onset | Gradual (URTI prodrome) | Acute, rapid (hours) |
| Cough | Barking, harsh | Absent or muffled |
| Voice | Hoarse | Muffled "hot potato" voice |
| Drooling | Absent | Present (can't swallow) |
| Position | Any | Tripod/sniffing, REFUSES to lie flat |
| Fever | Low-grade | High (>39°C), toxic |
| Stridor | Inspiratory | Both inspiratory and expiratory |
| X-ray | Steeple sign (subglottic narrowing) | Thumbprint sign (enlarged epiglottis) |
| Action | Dexamethasone ± adrenaline | DO NOT examine throat. Call anaesthetics NOW. Secure airway in OR. |
2.4 Community-Acquired Pneumonia (CAP)
Age-Based Pathogens
| Age | Most Likely Pathogen |
|---|---|
| Neonate-3 months | GBS, E. coli (bacterial), RSV (viral), Chlamydia trachomatis (afebrile pneumonia, staccato cough) |
| 3 months-5 years | Viral (RSV, parainfluenza, adenovirus) most common; S. pneumoniae (bacterial), H. influenzae |
| 5-18 years | S. pneumoniae still important; Mycoplasma pneumoniae (atypical - "walking pneumonia"), Chlamydophila pneumoniae |
Clinical Features
- Fever + tachypnoea + cough ± hypoxia
- Decreased breath sounds, crackles, dullness to percussion (lobar pneumonia)
- Tachypnoea is the most sensitive sign (WHO diagnostic criterion)
WHO Tachypnoea Thresholds for Pneumonia Diagnosis
| Age | Tachypnoea threshold |
|---|---|
| <2 months | ≥60 breaths/min |
| 2-12 months | ≥50 breaths/min |
| 1-5 years | ≥40 breaths/min |
Management by Severity
| Setting | Antibiotic | Notes |
|---|---|---|
| Outpatient | High-dose amoxicillin × 5 days (80-90 mg/kg/day in 2 doses) | First-line for typical bacterial CAP in immunized children |
| Outpatient, atypical suspected (school age, subacute) | Amoxicillin + azithromycin OR azithromycin alone | Mycoplasma: azithromycin 10 mg/kg day 1, then 5 mg/kg days 2-5 |
| Inpatient | IV ampicillin 200 mg/kg/day ÷ q6h | Switch to oral when improving |
| Inpatient, PCN-resistant concern | IV ceftriaxone 50-100 mg/kg/day | |
| ICU | IV ceftriaxone + vancomycin/linezolid (empirical MRSA cover) | Consider S. aureus superinfection post-influenza |
| Viral CAP | Supportive only; oseltamivir if influenza confirmed within 48h |
Admit criteria:
- Age <3-6 months
- SpO₂ <92% in air
- Respiratory distress (recession, respiratory rate severely elevated)
- Failure to feed / dehydration
- Complications (empyema, effusion)
- Social concerns
"Respiratory viruses cause the majority of CAP, especially in young children; thus, antibiotic therapy may not be indicated for all patients." - Red Book 2021
2.5 Bronchiolitis
Most common lower respiratory tract infection in infants.
- Age: <2 years (peak <6 months)
- Cause: RSV (80%), also rhinovirus, parainfluenza, adenovirus, hMPV
- Season: Winter (October-March in northern hemisphere)
- Pathology: Inflammation + oedema + mucus plugging of bronchioles
Clinical Features
- 1-3 days URTI → wheeze + crackles + tachypnoea + recession
- Feeding difficulty (nose blocked, tachypnoeic)
- SpO₂ may drop
- Apnoea risk (especially in infants <2 months and ex-premature)
Management — The key is knowing what DOESN'T work
| Intervention | Evidence | Recommendation |
|---|---|---|
| Supportive care (O₂, feeds, fluids) | ✅ Effective | Do this |
| Oxygen (target SpO₂ ≥92%) | ✅ Effective | Do this |
| NG tube feeds if SpO₂ drops with feeding | ✅ Effective | Do this |
| Salbutamol (bronchodilator) | ❌ Multiple RCTs: no benefit | Do NOT use |
| Nebulised hypertonic saline | ❌ No benefit in ED | Not recommended |
| Antibiotics | ❌ Viral cause | Do NOT use routinely |
| Steroids | ❌ No benefit | Do NOT use |
| Chest physiotherapy | ❌ No benefit | Do NOT use |
Admit criteria:
- SpO₂ <92% persistently
- Respiratory rate severely elevated
- Feeding <50% normal
- Age <6 weeks, ex-premature
- Apnoea episodes
- Social concerns
Palivizumab prophylaxis: Monthly IM injection in RSV season for high-risk infants (ex-premature <29 weeks gestation, chronic lung disease, haemodynamically significant CHD)
2.6 Group A Streptococcal (GAS) Pharyngitis / Tonsillitis
Diagnosis - Use Centor/McIsaac Score
| Feature | Points |
|---|---|
| Exudate on tonsils | +1 |
| Tender anterior cervical lymph nodes | +1 |
| Fever (>38°C) | +1 |
| Absence of cough | +1 |
| Age 3-14 years | +1 |
| Age ≥45 years | -1 |
- Score ≤1: viral → no antibiotic, no swab
- Score 2-3: test with rapid antigen detection test (RADT) or throat swab → treat if positive
- Score ≥4: treat empirically
Rule: Antibiotics do NOT help viral pharyngitis. Stop prescribing for every sore throat.
