Filariasis diagnosis part in detail please
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full detailed response.
Filariasis - Diagnosis in Detail
Overview of Diagnostic Approach
A definitive diagnosis of filariasis can be made only by detection of the parasites, which can be difficult because adult worms in lymphatic vessels are largely inaccessible. Diagnosis is approached through several complementary methods: direct parasitologic detection, antigen testing, serology, molecular methods, and imaging.
1. Clinical Clues Prompting Investigation
Before any test, certain findings should raise suspicion:
- Residence in or travel to endemic areas (sub-Saharan Africa, South/Southeast Asia, South Pacific, Caribbean, parts of South America)
- Lymphadenopathy, lymphangitis, lymphedema, or elephantiasis
- Scrotal swelling / hydrocele
- Tropical pulmonary eosinophilia (TPE)
- Peripheral eosinophilia and elevated serum IgE - very common nonspecific findings
- More than 50% of microfilaremic patients with W. bancrofti have hematuria and/or proteinuria
2. Direct Parasitologic Detection (Microfilariae)
This is the cornerstone of traditional diagnosis.
A. Blood Film (Most Important)
Microfilariae circulate in peripheral blood and are detected on:
- Thick and thin blood smears stained with Giemsa or hematoxylin
- Examined directly under microscopy
Timing of blood collection is critical - it must match the periodicity of the species:
| Species | Periodicity | Optimal Collection Time |
|---|---|---|
| W. bancrofti (most areas) | Nocturnally periodic | 10 PM - 2 AM |
| W. bancrofti (Pacific Islands) | Subperiodic | Any time / afternoon peak |
| Brugia malayi (coastal) | Nocturnally periodic | 10 PM - 2 AM |
| Brugia malayi (forest) | Subperiodic | Any time |
| Loa loa | Diurnal | 10 AM - 2 PM |
| Mansonella ozzardi, M. perstans | Nonperiodic | Any time |
| Onchocerca volvulus, M. streptocerca | In skin, not blood | Skin snip (see below) |
B. Concentration Methods (for low parasitemia)
Simple smear may miss low-level microfilaremia. More sensitive methods include:
- Polycarbonate membrane/Nuclepore filter method - blood is passed through a cylindrical pore filter (pore size 3 μm) which traps microfilariae; stained and examined. Increased sensitivity.
- Knott's concentration technique - blood is centrifuged in 2% formalin; sediment examined. Useful especially for W. bancrofti.
- Membrane filter (millipore) - similar principle to Nuclepore filter
- Saponin lysis method - RBCs are lysed with saponin, then centrifuged and sediment examined
- Direct wet mount - microfilariae may be seen moving in direct mounts of blood or tissue fluid
C. Skin Snip Biopsy
Used for dermal microfilariae - applicable to:
- Onchocerca volvulus (river blindness)
- Mansonella streptocerca
A small bloodless skin snip (punch biopsy) is placed in saline and examined after 30-60 minutes for emerging microfilariae. Microfilariae in skin do not exhibit periodicity.
3. Identification of Microfilarial Species
Species identification is essential because treatment varies. Key morphologic features used:
| Feature | W. bancrofti | Brugia malayi | Loa loa |
|---|---|---|---|
| Sheath | Present (poorly stains with Giemsa; stains with hematoxylin) | Present (deep pink with Giemsa) | Present (pink with Giemsa; nuclei extend to tail tip) |
| Tail nuclei | Absent from tip | Two distinct solitary nuclei in tail tip | Extend to tip |
| Cephalic space | Not as long as wide; distinct nuclear column | - | - |
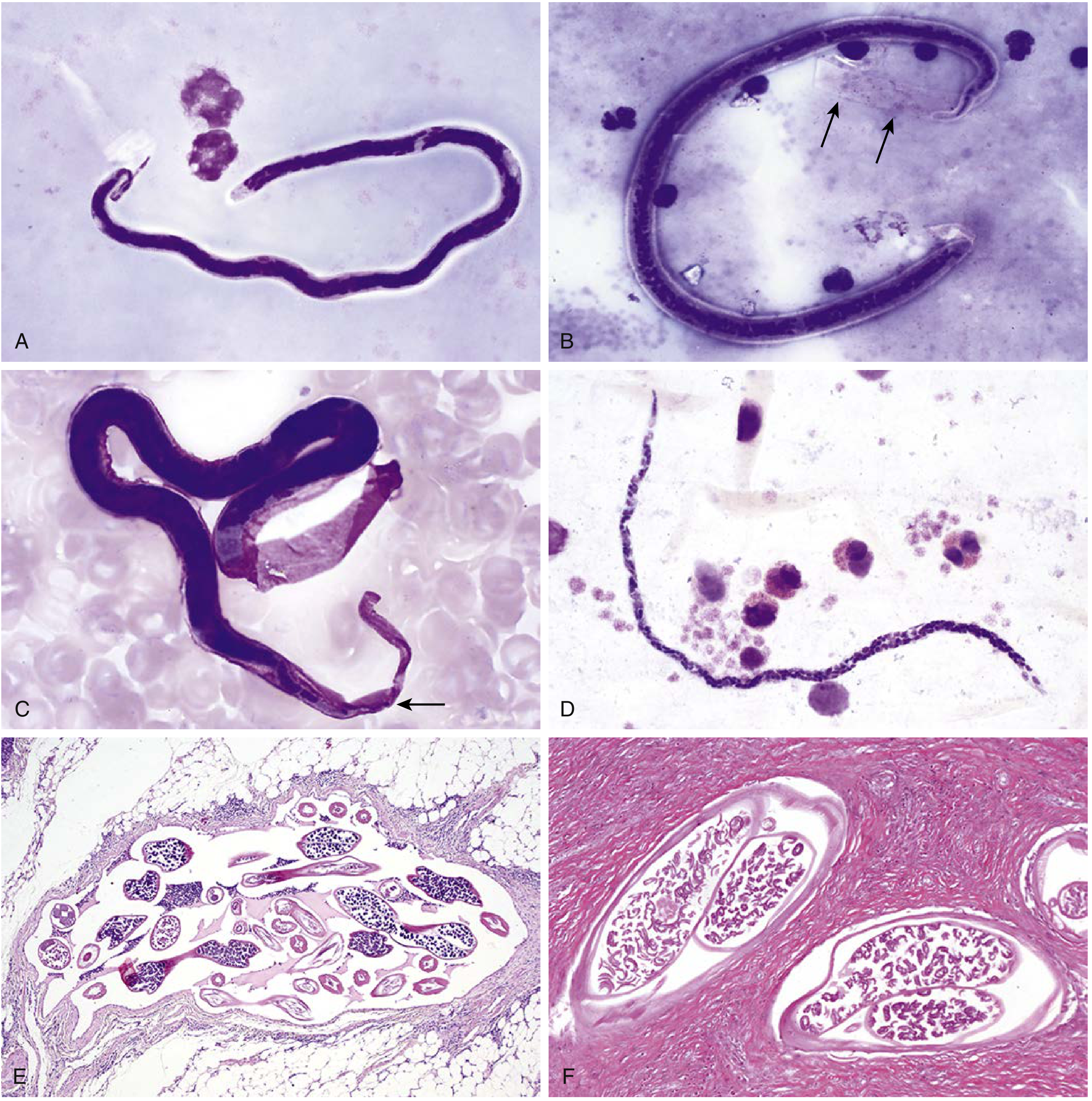
Figure: Giemsa-stained microfilariae (1000x) - A: Loa loa (sheathed, nuclei to tail tip); B: W. bancrofti (sheath seen as negative staining, no tail nuclei); C: Brugia malayi (deep pink sheath, 2 solitary tail nuclei); D: Mansonella perstans (unsheathed); E: W. bancrofti adult cross-section in lymphatics with fibrosis (H&E 20x); F: O. volvulus "double-barrel" uterus in skin nodule (H&E 100x). [Henry's Clinical Diagnosis and Management by Laboratory Methods]
4. Antigen Detection (Preferred for Bancroftian Filariasis)
