i wanna know everything there is about isoniazid including its moa, metabolism, side effects, other adverse drug reactions, and the case reports about those ADRs how they were treated. what to do in a case of INH toxicity how to identify and treat? dosages ?other uses of INH? everything. i must be a pro in this.
isoniazid adverse effects hepatotoxicity
isoniazid overdose seizure treatment pyridoxine
isoniazid case report adverse reaction
PMID: 37125482
PMID: 39397742
PMID: 39270087
PMID: 41894632
isoniazid hepatitis DRESS skin reaction case
Isoniazid (INH) - Complete Reference Guide
1. OVERVIEW & CHEMISTRY
- Forms available: Tablets 100 mg, 300 mg; Syrup 50 mg/5 mL; Injection 100 mg/mL (10 mL)
- Generic names: INH, Nydrazid (no longer marketed), Laniazid
2. MECHANISM OF ACTION
- KatG activation: KatG oxidizes INH, generating an isonicotinoyl radical that then binds to NAD/NADP, producing about a dozen adducts.
- Primary target - InhA: The key adduct (nicotinoyl-NAD isomer) inhibits InhA (enoyl acyl-carrier protein reductase / acyl carrier protein reductase) and KasA (beta-ketoacyl-ACP synthase). Both enzymes are essential for mycolic acid synthesis - the long-chain fatty acids that form the mycobacterial cell wall. Blocking mycolic acid synthesis destroys cell wall integrity and kills the bacillus.
- Secondary target - DHFR: Another adduct (nicotinoyl-NADP isomer) potently inhibits mycobacterial dihydrofolate reductase (Kd < 1 nM), disrupting nucleic acid synthesis.
- Free radical damage: KatG activation also produces superoxide, H₂O₂, alkyl hydroperoxides, and nitric oxide radicals, all of which contribute to mycobactericidal effects. M. tuberculosis is especially vulnerable because it has a defect in oxyR, the central regulator of oxidative stress response.
3. ANTIMICROBIAL SPECTRUM & MICs
| Organism | Activity |
|---|---|
| M. tuberculosis | Excellent (MIC 0.025-0.05 mg/L in US clinical strains) |
| M. kansasii | First-line therapy |
| M. bovis | Moderate activity |
| M. avium complex (MAC) | Poor activity |
| All other bacteria | No activity |
4. MECHANISMS OF RESISTANCE
| Mutation | Mechanism | Resistance Level |
|---|---|---|
| KatG mutation/deletion (most common: Ser315Asn) | Loss of prodrug activation | High-level resistance |
| InhA overexpression | Target enzyme upregulation | Low-level resistance + cross-resistance to ethionamide |
| AhpC overexpression | Increased oxidative stress defense | Compensatory |
| kasA mutations | Additional target alteration | Variable |
| Efflux pump induction | Drug removal | Low-level |
5. PHARMACOKINETICS
5.1 Absorption
- Bioavailability: ~100% after oral 300 mg dose
- Food impairs absorption - take 1 hour before or 2 hours after meals (especially high-fat meals)
- Aluminum-containing antacids decrease absorption
- Can be given IM at the same doses as oral when oral route is impossible
5.2 Distribution
- Diffuses freely into all body fluids, cells, and caseous (necrotic) material in TB lesions
- CSF concentrations equal serum concentrations - one of the few TB drugs to penetrate CSF reliably
- Protein binding: ~10%
- PK described by a two-compartment model
5.3 Metabolism - The NAT2 Story
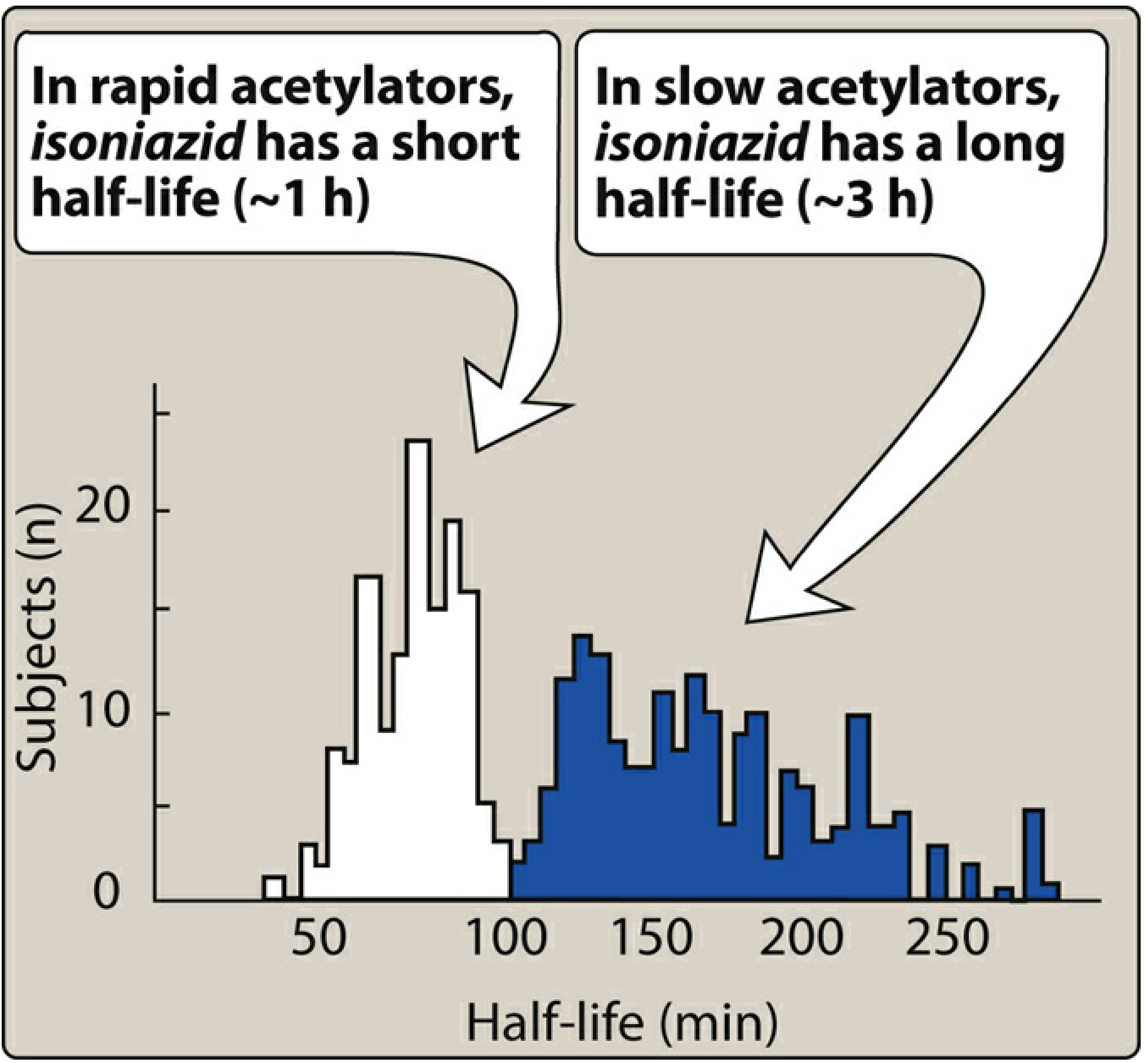
| Parameter | Rapid Acetylators | Slow Acetylators |
|---|---|---|
| Half-life | ~1-1.5 hours | ~3-4 hours |
| Peak serum Cp | ~2 µg/mL | ~4 µg/mL |
| NAT2 gene | Dominant trait (homozygous or heterozygous) | Recessive |
| Risk | Under-treatment, relapse, resistance | Peripheral neuropathy, toxicity |
| Prevalence | Common in Inuit, Japanese | Common in Scandinavians, North Africans, Jews |
5.4 Metabolic Pathway (Hepatotoxicity Pathway)
INH
└─► NAT2 ─────────────────► Acetylisoniazid (AcINH)
│
├─► Renal excretion (inactive)
│
└─► Acetylhydrazine (AcHz)
│
┌──────────────┴──────────────┐
▼ ▼
CYP2E1 (slow acetylators/ NAT2 (rapid acetylators)