Management
| Drug | Duration | Notes |
|---|---|---|
| Amoxicillin 50 mg/kg/day (max 500mg) twice daily | 10 days | First line; OR benzathine penicillin G IM single dose |
| PCN allergy (non-severe) | Cephalexin × 10 days | |
| PCN allergy (severe) | Clindamycin × 10 days | |
| Second-line | Azithromycin × 5 days | High resistance rates - use last |
Why treat? Prevent rheumatic fever (rare but devastating: cardiac valvular damage). Also reduces duration and infectivity.
Scarlet fever: GAS pharyngitis + diffuse sandpaper rash (spares face, accentuates flexures - Pastia's lines) + strawberry tongue → same treatment as above
Complications to know:
- Peritonsillar abscess: unilateral swelling, uvular deviation, trismus, "hot potato" voice → needle aspiration or I&D + antibiotics (amoxicillin-clavulanate or clindamycin), ENT referral
- Rheumatic fever: fever + migratory polyarthritis + carditis + Sydenham's chorea + erythema marginatum + subcutaneous nodules (Jones criteria) → penicillin + aspirin/naproxen
SECTION 3 — GASTROINTESTINAL INFECTIONS
3.1 Gastroenteritis
Most common cause: viral. Most important treatment: oral rehydration.
Pathogens by Context
| Pathogen | Clue |
|---|---|
| Rotavirus | Winter, unvaccinated child <5 years, profuse watery diarrhoea, vomiting |
| Norovirus | Any age, vomiting-predominant, explosive, school/daycare outbreaks |
| Salmonella | Raw eggs/poultry, can cause bloody diarrhoea, bacteraemia in young infants |
| Shigella | Bloody diarrhoea + fever, dysentery; seizures (Shigella toxin) |
| ETEC | Traveller's diarrhoea, watery |
| STEC O157:H7 | Undercooked beef, bloody diarrhoea, risk of HUS - DO NOT give antibiotics |
| Campylobacter | Bloody diarrhoea, poultry exposure, can mimic appendicitis (mesenteric adenitis) |
| C. difficile | Post-antibiotic diarrhoea; asymptomatic colonisation common in infants <12 months (do NOT test) |
Dehydration Assessment and Treatment
| Severity | % Dehydration | Action |
|---|---|---|
| Mild (3-5%) | <30-50 mL/kg deficit | ORS 50 mL/kg over 4 hours + ongoing losses |
| Moderate (5-10%) | 60-100 mL/kg deficit | ORS 100 mL/kg over 4 hours; if vomiting → NGT ORS |
| Severe (>10%) | >100 mL/kg deficit | IV fluid resuscitation 20 mL/kg 0.9% NaCl bolus then reassess, NGT when tolerating |
ORS (Oral Rehydration Solution): WHO formula - glucose 75 mmol/L, sodium 75 mmol/L, osmolarity 245 mOsm/L. Works via sodium-glucose cotransporter in enterocyte - survives even in secretory diarrhoea.