Detection of circulating filarial antigen (CFA) is now the preferred method for diagnosis of Bancroftian filariasis. This overcomes the limitation of amicrofilaremic infection.
Available Assays:
- ELISA (enzyme-linked immunosorbent assay) - for circulating antigen of W. bancrofti
- Rapid-format lateral flow assay / Immunochromatographic card test (ICT) - includes the BinaxNOW Filariasis ICT and the newer Alere Filariasis Test Strip, which has shown better sensitivity in field conditions
Both assays have:
- Sensitivity: 93-100%
- Specificity: approaching 100%
- Can detect both microfilaremic AND cryptic (amicrofilaremic) infections
- False positives can occur in patients co-infected with Loa loa
Limitation: Currently, no circulating antigen tests exist for Brugian filariasis (B. malayi, B. timori).
For Brugia spp. - a dipstick test for IgG4 antibody specific for the Brugia antigen BmR1 can be used as an alternative.
5. Serology (Antibody Detection)
- Filarial serology is often very sensitive but nonspecific due to cross-reaction with other helminthic infections (e.g., other nematodes)
- Cannot reliably distinguish past exposure from current active infection
- A positive serologic test for bloodborne species should be followed up with:
- Blood examination for microfilariae
- Antigen test (to confirm active vs. past infection)
- Antifilarial antibody levels support diagnosis but are not confirmatory alone
- Particularly helpful in non-endemic visitors (travelers/"expatriate syndrome")
6. Molecular Diagnosis (PCR)
- PCR-based assays for DNA of W. bancrofti and B. malayi in blood have been developed
- Sensitivity is equivalent to or greater than parasitologic methods
- Currently mainly used in research settings; not routinely FDA-approved for clinical use in non-endemic countries
- Species-specific assays allow definitive speciation
7. Imaging
High-Frequency Ultrasound (with Doppler)
- Examination of the scrotum, lymph nodes, or breast (in women)
- Can identify motile adult worms within dilated lymphatics
- Live adult worms exhibit a distinctive movement within lymphatic vessels called the "Filarial Dance Sign"
- Worms can be visualized in lymphatics of the spermatic cord in up to 80% of men infected with W. bancrofti
- More commonly seen in men than women
- Lymph node biopsy is contraindicated - may worsen lymphatic damage
Lymphoscintigraphy (Radionuclide)
- Reliably demonstrates widespread lymphatic abnormalities in both:
- Subclinical microfilaremic persons
- Patients with overt lymphatic disease
- Useful for delineating anatomic changes; principally a research tool
- More widely used for assessment of lymphedema of any cause
Chest X-Ray
- May show infiltrates in individuals with lymphatic filariasis or tropical pulmonary eosinophilia (TPE) (bilateral diffuse interstitial infiltrates)
8. Supporting Laboratory Findings
| Finding | Significance |
|---|---|
| Peripheral eosinophilia (sometimes high-grade) | Common in all filarial infections |
| Elevated serum IgE | Common in all filarial infections |
| Hematuria / proteinuria | >50% of microfilaremic W. bancrofti patients |
| Elevated antifilarial antibody titers | Supportive; nonspecific due to cross-reactivity |
9. Adult Worm Detection
- Adult worms can occasionally be identified in tissue biopsy specimens (e.g., lymph node, subcutaneous nodule)
- For zoonotic Brugia infections in the Americas, immature worms are typically found in biopsy specimens
- Histopathology shows adult worms in dilated lymphatics with surrounding fibrosis (H&E cross-section)
- Onchocercal nodules (onchocercomas): adult O. volvulus worms found in subcutaneous palpable nodules; excision and histology show "double-barrel" uterus on cross-section
10. Diagnostic Algorithm Summary
Suspected Filariasis
|
├── Blood collection (timed per species periodicity)
| ├── Thick/thin smear (Giemsa/hematoxylin)
| └── Concentration methods if smear negative
| (Knott's / Nuclepore filter)
|
├── Species-specific antigen test
| ├── CFA ELISA or ICT strip → W. bancrofti (preferred)
| └── BmR1 IgG4 dipstick → Brugia spp.