CYP2E1 induction) │
│ ▼
▼ Diacetylhydrazine
REACTIVE HEPATOTOXIC (NON-TOXIC)
METABOLITES ── liver injury
5.5 Excretion
- 75-95% of a dose excreted in urine within 24 hours, primarily as acetylisoniazid and isonicotinic acid
- Slow acetylators excrete more unchanged parent drug
- Dose adjustment required in renal failure (see below)
6. DOSING
6.1 Active Tuberculosis Treatment
| Population | Dose | Frequency | Notes |
|---|---|---|---|
| Adult | 5 mg/kg (max 300 mg) | Once daily | Part of HRZE regimen |
| Adult | 15 mg/kg (max 900 mg) | 3x weekly | With rifampin for compliant patients |
| Child/Infant | 10-15 mg/kg (max 300 mg) | Once daily | Uncomplicated pulmonary TB |
| Child/Infant | 20-30 mg/kg (max 900 mg) | 3x weekly | With rifampin |
6.2 Latent TB Infection (LTBI) Treatment Regimens
| Regimen | Dose | Duration | Notes |
|---|---|---|---|
| INH alone | 300 mg/day (5 mg/kg) | 6-9 months | 9 months preferred for HIV+ |
| INH alone (twice weekly) | 900 mg (15 mg/kg) | 6-9 months | Requires directly observed therapy (DOT) |
| INH + Rifapentine (3HP) | 900 mg INH + 900 mg rifapentine weekly | 3 months | Preferred for adults and children >2 yrs; DOT recommended |
| INH + Rifampin (3HR) | 300 mg/day + 600 mg/day | 3 months | Higher hepatotoxicity risk than individual drugs alone |
6.3 Pyridoxine Supplementation
- Always give pyridoxine (B6) 25-50 mg/day with INH for LTBI treatment
- Children: 1-2 mg/kg/24 hr supplemental pyridoxine for prevention of neuropathy
- High-risk groups requiring pyridoxine: pregnant women, alcoholics, diabetics, malnourished patients, HIV-positive individuals, elderly
6.4 Dose in Renal Failure
- Adjust dose in renal failure - see Chapter 31 of Harriet Lane or nephrology references
- Renally cleared metabolites can accumulate
7. ADVERSE EFFECTS
7.1 Hepatotoxicity - The Most Serious ADR
- Asymptomatic ALT elevation: 10-36% of patients in the first 10 weeks (often transient, normalizes spontaneously even if INH continued)
- Clinical hepatitis: ~2% of patients overall
- Fatal hepatitis: 5-10% of clinical hepatitis cases
- Severe hepatic injury (all patients): ~0.1%
- Age: Risk increases with age - 0.3% in 3rd decade, rises to 2%+ after age 50
- Sex: Overall rates equal in men/women, but 70% of fatal cases are women; Black and Hispanic women at particular risk
- Alcohol: Chronic excess alcohol markedly increases frequency and severity
- Concurrent drugs: Rifampin + pyrazinamide combination increases risk; acetaminophen also increases risk (CYP2E1 induction)
- HIV infection: Higher risk due to NASH, polypharmacy
- Chronic hepatitis B or C: Some (not all) studies show increased risk
- Malnutrition: Contributory in some countries
- Dose/level: Risk is NOT related to dose or blood level
- Latent period: 1 week to >6 months (median 8 weeks)
- Most cases: 4-8 weeks after start of therapy
- Prodrome (1/3 of patients): malaise, fatigue, anorexia, nausea, vomiting
- Jaundice appears days later
- Fever, rash, arthralgias, eosinophilia: uncommon (unlike typical drug hypersensitivity)
- ~10% present with jaundice as the only feature
- Hepatocellular pattern: elevated AST/ALT (AST exceeds ALT in ~50%)
- Elevated bilirubin - values >10x ULN indicate poor prognosis
- Prolonged PT in 1/3 of patients - 60% of these cases were fatal
- Liver histology: focal hepatocellular injury, hydropic change, zonal/submassive/massive necrosis; inflammation in portal tracts
- LTBI with INH: Discontinue if ALT ≥5x ULN (or ≥3x ULN with symptoms), or bilirubin reaches jaundice levels (>2x ULN). Consider alternative agent on normalization.
- Active TB with INH: Stop H, Z, R and other hepatotoxic drugs if ALT >5x ULN or >3x ULN with hepatitis symptoms. Obtain alcohol history, check viral hepatitis serologies. Rechallenge: reintroduce R and H sequentially once enzymes normalize; Z often not restarted.