"Enteral rehydration is preferred to intravenous regardless of etiology." - Harriet Lane Handbook
Antibiotic Use in Gastroenteritis - The Rules
| Pathogen | Antibiotics? | If yes, drug |
|---|---|---|
| Viral (rotavirus, norovirus) | ❌ Never | - |
| Salmonella (non-typhi, non-invasive) | ❌ No - prolongs carriage | - |
| Salmonella (age <3 months, immunocompromised, bacteraemia) | ✅ Yes | Ceftriaxone or azithromycin 3-14 days |
| Shigella (severe, young infant) | ✅ Yes | Ceftriaxone × 2-5 days, azithromycin × 3 days |
| Campylobacter (severe) | ✅ Yes | Azithromycin × 3-5 days |
| STEC O157:H7 | 🚫 CONTRAINDICATED | Antibiotics increase HUS risk |
| C. difficile (symptomatic ≥12 months) | ✅ Yes | PO vancomycin (preferred) or metronidazole; discontinue offending antibiotic |
Ondansetron: Safe and effective antiemetic in children >6 months for vomiting with gastroenteritis - single oral dose 0.15 mg/kg improves ORS tolerance.
SECTION 4 — URINARY TRACT INFECTIONS
4.1 UTI in Children
Important because untreated UTI → renal scarring → chronic kidney disease
Pathogens
E. coli (80%), Klebsiella, Enterococcus, Staphylococcus saprophyticus (adolescent girls)
Clinical Features by Age
| Age | Presentation |
|---|---|
| Neonate/infant | Fever, poor feeding, lethargy, vomiting, jaundice, irritability - NO localizing signs |
| Toddler | Fever, abdominal pain, vomiting |
| School age | Frequency, dysuria, urgency, suprapubic pain (cystitis) OR fever + loin pain/CVA tenderness (pyelonephritis) |
| Adolescent girls | Classic LUTS (dysuria, frequency, urgency) |
Pyelonephritis vs. Cystitis:
- Pyelonephritis: fever >38°C + systemic illness + possibly loin pain / CVA tenderness
- Cystitis: LUTS without fever or systemic illness
Diagnosis
- Urine dipstick: nitrites (specific for gram-negative bacteria) + leucocyte esterase (WCC)
- Both positive → treat; both negative → UTI unlikely
- Urine culture: mandatory before starting antibiotics in children; ≥10⁵ CFU/mL = significant growth
- Collection method matters:
- Catheter specimen (CSU): most reliable for infants
- Clean catch midstream (MSU): older children
- Pad urine: high contamination rate - only for initial dipstick, not culture
- Suprapubic aspiration (SPA): gold standard in neonates
Treatment
| Setting | Drug | Duration |
|---|---|---|
| Cystitis, older child, outpatient | Trimethoprim 4 mg/kg twice daily OR nitrofurantoin 1 mg/kg four times daily | 3-7 days |
| Pyelonephritis, outpatient (well child >3 months) | Co-amoxiclav (amoxicillin-clavulanate) OR cephalexin OR trimethoprim | 7-10 days |
| Pyelonephritis, inpatient | IV ceftriaxone 50-75 mg/kg/day once daily | Until afebrile 24-48h, then switch to oral for total 10-14 days |
| Neonate (<1 month) | IV ampicillin + gentamicin (or ceftazidime) | 10-14 days IV |
After first UTI - Imaging:
- Renal ultrasound: all children <2 years with first confirmed UTI (within 6 weeks)
- MCUG (micturating cystourethrogram): only if USS abnormal, atypical UTI, or recurrent UTI - to detect vesicoureteric reflux (VUR)
- DMSA scan: 4-6 months after acute infection - detects renal scarring; recommended for recurrent UTI or severe VUR
Vesicoureteric Reflux (VUR)
- Retrograde flow of urine from bladder to ureter/kidney
- Grades I-V (V = most severe, into renal pelvis with reflux nephropathy)
- Low-grade (I-III): often resolves spontaneously; prophylactic trimethoprim in recurrent UTI
- High-grade (IV-V): urology referral; consider surgical correction
SECTION 5 — SKIN AND SOFT TISSUE INFECTIONS
5.1 Impetigo
- Cause: S. aureus (most common, produces bullous impetigo), S. pyogenes (GAS, non-bullous)
- Features: golden-crusted lesions (non-bullous) or fluid-filled bullae (bullous)
- Treatment: topical fusidic acid or mupirocin × 5-7 days for localised; oral flucloxacillin or cefalexin × 7 days for widespread/systemic symptoms; MRSA: clindamycin or trimethoprim-sulfamethoxazole
5.2 Cellulitis
- Spreading erythema, warmth, oedema, pain, fever
- Cause: S. pyogenes, S. aureus
- Periorbital cellulitis (pre-septal, no proptosis, no ophthalmoplegia): IV cefazolin or cephalexin (mild) → switch oral after 24h improvement
- Orbital cellulitis (post-septal): proptosis + restricted eye movement + pain on movement → CT orbit → IV ampicillin-sulbactam + vancomycin, SURGICAL EMERGENCY if abscess
- Standard cellulitis: flucloxacillin/cefalexin orally for mild; IV for moderate-severe
SECTION 6 — KAWASAKI DISEASE
The great mimicker - and the leading cause of acquired heart disease in children in developed countries.