|
├── If blood negative but suspected active infection:
| ├── Ultrasound (scrotum/lymphatics) → "Filarial Dance Sign"
| ├── PCR (research labs)
| └── Serology (rule out past infection)
|
├── Skin snip → O. volvulus / M. streptocerca
|
└── Supporting: Eosinophilia, IgE, hematuria/proteinuria
Key Points to Remember
- Bancroftian filariasis: CFA antigen test (ICT strip) is preferred; nocturnal blood collection for smears
- Brugian filariasis: BmR1 IgG4 test or timed blood smear; no commercial antigen test available
- Many symptomatic patients are amicrofilaremic - parasite detection alone is unreliable; antigen tests and ultrasound fill this gap
- Filarial dance sign on ultrasound - pathognomonic for living adult worms in lymphatics
- Lymph node biopsy is contraindicated
- Microfilariae appear in blood only 5-6 months after infection in loiasis - early infection may be parasitologically negative
- Eosinophilia + elevated IgE in a patient from an endemic area should always prompt filarial workup
Sources: Harrison's Principles of Internal Medicine 22E; Henry's Clinical Diagnosis and Management by Laboratory Methods; Fitzpatrick's Dermatology; Dermatology 2-Volume Set 5e; Robbins & Cotran Pathologic Basis of Disease; Park's Textbook of Preventive and Social Medicine
General identification features in clinical practice
Asking for Preferences
Of Filariasis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Excellent - I now have everything needed for a thorough, well-illustrated answer.
General Identification Features of Filarial Species in Clinical Practice
In clinical microbiology/parasitology, filarial species are identified on Giemsa-stained thick or thin blood smears (or skin snips) using five key morphologic criteria. These must be assessed together - no single feature alone is sufficient.
The Five Principal Identification Features
1. Sheath (Present or Absent)
The sheath is a remnant of the egg membrane that surrounds some microfilariae. It is the single most important first-pass discriminator.
| Sheathed | Unsheathed |
|---|---|
| W. bancrofti | O. volvulus |
| Brugia malayi | M. perstans |
| Brugia timori | M. ozzardi |
| Loa loa | M. streptocerca |
Sheath staining with Giemsa further differentiates sheathed species:
- W. bancrofti: Sheath transparent/unstained - visible only as a negative outline around the body; may be missed
- B. malayi: Sheath stains deep pink/bright pink - the most distinctive sheath staining feature
- B. timori: Sheath present but does NOT stain bright pink (unlike B. malayi)
- Loa loa: Sheath present, transparent (similar to W. bancrofti by Giemsa)
Practical tip: Hematoxylin stain reliably stains all sheaths, making them easier to identify when Giemsa is equivocal.
2. Tail Nuclei (Distribution to the Tip)
The pattern of nuclei in the posterior tail tip is the most reliable differentiating feature among the sheathed species.
| Species | Tail Nuclei Pattern |
|---|---|
| W. bancrofti | No nuclei in the tail tip - tip is clear, pointed |
| B. malayi | Two distinct, solitary nuclei at the tail tip (one subterminal, one terminal), separated by a gap from the nuclear column |
| B. timori | Two subterminal nuclei (similar to B. malayi, but larger body) |
| Loa loa | Nuclei extend all the way to the tail tip - continuous to the tip |
| M. perstans | Nuclei extend to the tail tip |
| M. ozzardi | No nuclei in the tail tip |
| O. volvulus | No nuclei in the tail tip |
3. Size (Length and Width)
Measured in stained smears. Smaller diameter species can be missed at lower magnification.