7.2 Peripheral Neuropathy (Pyridoxine-Deficiency Neuropathy)
- GABA synthesis (key - see toxicity section)
- Aminotransferases
- Amino acid metabolism
- Slow acetylators (higher drug levels)
- Diabetes mellitus
- Poor nutrition / malnutrition
- Anemia
- HIV infection
- Alcoholism
- Pregnancy
7.3 CNS Toxicity
- Convulsions (especially in patients with pre-existing seizure disorders)
- Optic neuritis and optic atrophy
- Muscle twitching
- Dizziness, ataxia
- Paresthesias, stupor
- Toxic encephalopathy
- Psychiatric: euphoria, transient memory impairment, loss of self-control, florid psychoses
7.4 Hypersensitivity Reactions
- Drug fever: can occur
- Skin reactions: morbilliform rash, urticaria
- Drug-induced lupus erythematosus (DIL): Vasculitis with antinuclear antibodies (ANA) appearing during treatment; resolves when drug stopped
- Arthritic syndromes: Arthralgia, arthritis attributed to INH
- DRESS syndrome (Drug Reaction with Eosinophilia and Systemic Symptoms): Rare but life-threatening - see case reports below
7.5 Hematological ADRs
- Sideroblastic anemia: INH is a recognized cause (along with chloramphenicol, linezolid). Mechanism: pyridoxine depletion disrupts heme synthesis. Responds dramatically to high-dose vitamin B6.
- Agranulocytosis (rare)
- Thrombocytopenia (rare)
- Hemolytic anemia in G6PD-deficient patients
7.6 Other ADRs
- GI: Epigastric distress, nausea, vomiting
- Methemoglobinemia
- Tinnitus
- Urinary retention
- Dryness of mouth
- Pancreatitis (reported, rare)
- Toxic epidermal necrolysis (TEN) (rare - reported in children and adults)
- False-positive urine glucose test
- Gynecomastia (rare)
7.7 Ocular Toxicity
- Optic neuritis (dose-dependent at higher doses; less common at standard doses)
- This is a class effect shared with ethambutol
8. DRUG INTERACTIONS
| Coadministered Drug | CYP Involved | Consequence |
|---|---|---|
| Phenytoin | CYP2C19 inhibition | INH inhibits phenytoin metabolism → phenytoin toxicity (nystagmus, ataxia) - classic exam interaction |
| Carbamazepine | CYP3A inhibition | Neurological toxicity from carbamazepine accumulation |
| Diazepam | CYP3A + CYP2C19 inhibition | Sedation, respiratory depression |
| Ethosuximide | CYP3A inhibition | Psychotic behaviors |
| Acetaminophen | CYP2E1 induction | Increased hepatotoxicity (more toxic acetaminophen metabolites) |
| Isoflurane/Enflurane | CYP2E1 induction | Decreased anesthetic effectiveness |
| Prednisone | Prednisone may decrease INH effects | Reduced INH efficacy |
| Rifampin | Combined hepatotoxic effect | Increased hepatotoxicity risk |
| Warfarin | CYP2C9 inhibition (indirect) | Enhanced anticoagulant effect |
| Aluminum antacids | Absorption interference | Decreased INH absorption |
9. INH TOXICITY / OVERDOSE
9.1 The Classic Triad of INH Overdose
- Seizures - generalized tonic-clonic, refractory to standard anticonvulsants
- Anion gap metabolic acidosis - refractory to sodium bicarbonate
- Coma
9.2 Timeline
- Early symptoms begin 30 minutes to 3 hours after ingestion
- Initial: nausea, mental status changes, ataxia, peripheral neuropathy, dizziness, slurred speech
- Progression: grand mal seizures, metabolic acidosis, coma
9.3 Dose-Toxicity Correlation
- As little as 1.5 g can be toxic
- Seizures typically follow ingestions of >20-30 mg/kg
- Mortality at doses ≥30 mg/kg: up to 20%
9.4 Pathophysiology of Seizures
9.5 Pathophysiology of Metabolic Acidosis
9.6 Treatment of INH Overdose
| Scenario | Dose |
|---|---|
| Known amount of INH ingested | Gram-for-gram: give same mg of pyridoxine IV as mg of INH ingested |
| Unknown amount ingested - adult | 5 grams IV |
| Unknown amount ingested - child | 70 mg/kg IV (maximum 5 g) |
| Administration rate | 1 g IV every 2-3 minutes until seizures stop or max dose given |
| After seizures stop | Give remainder of dose over 4-6 hours to prevent recurrence |
| If seizures persist after full dose | Pyridoxine dose may be repeated |
| If only tablets available | Crush and administer via NG tube |
- Phenytoin has NO role in INH-induced seizures
- Sodium bicarbonate does NOT help the metabolic acidosis
- Pyridoxine may reverse INH-induced coma (not just seizures)
- Hemodialysis has been reported to clear INH (case reports exist)
- If patient is asymptomatic at 6 hours post-ingestion in the ED, it is safe for medical clearance
10. MONITORING GUIDELINES
10.1 Baseline
- All adults starting INH for active TB: ALT, bilirubin, platelets, creatinine, hepatitis panel
- Adults starting LTBI with hepatic risk factors: baseline ALT and bilirubin
- Risk factors for hepatic monitoring: age >35, alcohol use, chronic liver disease, HBV/HCV, HIV, pregnancy
10.2 Ongoing
- Routine biochemical monitoring not required for uncomplicated LTBI treatment
- Patients with hepatic risk factors: monthly ALT and bilirubin
- Active TB: monthly clinical assessment for nausea, vomiting, abdominal pain, fatigue, jaundice, dark urine, pale stools
- Monthly dispensing of TB medications allows essential clinical monitoring
10.3 Stop/Continue Rules
| Situation | Threshold | Action |
|---|---|---|
| LTBI - asymptomatic | ALT ≥5x ULN | Stop INH |
| LTBI - symptomatic | ALT ≥3x ULN | Stop INH |
| Active TB | ALT >5x ULN | Stop H, Z, R, all hepatotoxics |
| Active TB - with hepatitis symptoms | ALT >3x ULN | Stop H, Z, R |
| Either - bilirubin | >2x ULN (jaundice level) | Stop INH |
11. CONTRAINDICATIONS
- Acute liver disease
- Previous isoniazid-associated hepatitis (absolute contraindication)
- Hypersensitivity to INH
12. OTHER USES OF INH (Beyond Standard TB)
| Indication | Notes |
|---|---|
| Latent TB infection (LTBI) treatment | All regimens listed above; 6H, 9H, 3HP, 3HR |
| M. kansasii infection | First-line therapy |