Diagnostic Criteria (Classic KD)
Fever ≥5 days + ≥4 of the following 5 criteria (or fewer with coronary artery changes):
| Criterion | Feature | Memory |
|---|---|---|
| Conjunctivitis | Bilateral, non-purulent | |
| Rash | Polymorphous, trunk | |
| Adenopathy | Cervical, unilateral, >1.5 cm | |
| Strawberry tongue / oral changes | Erythema of lips, strawberry tongue, fissured lips | |
| Hands and feet | Erythema/oedema of palms+soles acutely; desquamation of fingertips at 2-3 weeks |
Mnemonic: CRASH or RASH + Fever >5 days
Why it Matters
- 25% of untreated children develop coronary artery aneurysms → myocardial infarction, sudden death
- Must treat within first 10 days to prevent coronary involvement
Management
"IVIG and high-dose aspirin have an additive effect and, when initiated within 10 days from onset of illness, can substantially decrease the progression to coronary artery dilation and aneurysm formation." - Rosen's Emergency Medicine
- IVIG 2 g/kg IV as a single infusion over 10-12 hours - given within first 10 days of illness
- High-dose aspirin 80-100 mg/kg/day in 4 doses during febrile phase → switch to low-dose aspirin 3-5 mg/kg/day once afebrile × 6-8 weeks (or longer if coronary aneurysms)
- Echocardiogram at diagnosis, 2 weeks, and 6-8 weeks
- If resistant (fever persists ≥36h after IVIG): second dose IVIG 2g/kg OR infliximab OR corticosteroids
SECTION 7 — NEONATAL INFECTIONS
Special population - any fever in a neonate (<28 days) = emergency.
Neonatal Sepsis
| Type | Onset | Pathogens | Key Risk Factors |
|---|---|---|---|
| Early onset (<72h) | Within 3 days | GBS, E. coli, Listeria | Maternal GBS+, prolonged rupture of membranes, prematurity, chorioamnionitis |
| Late onset (>72h) | 3 days-3 months | GBS, E. coli, S. aureus, coagulase-negative Staph (CONS - NICU) | NICU stay, lines, prematurity |
Presentation (any of these in neonate = act fast):
- Fever ≥38°C OR hypothermia <36°C
- Lethargy, hypotonia
- Poor feeding, vomiting
- Jaundice
- Grunting, tachypnoea, apnoea
- Bulging fontanelle, seizures
- Mottled/grey skin, prolonged CRT
Management
- Full septic screen: FBC, CRP, blood culture × 2, LP (CSF), urine (SPA/catheter), CXR
- Empiric IV antibiotics: Ampicillin + Gentamicin (or cefotaxime for suspected meningitis)
- Do NOT wait for results. Start within 1 hour of clinical suspicion.
- Duration: 7 days if blood culture positive, 48h rule-out if cultures negative and CRP trending down
Neonatal Herpes (HSV)
- Acquisition from maternal genital HSV during delivery (primary > recurrent)
- Presentation: vesicular rash, hepatitis, encephalitis
- Treat immediately with IV aciclovir 60mg/kg/day ÷ q8h × 14-21 days
SECTION 8 — FEVER WITHOUT A SOURCE (FWS)
Very common. Management depends entirely on age.