| Species | Length (stained film) | Notable |
|---|---|---|
| W. bancrofti | 244-296 μm | Moderate width |
| B. malayi | ~220-260 μm | Similar to W. bancrofti |
| B. timori | ~265-325 μm | Larger than B. malayi |
| Loa loa | 250-300 μm | Similar size |
| M. perstans | ~190-200 μm | Noticeably narrower/smaller than blood-dwelling species |
| M. ozzardi | ~175-240 μm | Narrow, small |
| O. volvulus | ~280-350 μm | In skin, not blood |
4. Cephalic Space (Head Region)
The cephalic space is the clear area at the anterior end before the nuclear column begins.
| Species | Cephalic Space |
|---|---|
| W. bancrofti | Short - not as long as it is wide (ratio ≤1); distinct nuclear column |
| B. malayi | Longer than it is wide (ratio >1) - a key differentiating point from W. bancrofti |
| Loa loa | Short cephalic space; irregular nuclei |
5. Nuclear Column Appearance
- W. bancrofti: Nuclei are discrete, distinct, well-separated in a clear column
- B. malayi: Nuclei are more crowded and irregular
- Loa loa: Nuclei are irregular and overlapping, difficult to count
- M. perstans: Nuclei extend to tip; no sheath; smaller diameter
Diagnostic Diagrams
Anterior and posterior ends of common human microfilariae (camera lucida drawings):
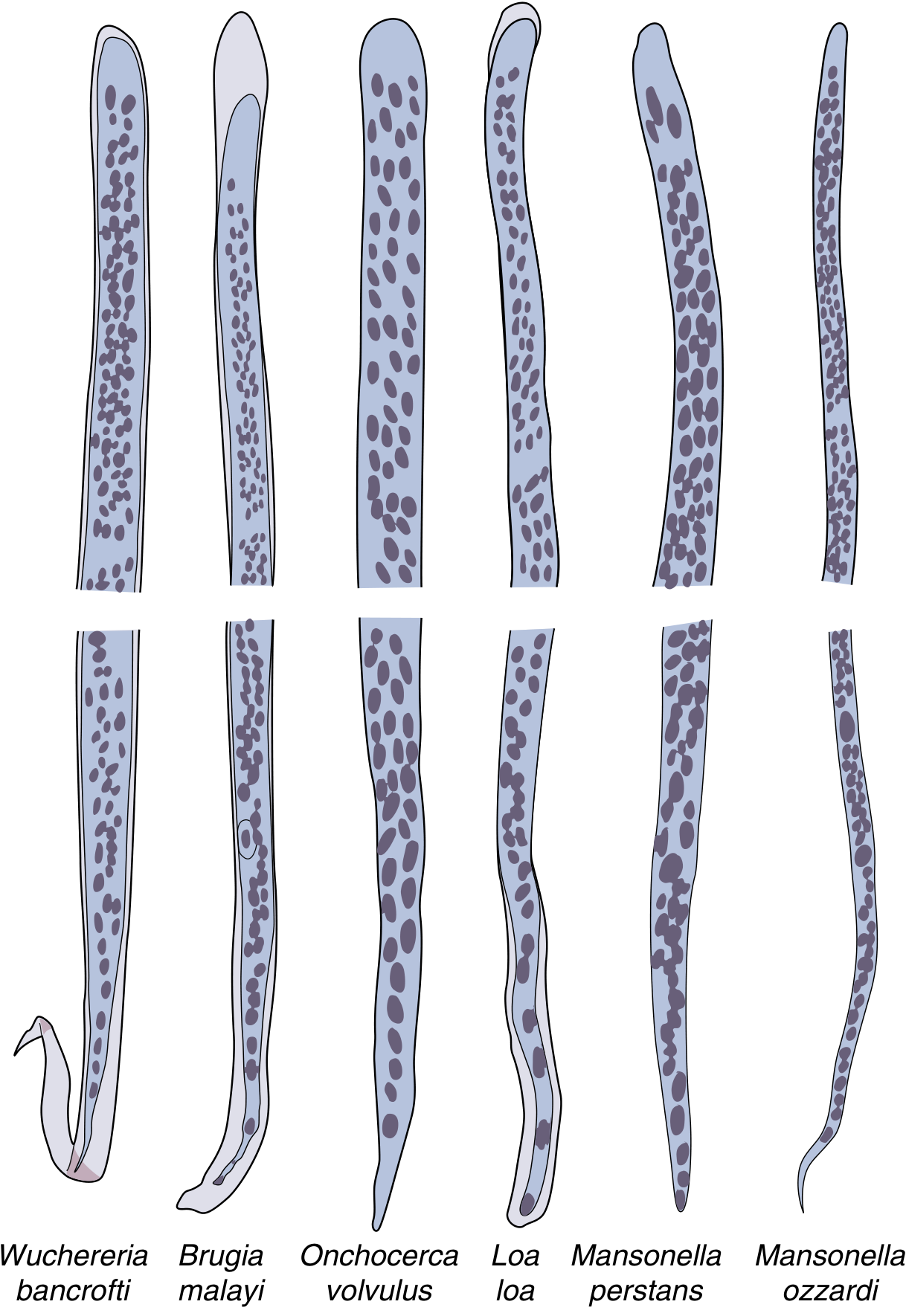
Anterior (top row) and posterior (bottom row) ends of microfilariae - W. bancrofti, B. malayi, O. volvulus, Loa loa, M. perstans, M. ozzardi. [Henry's Clinical Diagnosis and Management by Laboratory Methods]
Actual Giemsa-stained photomicrographs (1000x):
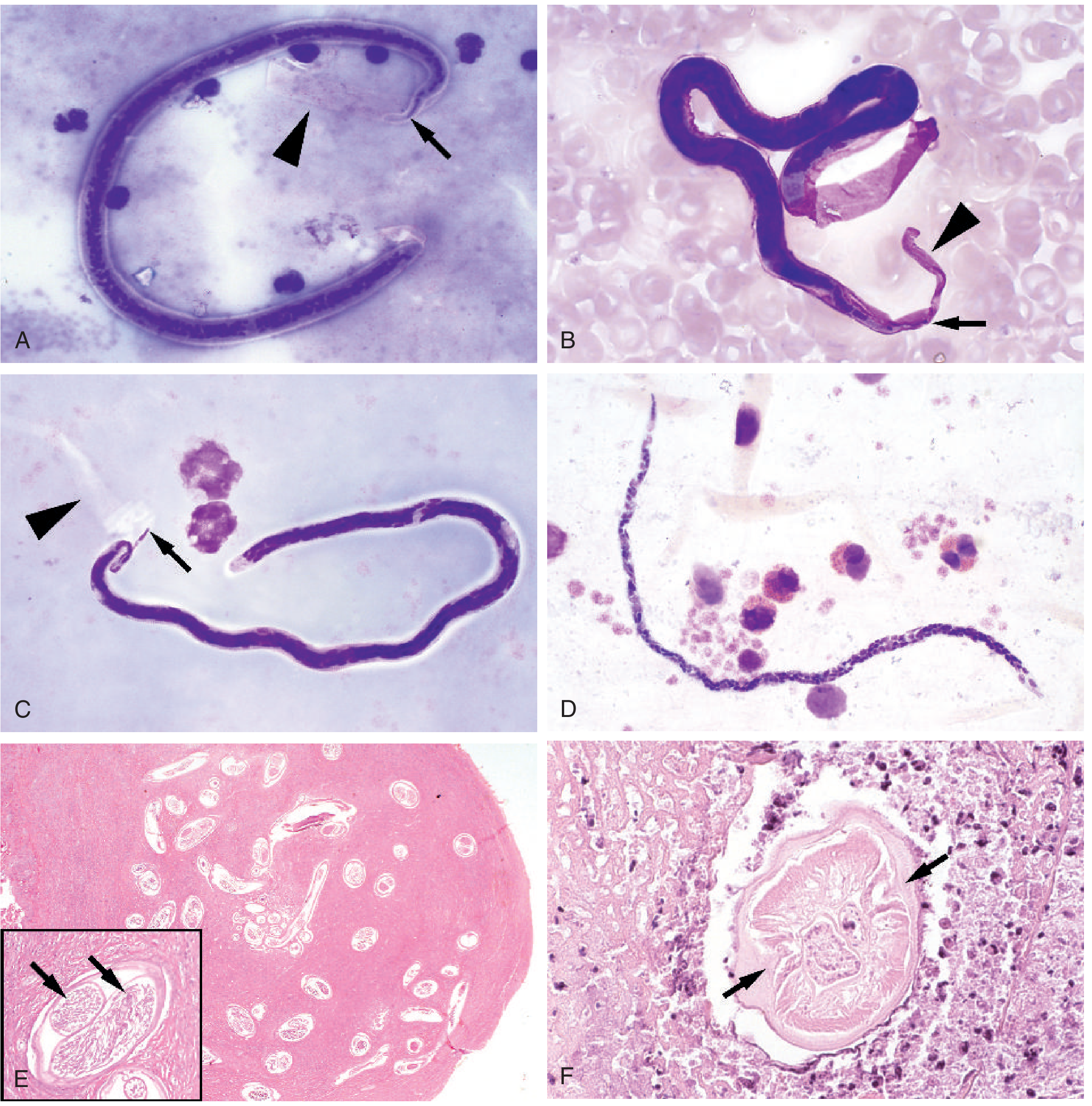