| TB meningitis | One of the drugs of choice due to excellent CSF penetration |
| Miliary tuberculosis | Part of standard 4-drug regimen |
| Extrapulmonary TB (bone, joint, renal, pericardial, lymph node) | Part of standard regimen |
| HIV + TB co-infection | Used with modification for drug interactions |
| MDR-TB (some cases) | Low-level resistance strains may still respond; role limited |
| Prophylaxis in close contacts | After exposure assessment |
13. SPECIAL POPULATIONS
13.1 Pregnancy
- INH is generally used during pregnancy when indicated (TB risk outweighs drug risk)
- 3HP (INH + rifapentine) is NOT recommended in pregnant women (insufficient safety data)
- Pyridoxine supplementation is especially important during pregnancy
- 2026 systematic review/meta-analysis (PMID: 41824367) examined outcomes of INH preventive therapy in pregnant women with HIV - data continue to evolve
13.2 Children
- INH is generally safe and well-tolerated in children
- Severe liver injury has been reported (uncommon but documented)
- A 2023 meta-analysis (PMID: 37125482) found pediatric populations have very low AE incidence with all LTBI regimens
- Supplemental pyridoxine 1-2 mg/kg/day for all children on INH
13.3 HIV-Positive Patients
- Higher risk of hepatotoxicity (NASH, polypharmacy)
- Monthly liver function monitoring required
- 9 months of INH may be more effective than 6 months for HIV-positive LTBI
- Drug interactions with antiretrovirals (especially PIs and NNRTIs): INH CYP inhibition can affect ARV levels
13.4 Renal Impairment
- Dose adjustment required (consult formulary for specific GFR thresholds)
- Metabolites accumulate in renal failure
14. CASE REPORTS OF NOTABLE ADRs AND THEIR MANAGEMENT
Case 1: INH Overdose with Hypersensitivity Myocarditis (PMID: 39397742, Cardiology in the Young, 2024)
Case 2: DRESS Syndrome from Anti-TB Drugs including INH (PMID: 41894632, Int J Mycobacteriol, 2026)
- Discontinue all anti-TB drugs
- Systemic corticosteroids
- Hepatoprotective agents
- Topical therapy
- Supportive respiratory management
- ATD desensitization on clinical improvement Final regimen: Rifampin 450 mg/INH 200 mg/ethambutol 750 mg for 9 months (pyrazinamide excluded due to prior hepatic involvement) Outcome: No DRESS recurrence; AFB-negative at 6 months Teaching point: DRESS requires complete drug stoppage + steroids; desensitization enables re-treatment. Use RegiSCAR scoring for diagnosis.
Case 3: INH-Associated Gastroparesis (PMID: 39270087, Rev Med Chil, 2023) - First ever reported case
Case 4: Suicide Attempts with INH in Adolescents on TB Prophylaxis (PMID: 34229576, Paediatr Int Child Health, 2021)
Classic Published Case Types (from textbooks):
- Typical presentation: malaise, fatigue, anorexia, nausea/vomiting 4-8 weeks after starting INH
- 70% of fatal cases occur in women
- AST often exceeds ALT
- Continued INH after onset of symptoms = most preventable cause of fatal DILI
- Management: Stop INH immediately. Supportive care. LT if fulminant. Rechallenge may be attempted by gradual reintroduction after full resolution in selected patients.
- ANA-positive vasculitis appearing during treatment
- No specific management beyond stopping INH - resolves spontaneously
- Pyridoxine-deficient patient starting INH develops dramatic anemia
- Treatment: large doses of vitamin B6 gradually restore blood count to normal
15. META-ANALYSIS: OVERALL ADR INCIDENCE IN LTBI TREATMENT
- Any AE in adults: 3.7%
- Hepatotoxicity leading to drug discontinuation in adults: 1.1%
- Any AE in children: 0.4%
- Hepatotoxic AE in children: 0.02%
- Highest AE incidence: 3HP (INH + rifapentine 3 months) and 9H (9 months INH monotherapy)
- Lowest AE incidence: 4R (4 months rifampin alone)
- Conclusion: Pediatric populations are very safe on all LTBI regimens; in adults, rifamycin-based regimens are safer than INH monotherapy, with 4R having the lowest hepatotoxicity.
16. SUMMARY TABLE: KNOW-IT-ALL QUICK REFERENCE
| Feature | Key Fact |
|---|---|
| Drug class | Bactericidal antitubercular (isonicotinic acid hydrazide) |
| Prodrug activated by | KatG catalase-peroxidase (mycobacterial) |
| Primary target | InhA (enoyl-ACP reductase) + KasA → blocks mycolic acid synthesis |
| Secondary target | Dihydrofolate reductase → blocks nucleic acid synthesis |
| Spectrum | M. tuberculosis, M. kansasii (limited); no activity elsewhere |
| Bioavailability | ~100% oral |
| CSF penetration | Excellent (equals serum levels) |
| Metabolism | NAT2 (liver) → acetylisoniazid; toxic metabolites via CYP2E1 |
| Acetylator status determines | Half-life (1h rapid; 3-4h slow), side effect profile |
| Most serious ADR | Hepatotoxicity (2% incidence; 5-10% of cases fatal) |
| Classic toxic triad | Seizures + metabolic acidosis + coma |
| Overdose antidote | Pyridoxine IV, gram-for-gram; 5g adults, 70mg/kg children |
| Peripheral neuropathy prevention | Pyridoxine 25-50 mg/day |
| Key drug interaction | Phenytoin (CYP2C19 inhibition) - phenytoin toxicity |
| Contraindications | Acute liver disease; prior INH hepatitis |
| LTBI preferred regimen 2025 | 3HP (INH + rifapentine weekly x 3 months) |
| Active TB dose | 5 mg/kg/day (max 300 mg) in HRZE combo |
| Monitoring cutoff for stopping | ALT ≥5x ULN (asymptomatic), ≥3x ULN (symptomatic) |
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, pp. 1292-1293
- Harrison's Principles of Internal Medicine 22E (2025), pp. 1462-1466
- Lippincott Illustrated Reviews: Pharmacology, pp. 1055-1058
- Tintinalli's Emergency Medicine: A Comprehensive Study, pp. 1278-1299
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, pp. 1676-1677
- The Harriet Lane Handbook (Johns Hopkins), 23rd ed., pp. 3997-4042
- Symptom to Diagnosis: An Evidence Based Guide, 4th Ed., pp. 9030-9040