| Age | Action |
|---|---|
| <28 days (neonate) | Full septic screen (FBC, CRP, blood/urine/CSF cultures, CXR) + admit + empiric ampicillin + gentamicin. No exceptions. |
| 29-60 days | Blood culture + urine + CRP/PCT. Low-risk criteria (Rochester/NICE): if met, may observe without antibiotics. High-risk → LP + admit + antibiotics |
| 3-36 months, well-appearing, vaccinated | Urine dipstick (UTI most common serious bacterial infection). Observe. Investigate if fever >39°C persists >48h. |
| >3 years, well, vaccinated | Clinical assessment. Most viral. Watchful waiting. Investigate if prolonged. |
Rochester Low-Risk Criteria (for infants 29-60 days):
- Previously healthy
- No focal bacterial infection
- WCC 5,000-15,000; band count <1,500; UA <10 WBC/hpf; stool WBC <5/hpf if diarrhoea
SECTION 9 — VACCINE-PREVENTABLE INFECTIONS (HIGH YIELD)
Know these because the unvaccinated child is a key exam and real-world scenario:
| Disease | Cause | Key Features | Prevention |
|---|---|---|---|
| Measles | Paramyxovirus | Koplik spots → maculopapular rash (head → feet), 3 C's (Cough, Coryza, Conjunctivitis), fever, photophobia | MMR vaccine |
| Mumps | Paramyxovirus | Parotitis (bilateral) + orchitis (post-pubertal boys) + aseptic meningitis | MMR vaccine |
| Rubella | Togavirus | Mild rash, posterior cervical lymphadenopathy; devastating in 1st trimester pregnancy (CRS) | MMR vaccine |
| Pertussis (whooping cough) | Bordetella pertussis | Paroxysmal cough + inspiratory whoop + post-tussive vomiting + apnoea in infants | DTaP |
| Epiglottitis | H. influenzae type b | (see croup section above) | Hib vaccine |
| Chickenpox (VZV) | Varicella-zoster | Pruritic vesicular rash, crops at different stages simultaneously | Varicella vaccine |
Pertussis treatment: Azithromycin × 5 days (or erythromycin × 14 days) - reduces infectivity; limited clinical benefit after the paroxysmal stage begins. Treat all contacts.
Measles: Supportive + vitamin A supplementation (WHO recommendation, reduces severity and mortality in developing countries and vitamin A-deficient children)
THE MASTER 80/20 TABLE — Drugs Every Pediatric Clinician Must Know
| Condition | First-Line Drug | Dose Principle |
|---|---|---|
| Bacterial meningitis (>1 month) | Vancomycin + Ceftriaxone | Vancomycin 15 mg/kg q6h; Ceftriaxone 100 mg/kg/day |
| Bacterial meningitis (<1 month) | Ampicillin + Cefotaxime | Ampicillin 200-300 mg/kg/day |
| Meningococcaemia | Benzylpenicillin / Ceftriaxone | Benzylpenicillin IM: <1yr 300mg, 1-9yr 600mg, >10yr 1200mg |
| CAP (outpatient) | High-dose amoxicillin | 80-90 mg/kg/day ÷ BD |
| CAP atypical | Azithromycin | 10 mg/kg day 1, 5 mg/kg days 2-5 |
| Croup | Dexamethasone ± nebulised adrenaline | Dex 0.15-0.6 mg/kg PO once |
| AOM (antibiotic required) | High-dose amoxicillin | 80-90 mg/kg/day ÷ BD × 10 days (<2yr) |
| GAS pharyngitis | Amoxicillin | 50 mg/kg/day ÷ BD × 10 days |
| UTI cystitis | Trimethoprim or nitrofurantoin | Trimethoprim 4 mg/kg BD × 7 days |
| UTI pyelonephritis (inpatient) | IV Ceftriaxone | 50-75 mg/kg/day once daily |
| Kawasaki disease | IVIG + high-dose aspirin | IVIG 2 g/kg IV single dose |
| Neonatal sepsis | Ampicillin + Gentamicin | Ampicillin 200 mg/kg/day; Gentamicin once daily dosing |
| Neonatal HSV | IV Aciclovir | 60 mg/kg/day ÷ q8h × 14-21 days |
| C. difficile | PO Vancomycin | 10 mg/kg QDS × 10 days (preferred over metronidazole) |
| STEC O157:H7 | Supportive ONLY | ⛔ Antibiotics CONTRAINDICATED - increase HUS risk |
| Bronchiolitis | Supportive + O₂ | ⛔ No salbutamol, no steroids, no antibiotics |
Sources: Harriet Lane Handbook 23rd Ed (Johns Hopkins), Red Book 2021 (AAP), Rosen's Emergency Medicine, Harrison's Principles of Internal Medicine 22nd Ed, Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.