A: W. bancrofti - transparent sheath (arrowhead), tail nuclei absent (arrow); B: B. malayi - deep pink sheath, two spaced tail nuclei; C: Loa loa - transparent sheath, nuclei continuous to tip; D: M. perstans - no sheath, narrow diameter; E: Onchocerca nodule (H&E), inset shows "double-barrel" uterus; F: Dirofilaria pulmonary cross-section with lateral cuticular ridges. [Tietz Textbook of Laboratory Medicine 7e]
Comprehensive Species Identification Table
| Feature | W. bancrofti | B. malayi | B. timori | Loa loa | M. perstans | M. ozzardi | O. volvulus |
|---|---|---|---|---|---|---|---|
| Sheath | Yes | Yes | Yes | Yes | No | No | No |
| Sheath Giemsa stain | Transparent (negative outline) | Deep pink | Unstained (not pink) | Transparent | - | - | - |
| Tail nuclei | None at tip | 2 distinct (subterminal + terminal) | 2 subterminal | Extend to tip | Extend to tip | None at tip | None at tip |
| Cephalic space | Short (≤ width) | Long (> width) | Long | Short | Short | Short | Short |
| Nuclear column | Distinct, spaced | Crowded, irregular | Similar to B. malayi | Irregular, overlapping | Extends to tip | Sparse | - |
| Periodicity | Nocturnal | Nocturnal | Nocturnal | Diurnal | None | None | Not in blood |
| Specimen | Blood | Blood | Blood | Blood | Blood | Blood | Skin snip |
| Optimal collection | 10 PM-2 AM | 10 PM-2 AM | 10 PM-2 AM | 10 AM-2 PM | Any time | Any time | Any time |
| Adult location | Lymphatics | Lymphatics | Lymphatics | Subcutaneous | Serous cavities | Serous cavities | Subcutaneous nodules |
Adult Worm Identification Features (Histopathology)
When adult worms are found in tissue biopsy or nodule:
- W. bancrofti / Brugia spp.: Cross-section in lymphatic vessel shows adult worm with surrounding lymphatic dilation and fibrosis