- Melnychuk et al. (2023). Systematic Review/Meta-analysis of TB preventive therapy AEs. Clin Infect Dis. PMID: 37125482
- Akçay et al. (2024). INH overdose hypersensitivity myocarditis. Cardiol Young. PMID: 39397742
- Manullang & Marhana (2026). DRESS syndrome in TB patient. Int J Mycobacteriol. PMID: 41894632
- Gálvez et al. (2023). Gastroparesis associated with isoniazid. Rev Med Chil. PMID: 39270087
make one each for rifampicin, pyrazinamide and etambutol in the similar way
rifampicin adverse effects hepatotoxicity drug interactions
ethambutol optic neuropathy case report treatment
pyrazinamide hepatotoxicity gout hyperuricemia case
rifampicin adverse reaction case report cutaneous thrombocytopenia
PMID: 35518548
PMID: 35756837
rifampin flu-like syndrome acute renal failure hemolytic anemia
pyrazinamide adverse effect case report
PMID: 36181061
PMID: 39034578
PMID: 35582729
RIFAMPICIN (RIFAMPIN) - Complete Reference Guide
1. OVERVIEW & CHEMISTRY
- Forms: Capsules 150, 300 mg; Oral suspension 10, 25 mg/mL; Injection 600 mg/vial (contains formaldehyde sulfoxylate); Fixed-dose combination Rifater (rifampin 120 mg + INH 50 mg + pyrazinamide 300 mg)
- Brand names: Rifadin and generics
2. MECHANISM OF ACTION
- The human RNA polymerase does NOT bind rifampin and is NOT inhibited - basis for selective toxicity
- Rifampin is bactericidal for mycobacteria - it kills organisms in all metabolic states
- It kills intracellular organisms, organisms in abscesses, and those in lung cavities - places most other drugs cannot reach effectively
- This explains its unique role as a "sterilizing" drug - it eradicates persistent, slowly metabolizing organisms that would cause relapse
3. ANTIMICROBIAL SPECTRUM
| Organism | Activity |
|---|---|
| M. tuberculosis | Excellent (MIC 0.06-0.25 mg/L) |
| M. leprae | Excellent (<1 µg/mL) |
| M. kansasii | Good (MIC 0.25-1 mg/L) |
| M. avium complex (MAC) | Moderate (MIC ~4 mg/L) |
| M. scrofulaceum, M. intracellulare | Moderate |
| M. abscessus | Innate resistance (ADP-ribosyltransferase + monooxygenase) |
| S. aureus, coagulase-negative staph | Active |
| N. meningitidis, H. influenzae | Active |
| Legionella spp. | Active |
| E. coli, Pseudomonas, Proteus, Klebsiella | Active in vitro (not primary indication) |
| Chlamydiae | Active |
4. MECHANISMS OF RESISTANCE
- Prevalence: ~1 in 10⁷-10⁸ bacilli
- 86% of cases: point mutations at codons 526 and 531 of rpoB gene → altered RNAP with reduced rifampin affinity
- Various other missense mutations in the core region of rpoB
- Efflux pump induction and mutations also contribute
- Cross-resistance: Complete cross-resistance among all rifamycins (rifampin, rifapentine, rifabutin)
- No cross-resistance to other antimicrobial drug classes
- Resistance develops rapidly with monotherapy - NEVER use alone in active disease
- Rifamycin monoresistance occurs at higher rates with intermittent dosing, especially in HIV-positive patients
5. PHARMACOKINETICS
5.1 Absorption
- Well absorbed orally
- Food decreases Cmax by one-third - best taken on an empty stomach (1 hour before or 2 hours after meals)
- Oral doses: give 1 hour before or 2 hours after meals; abstain from alcohol
- Can be given IV (same dose) when oral route not possible
5.2 Distribution
- Distributes widely to most body fluids and tissues
- Penetrates into phagocytes - kills intracellular organisms
- CSF penetration: Variable, 10-20% of blood concentrations at standard doses; only adequate in presence of meningeal inflammation (Katzung). Nonetheless recommended for TB meningitis.
- Protein binding: Relatively high (97% for rifapentine; rifampin highly protein-bound)
- Tears, urine, sweat, saliva, sputum, feces turn orange-red - harmless but warn patients; tears can permanently stain soft contact lenses
5.3 Metabolism & Excretion
- Metabolized by hepatic microsomal β-esterases and cholinesterases
- Autoinduction: Rifampin induces its own metabolism (CYP enzymes), causing increasing clearance with repeated dosing - half-life shortens over the first 1-2 weeks of therapy. This is concentration-dependent.
- Major metabolite: deacetylated rifampin (microbiologically active)
- Excreted primarily through bile into feces via enterohepatic recycling; small amount in urine
- Serum levels: 5-7 µg/mL at usual doses; Cmax 10-20 µg/mL 2.5 h after 10 mg/kg dose
5.4 Dose Adjustment
- No dose adjustment needed for renal or hepatic insufficiency (Katzung) - but use cautiously in liver disease
- Harriet Lane: reduce dose in hepatic impairment; adjust dose in renal failure per guidelines
- Elimination constant: 1.15/h
- Systemic clearance: 19 L/h
- Volume of distribution: 53 L
6. DOSING
6.1 Active Tuberculosis
| Population | Dose | Frequency |
|---|---|---|
| Adult | 10 mg/kg (max 600 mg) | Once daily |
| Adult | 10 mg/kg (max 600 mg) | Twice weekly (continuation phase) |
| Child/Infant (daily) | 10-20 mg/kg (max 600 mg) | Once or divided Q12-24h |
| Child (twice weekly) | 15-20 mg/kg (max 600 mg) | Twice weekly |
| CNS/Disseminated TB in infants/toddlers | 20-30 mg/kg (max 600 mg) | Divided Q12-24h |
| TB meningitis (all ages) - PO | 20 mg/kg (max 1200 mg) | Q24h |
| TB meningitis - IV | 15 mg/kg (max 900 mg) | Q24h |
6.2 Latent TB Infection (LTBI)
- 4R (Rifampin alone, 4 months): 600 mg/day in adults, 10-20 mg/kg in children. Currently preferred over 9H for HIV-negative individuals; lower AE incidence than INH-based regimens.
- 3HR (Rifampin + INH, 3 months): Daily rifampin + INH for 3 months. Note: higher hepatotoxicity than individual drugs.
- 3HP (Rifapentine + INH, weekly x 12 doses): 900 mg rifapentine + 900 mg INH weekly. Currently preferred LTBI regimen overall.
- CONTRAINDICATED for LTBI: Rifampin + pyrazinamide combination - risk of severe/fatal liver injury.