- O. volvulus: Cross-section in subcutaneous nodule (onchocercoma) shows a distinctive "double-barrel" uterus - the paired uterine tubes are the hallmark on H&E
- Loa loa: Adult worm visible migrating under conjunctiva or excised from subcutaneous tissue; cuticle has random pimple-like projections (bosses)
- Dirofilaria spp. (zoonotic, non-human filaria): Cross-section in pulmonary granuloma shows longitudinal cuticular ridges - distinguishes from Loa loa which has bosses
Quick Clinical Memory Aid
Sheathed species → think "WBrBrLo" (W. bancrofti, B. malayi, B. timori, Loa loa)
Tail tip nuclei rule:
- "No nuclei at tip" = W. bancrofti, O. volvulus, M. ozzardi
- "Nuclei reach tip" = Loa loa, M. perstans
- "Two lonely nuclei at tip" = B. malayi (the unique pattern)
Pink sheath = B. malayi (the only one with a Giemsa-positive pink sheath)
Skin snip, not blood = O. volvulus, M. streptocerca
Diurnal blood = Loa loa only (draw at noon, not midnight)
Sources: Tietz Textbook of Laboratory Medicine 7e; Henry's Clinical Diagnosis and Management by Laboratory Methods; Harrison's Principles of Internal Medicine 22E
Find recent clinical images of filarial-infected tissue specimens
Finding Sources
Searching the Web
filariasis histopathology tissue specimen clinical images microfilariae lymph node
Loading Image
Loading Image
Loading Image
Loading Image
Searching the Web
filariasis tissue biopsy elephantiasis skin histology Wuchereria bancrofti lymphedema clinical photo
Loading Image
Loading Image
Loading Image
I now have a rich collection of clinical and histopathology images. Here is the curated gallery with annotations.
Clinical Images of Filarial-Infected Tissue Specimens
Here is a curated collection organized by specimen type and tissue involved.
1. Clinical Presentation - Elephantiasis of the Lower Extremity
Gross clinical photo - advanced filarial elephantiasis (W. bancrofti)

Elephantiasis of lower extremity - W. bancrofti infection. Left foot shows end-stage nodular, cobblestone deformity. Right leg shows earlier scaling and thickening. [Harrison's Principles of Internal Medicine 22E]
2. Breast Tissue - Adult Worm Cross-Sections (H&E, PathologyOutlines)
Low power (200 µm scale) - multiple filarial worm cross-sections in a dilated lymphatic channel within breast adipose tissue:
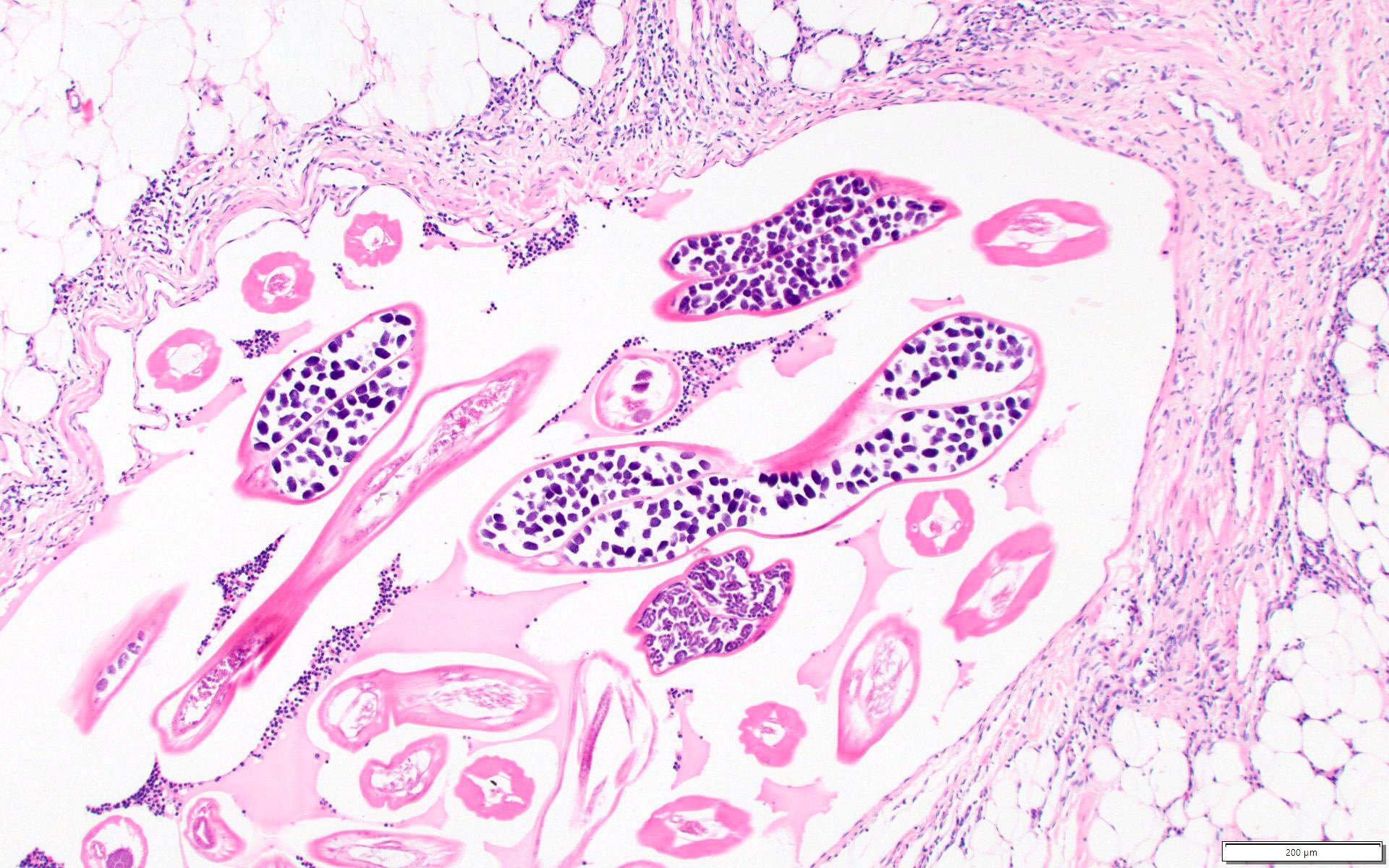
Breast biopsy H&E (200 µm): Dilated lymphatic vessel packed with multiple adult worm cross-sections showing internal structures, surrounded by fibrous stroma. Adipose tissue at periphery. Source: PathologyOutlines.com - Breast Filariasis
High power (50 µm scale) - female worm uterus packed with developing microfilariae:
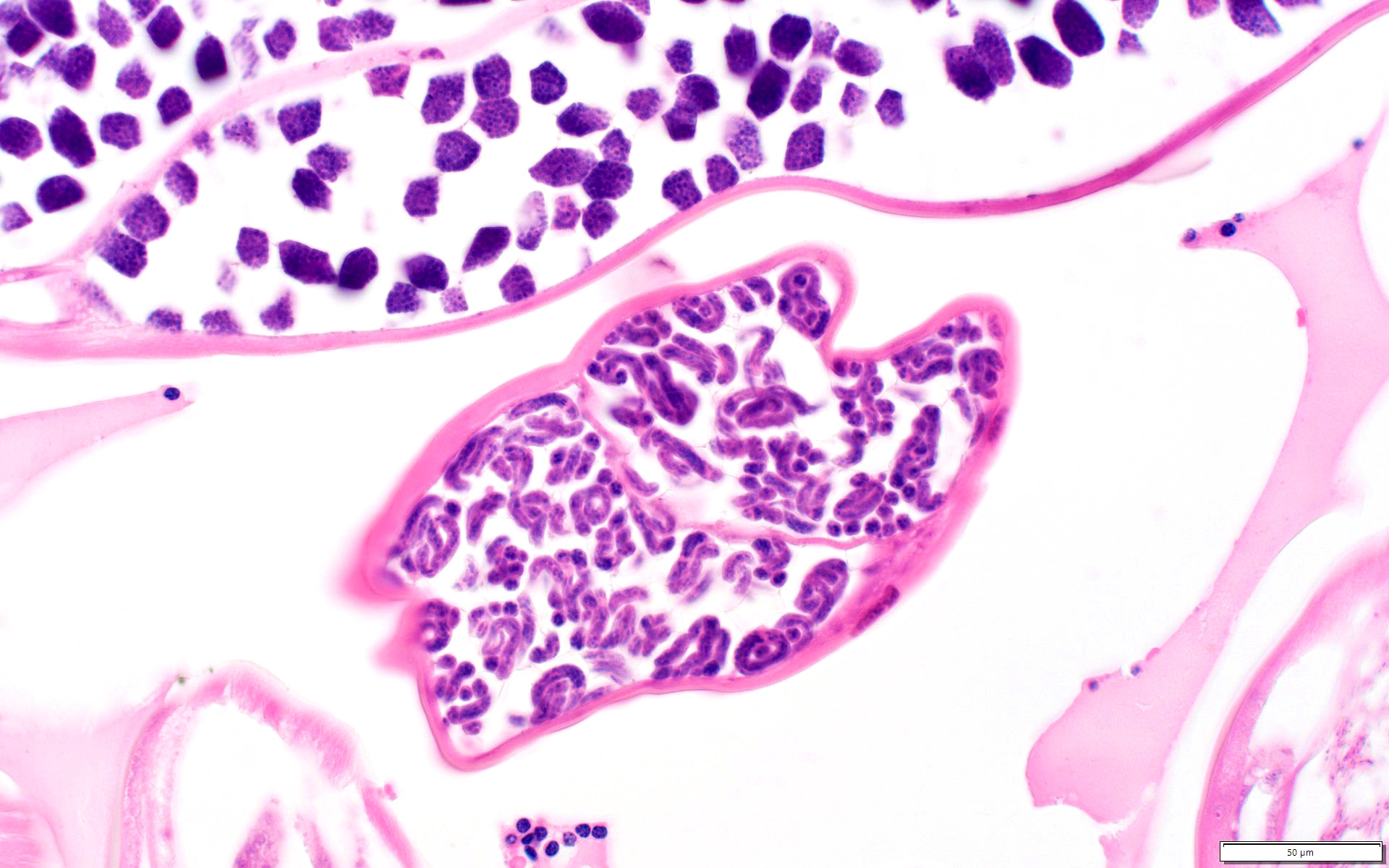
High magnification (50 µm): Female worm cross-section - the uterus is filled with tightly packed developing microfilariae (coiled profiles). Adjacent sections of male worm visible at top. Source: PathologyOutlines.com - Breast Filariasis
3. CDC Reference - Brugia Cross-Sections in Tissue (H&E)
Brugia sp. adult worm cross-sections - H&E tissue section:

Brugia sp. cross-sections in tissue H&E (50 µm). Note multiple body cross-sections showing internal anatomy including the prominent uterine tubes. [CDC DPDx - Lymphatic Filariasis]
Brugia sp. - lower power showing worms within lymphatic tissue:

Brugia sp. in lymphatic tissue H&E (100 µm). Multiple worm cross-sections embedded in fibrous tissue. [CDC DPDx - Lymphatic Filariasis]