6.3 Other Indications - Dosing
| Indication | Dose |
|---|---|
| Meningococcal prophylaxis (adult) | 600 mg PO Q12h x 2 days |
| Meningococcal prophylaxis (≥1 mo) | 20 mg/kg/24h ÷ Q12h x 2 days |
| Meningococcal prophylaxis (<1 mo) | 10 mg/kg/24h ÷ Q12h x 2 days |
| H. influenzae type b prophylaxis | 20 mg/kg (max 600 mg) once daily x 4 days |
| Staphylococcal infections (synergistic) | 10-20 mg/kg/24h ÷ Q12h IV/PO (max 600 mg/24h) |
| Prosthetic valve endocarditis - early | 20 mg/kg/24h ÷ Q8h (max 900 mg/24h) |
| MRSA infection | 15 mg/kg/24h ÷ Q8h (max 900 mg/24h) |
| Leprosy | Part of multi-drug regimen (monthly supervised 600 mg) |
7. OTHER USES OF RIFAMPIN
- TB treatment (all forms - pulmonary, extrapulmonary, meningitis, miliary)
- LTBI treatment (4R alone, or 3HP/3HR combinations)
- Leprosy (multibacillary and paucibacillary regimens)
- Meningococcal prophylaxis (close contacts of N. meningitidis cases)
- H. influenzae type b prophylaxis (contacts of children with Hib meningitis)
- NTM infections: M. kansasii, M. avium, M. marinum, M. ulcerans, M. malmoense, M. haemophilum
- Prosthetic material infections: prosthetic joint infections, prosthetic valve endocarditis, vascular graft infections (combined with other antibiotics)
- Serious staphylococcal infections: osteomyelitis, endocarditis (synergistic combination therapy only)
- Brucellosis (combination therapy)
- Rifampin-soaked prosthetics in surgery to prevent biofilm formation
8. ADVERSE EFFECTS
8.1 Common / Minor
- Urine, sweat, tears, saliva, sputum turn orange-red - harmless; can permanently stain soft contact lenses. Always warn patients.
- GI: Nausea, vomiting, abdominal discomfort, diarrhea (common)
- Headache, fatigue, ataxia, muscle weakness
- Transient elevations in LFTs (common, often resolve)
- Light-chain proteinuria (common, usually benign)
8.2 Hepatotoxicity
- Isolated hyperbilirubinemia (competitive inhibition of bilirubin excretion) - common, usually benign
- Clinical hepatitis: Rare in absence of preexisting liver disease; more common as aminotransferase elevation than frank hepatitis
- When combined with INH and/or pyrazinamide: hepatotoxicity risk increases significantly
- Fatal hepatic failure: rare
- Risk increases in: alcoholics, elderly, patients with chronic liver disease, combined anti-TB regimens
- CONTRAINDICATED: Rifampin + pyrazinamide for LTBI (risk of severe/fatal liver injury - this combination was removed from LTBI guidelines)
- Pulmonary toxicity and vitamin K-dependent coagulation disorders: reported
8.3 The "Flu-Like" Hypersensitivity Syndrome (Intermittent Dosing)
- Occurs especially with high-dose intermittent therapy (less than twice weekly)
- Manifestations: fever, chills, myalgias, arthralgias
- Can progress to: hemolytic anemia, thrombocytopenia, acute renal failure (acute tubular necrosis, interstitial nephritis), shock
- Mechanism: immune-mediated (antibody formation against rifampin-protein adducts during intermittent exposure)
- Management: switch to daily dosing; discontinue rifampin if severe
8.4 Hematological ADRs
- Thrombocytopenia (immune-mediated, particularly with intermittent dosing)
- Hemolytic anemia (immune-mediated, intermittent dosing)
- Blood dyscrasias (general)
- Bleeding / coagulation disorders (vitamin K pathway disruption)
8.5 Renal ADRs
- Interstitial nephritis
- Acute tubular necrosis
- Elevated BUN and uric acid
- Associated with severe hypersensitivity reactions in intermittent dosing
8.6 Other ADRs
- Rash, pruritus - relatively common
- Confusion, mental status changes
- Porphyria: Use not recommended in porphyria
- Rifabutin-specific: Uveitis (anterior), pseudojaundice (skin orange discoloration), neutropenia, polymyalgia, skin hyperpigmentation
9. DRUG INTERACTIONS - THE MOST IMPORTANT ASPECT OF RIFAMPIN
| Drug Class | Drug | Consequence |
|---|---|---|
| Antiretrovirals | Protease inhibitors, NNRTIs, INSTIs | Dramatically reduced ARV levels - usually switch to rifabutin |
| Anticoagulants | Warfarin | Reduced anticoagulant effect → need higher doses; monitor INR closely |
| Anticonvulsants | Phenytoin, carbamazepine | Reduced anticonvulsant levels → seizure risk |
| Immunosuppressants | Cyclosporine, tacrolimus | Reduced levels → transplant rejection risk |
| Corticosteroids | Prednisolone, dexamethasone | Reduced steroid effect |
| Oral contraceptives | Estrogen/progesterone pills | Contraceptive failure - switch to non-hormonal method |
| Antifungals | Itraconazole, ketoconazole, voriconazole | Markedly reduced antifungal levels |
| Opioids | Methadone | Withdrawal symptoms (reduced methadone levels) |
| Cardiovascular | Digoxin, calcium channel blockers, β-blockers, quinidine | Reduced drug levels |
| Benzodiazepines | Diazepam and others | Reduced sedation |
| Others | Theophylline, buspirone, fentanyl, barbiturates | Reduced drug levels |
| Praziquantel | Praziquantel | Dramatically reduced praziquantel levels - contraindicated; stop rifampin 4 weeks before praziquantel, restart 1 day after completion |
10. MONITORING
| Baseline | Ongoing |
|---|---|
| Hepatic enzyme measurements (ALT, bilirubin) | Repeat if abnormal or patient is at risk or symptomatic |
| CBC | Monthly clinical monitoring for hepatotoxicity symptoms |
| Review all drug interactions | Visual checks of urine color for adherence |
11. CONTRAINDICATIONS
- Porphyria
- Severe hepatic impairment (relative)
- Hypersensitivity to rifamycins
- Combination with pyrazinamide for LTBI (absolute)
- Combination with praziquantel (relative - time-separate)
12. CASE REPORT: Rifampin-Associated Adverse Events
Classic Pattern: Intermittent Rifampin Flu-Like Syndrome with Hemolytic Anemia
- Patient on twice-weekly or less frequent rifampin develops fever, chills, myalgias 3-6 hours after each dose
- On workup: thrombocytopenia, hemolytic anemia with elevated LDH and unconjugated bilirubin
- Coombs test may be positive (immune hemolysis)
- Renal function deteriorates: rising creatinine (interstitial nephritis)
- Management: Discontinue rifampin immediately. Switch to rifabutin if TB treatment continuation necessary. Supportive care with IV fluids for renal protection. Rarely, dialysis may be needed.
- Teaching point: This syndrome is immune-mediated, antibody-driven, and is specifically linked to irregular/intermittent dosing. Daily dosing reduces the risk significantly.
13. QUICK REFERENCE TABLE
| Feature | Key Fact |
|---|---|
| Class | Rifamycin macrocyclic antibiotic |
| MOA | Binds β-subunit of bacterial RNAP (rpoB) → blocks RNA transcription |
| Unique role | STERILIZING agent - kills persistent organisms → enables 6-month short course |
| Spectrum | M. tuberculosis, M. leprae, M. kansasii, NTM, S. aureus, N. meningitidis, H. influenzae |
| Best taken | Empty stomach (food reduces Cmax by 1/3) |
| Distinctive | Turns body fluids orange-red (urine, tears, sweat) |
| Metabolism | CYP autoinduction → half-life shortens over 1-2 weeks; biliary excretion |
| Key ADR | Flu-like syndrome with hemolysis/thrombocytopenia/AKI (intermittent dosing) |
| Hepatotoxicity | Rare alone; risk increases with INH+PZA combo |
| Drug interactions | POTENT CYP inducer (1A2, 2C9, 2C19, 2D6, 3A4) - review all meds |
| Adult TB dose | 10 mg/kg/day (max 600 mg) |
| LTBI dose | 10 mg/kg/day (max 600 mg) x 4 months (4R) |
| Never | Monotherapy in active TB; rifampin + PZA for LTBI |
| Resistance | rpoB mutations; 86% at codons 526 and 531 |
PYRAZINAMIDE (PZA) - Complete Reference Guide
1. OVERVIEW & CHEMISTRY
- Forms: Tablets 500 mg; Oral suspension 100 mg/mL; Fixed combination Rifater (PZA 300 mg + rifampin 120 mg + INH 50 mg)
- Available as: Pyrazinoic acid amide and generics
2. MECHANISM OF ACTION
- PanD inhibition: POA binds competitively to the enzyme PanD (aspartate decarboxylase), which is essential for coenzyme A biosynthesis in M. tuberculosis. This triggers degradation of PanD by the protease ClpC1-ClpP.
- RpsA inhibition: An additional target is ribosomal protein S1 (RpsA), involved in the trans-translation process. Blocking RpsA leads to accumulation of toxic truncated proteins that kill bacteria.
- Active only at acidic pH (<6.0) - works specifically in acidic compartments: inside phagolysosomes and in necrotic/caseous lesions
- More active against slowly replicating organisms than rapidly replicating ones (opposite of INH)
- This pH-dependent activity is the basis for its unique clinical niche
- At pH 5.9, MIC of M. tuberculosis ranges 6.25-200 mg/L (wide variation)
3. ANTIBACTERIAL SPECTRUM
- Essentially limited to M. tuberculosis - very narrow spectrum
- Activity is minimal against M. bovis (intrinsically pyrazinamidase-deficient)
- Most NTM are resistant
- Active against bacilli inside macrophages and acidic granulomas where most other drugs cannot function
4. MECHANISMS OF RESISTANCE
| Mechanism | Details |
|---|---|
| pncA mutations (most common) | Mutations in multiple positions → reduced pyrazinamidase activity → drug not converted to active POA |
| RpsA mutations | Confer resistance directly |
| panD mutations | Reduce target affinity for POA |
| Efflux pump mutations | Cause cross-resistance with other TB drugs |
5. PHARMACOKINETICS
5.1 Absorption
- Oral bioavailability >90% - well absorbed, though absorption rate varies between patients (absorption constant 3.56/h vs 1.25/h in slow absorbers)
5.2 Distribution
- Distributes throughout the body
- Penetrates CSF - important for TB meningitis coverage
- Vd and clearance increase with patient mass (0.5 L/h and 4.3 L per 10 kg above 50 kg)
- Vd is larger in males (by 4.5 L)
5.3 Metabolism & Excretion
- Metabolized by microsomal deaminase → pyrazinoic acid (POA) → hydroxylated by xanthine oxidase → 5-hydroxy-POA → renally excreted
- POA inhibits renal tubular secretion of urate → hyperuricemia (nearly universal)
- Hemodialysis removes pyrazinamide - must redose after each session
- Clearance is reduced in renal failure → dosing frequency reduced to 3 times/week at low GFR
- PK is AUC-driven for both efficacy and toxicity
- Absorption constant: 3.56/h
- Systemic clearance: 3.4 L/h
- Volume of distribution: 29.2 L
6. DOSING
6.1 Active Tuberculosis (First 2 months of HRZE)
| Population | Weight | Daily Dose | Twice-Weekly |
|---|---|---|---|
| Adult | 40-55 kg | 1000 mg PO once daily | 2000 mg x2/week |
| Adult | 56-75 kg | 1500 mg PO once daily | 3000 mg x2/week |
| Adult | 76-90 kg | 2000 mg PO once daily | 4000 mg x2/week |
| Child (<40 kg) | <40 kg | 30-40 mg/kg/24h once daily (max 2 g) | 50 mg/kg/dose x2/week (max 2 g/dose) |
6.2 Dose in Renal Failure
- GFR <30 mL/min: give 3x/week instead of daily
- Hemodialysis patients: re-dose after each session
6.3 NOT Recommended
- PZA + rifampin for LTBI - removed from guidelines due to unacceptably high risk of severe/fatal liver injury
7. OTHER USES
8. ADVERSE EFFECTS
8.1 Hepatotoxicity - Most Serious ADR
- Most common dose-related adverse effect
- Appears to be idiosyncratic up to ~40 mg/kg; above that, a clear exposure-toxicity relationship emerges
- At high doses (historical): hepatic disease in ~15%, jaundice in 2-3%, deaths from hepatic necrosis (rare)
- At current dosing regimens: much safer, but still the most hepatotoxic of first-line TB drugs weight-for-weight
- Baseline hepatic function tests required before starting PZA; repeat during treatment
- Contraindicated in severe hepatic damage and in porphyria
- If PZA cannot be used due to liver disease: use rifampin + INH + ethambutol for 9 months instead of 6
- Stop PZA (and all hepatotoxic drugs)
- Wait for complete enzyme normalization (may take weeks to months - see case report below)
- Alternative regimen: ethambutol + fluoroquinolone (e.g., levofloxacin) for extended duration
8.2 Hyperuricemia (Near-Universal)
- Occurs in nearly all patients - POA inhibits renal tubular secretion of urate
- Usually asymptomatic
- Acute gout attacks can occur - particularly in patients with pre-existing gout or high uric acid
- Contraindicated in acute gout (Harriet Lane)
- Monitor baseline and periodic serum uric acid
- If symptomatic hyperuricemia: consider allopurinol; if gout attack occurs, may need to hold PZA