4. Blood Smear - W. bancrofti Microfilaria (Thick Smear, Giemsa)
W. bancrofti microfilaria in thick blood smear:
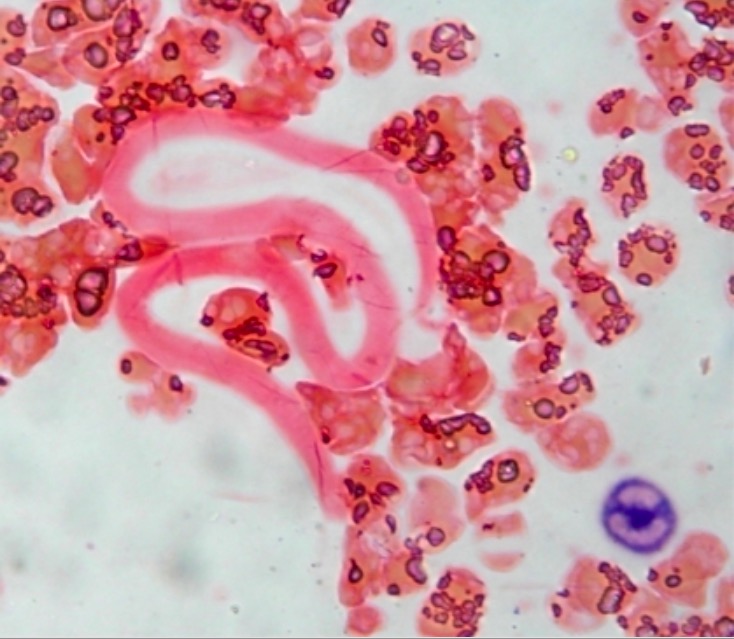
W. bancrofti microfilaria on Giemsa-stained peripheral blood smear. The sheathed microfilaria is coiled among RBCs. Note the pale staining of the transparent sheath. [Lecturio Medical Education]
5. Composite Histopathology Overview - India Panel
Multi-panel composite showing key filarial tissue findings:
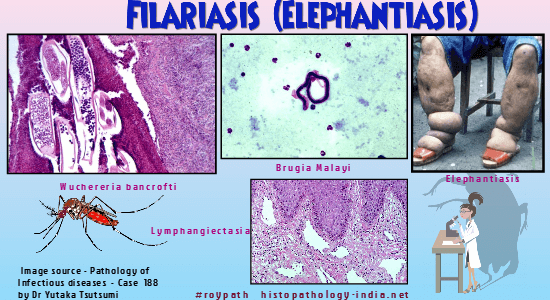
Composite panel: (Top-left) H&E - W. bancrofti adult cross-sections; (Top-center) Giemsa smear - B. malayi microfilaria (sheathed, with characteristic morphology); (Top-right) Clinical elephantiasis; (Bottom) H&E lymphangiectasia. [Histopathology-India.net / Pathology of Infectious Diseases]
What to Look for in Each Specimen Type
| Specimen | What You See |
|---|---|
| Blood smear (Giemsa) | Coiled/curved microfilaria among RBCs; sheath staining; tail nuclear pattern |
| Lymph node / lymphatic biopsy (H&E) | Adult worms in dilated lymphatics; fibrous thickening of vessel walls; inflammatory infiltrate |
| Breast / soft tissue (H&E) | Multiple worm cross-sections in lymphatic channel; female worm with uterus full of microfilariae |
| Skin snip (H&E) | O. volvulus - unsheathed microfilariae in dermis; nodule with "double-barrel" uterus |
| Clinical photo | Elephantiasis - progressive nodular skin thickening, lymphedema, cobblestone deformity |
Sources: Harrison's Principles of Internal Medicine 22E; PathologyOutlines.com; CDC DPDx Parasitology; Lecturio Medical Education; Histopathology-India.net
This is a shared conversation. Sign in to Orris to start your own chat.