8.3 GI Toxicity
- Anorexia, nausea, vomiting (common)
- Dysuria
- Malaise
8.4 Arthralgia / Joint Pain
- Non-gouty arthralgia (separate from hyperuricemic gout)
- Common, generally manageable with NSAIDs
- Joint aches are among the most frequently reported patient complaints
8.5 Cutaneous ADRs
- Rash (various morphologies)
- Photosensitivity - patients should use sun protection
- Rare: Toxic Epidermal Necrolysis (TEN) - life-threatening (see case report)
- Drug-induced lichenoid eruptions (reported with anti-TB regimens)
8.6 Other
- Fever (drug fever)
- Diabetes management: Use with caution in diabetes mellitus (Harriet Lane)
- Sideroblastic anemia (reported rarely)
9. DRUG INTERACTIONS
| Interaction | Notes |
|---|---|
| Combined with rifampin (active TB) | Acceptable but increases overall hepatotoxicity risk |
| Combined with rifampin (LTBI) | CONTRAINDICATED - severe/fatal hepatotoxicity |
| Combined with rifampin + INH | All three are hepatotoxic; monitor closely |
| Combined with allopurinol | May be used if PZA-induced hyperuricemia is symptomatic |
| Renal failure | PZA accumulates; adjust dosing frequency |
10. MONITORING
| Baseline | Ongoing |
|---|---|
| LFTs (ALT, AST, bilirubin) - mandatory | Monthly LFTs during treatment |
| Serum uric acid | Periodic uric acid monitoring |
| Assess for gout, liver disease, diabetes | Monthly clinical monitoring for GI/joint/skin symptoms |
- ALT >5x ULN asymptomatic, or >3x ULN with hepatitis symptoms
- Any signs of acute gout
- Severe rash or blistering skin reactions
11. CONTRAINDICATIONS
- Severe hepatic damage
- Acute gout (Harriet Lane)
- Combination with rifampin for LTBI (absolute)
- Pregnancy: WHO allows PZA in pregnancy; US does NOT approve due to inadequate teratogenicity data. CDC/ATS recommend avoiding for routine LTBI in pregnancy.
12. CASE REPORTS OF NOTABLE ADRs AND THEIR MANAGEMENT
Case 1: Pyrazinamide-Related Prolonged Drug-Induced Liver Injury (PMID: 36181061, Medicine, 2022)
- PZA-related DILI can be prolonged and delayed - recovery may take months, not weeks
- NAT2 slow acetylator phenotype may increase PZA DILI risk (mechanism unclear - not the same pathway as INH)
- If PZA must be discontinued, effective TB cure is still achievable with alternative extended regimens
Case 2: Pyrazinamide-Induced Toxic Epidermal Necrolysis (PMID: 39034578, Ann Afr Med, 2024)
- Immediate discontinuation of PZA (and all suspect drugs)
- Supportive care in ICU/burn unit setting
- Wound care, fluid management, ophthalmologic care
- Consideration of IVIG or cyclosporin for TEN management Teaching point: Any anti-TB drug can potentially cause TEN. Rapid discontinuation is mandatory and life-saving. Always assess all drugs and rechallenge only under specialist supervision.
Case 3: Tuberculosis Treatment-Related Lichenoid Drug Eruptions (PMID: 36510939, Int J Mycobacteriol, 2022)
13. QUICK REFERENCE TABLE
| Feature | Key Fact |
|---|---|
| Class | Synthetic pyrazine analogue of nicotinamide; prodrug |
| MOA | Activated by pncA to POA → inhibits PanD (CoA synthesis) + RpsA (trans-translation) |
| Unique feature | Active ONLY at acidic pH (<6.0) - kills intracellular/caseous bacilli |
| Clinical role | Enables 6-month short-course therapy (vs 9-12 months without) |
| Spectrum | M. tuberculosis only |
| Duration in regimen | First 2 months only |
| Adult dose | Weight-banded: 1000-2000 mg/day (40-90 kg) |
| Most common ADR | Hyperuricemia (near-universal) |
| Most serious ADR | Hepatotoxicity (idiosyncratic; dose-related at high doses) |
| Liver monitoring | Mandatory at baseline and throughout |
| Gout | Contraindicated in acute gout |
| Key drug interaction | Rifampin + PZA for LTBI = CONTRAINDICATED (fatal hepatitis) |
| Renal failure | Reduce frequency to 3x/week; re-dose after dialysis |
| Pregnancy | WHO allows; US does NOT (inadequate data) |
ETHAMBUTOL (EMB) - Complete Reference Guide
1. OVERVIEW & CHEMISTRY
- Forms: Tablets 100 mg, 400 mg (may be scored); Oral suspension 50, 100 mg/mL
- Brand names: Myambutol and generics
- Note: Only the D-isomer is active; the L-isomer is less active and more toxic
2. MECHANISM OF ACTION
- Bacteriostatic - slows mycobacterial growth, does not kill
- Specific for mycobacteria; no activity against other bacteria or fungi
- Active against both intracellular and extracellular organisms
- Microbial kill of M. tuberculosis is optimized by AUC/MIC ratio; MAC kill optimized by Cmax/MIC
3. ANTIMICROBIAL SPECTRUM
| Organism | MIC | Activity |
|---|---|---|
| M. tuberculosis | 0.5-2 mg/L | Good |
| M. kansasii | ~0.8 mg/L | Good |
| M. avium complex (MAC) | 2-7.5 mg/L | Moderate |
| M. gordonae, M. marinum, M. scrofulaceum, M. szulgai | Variable | Susceptible |
| M. xenopi, M. fortuitum, M. abscessus, M. chelonae | High | Mostly resistant |
| All other bacteria | - | No activity |
4. MECHANISMS OF RESISTANCE
| Mechanism | Details |
|---|---|
| embB mutations (most common, 30-70% of clinical isolates) | Mutations in the ethambutol resistance-determining region of embB gene, particularly codon 306 |
| Codon 306 caveat | Also found in ethambutol-susceptible strains - necessary but NOT sufficient for resistance |
| Efflux pump overexpression | Can confer resistance to both EMB and INH in vitro |
| emb gene overexpression | Increased arabinosyl transferase levels overwhelm drug concentration |
5. PHARMACOKINETICS
5.1 Absorption
- Oral bioavailability ~80%
- After 25 mg/kg ingestion: blood level peak of 2-5 µg/mL at 2-4 hours
- Slow and incomplete absorption is common in children (Goodman & Gilman's)
- Give with food (Harriet Lane)
- Aluminum hydroxide decreases absorption - space administration by 4 hours
5.2 Distribution
- Two-compartment model with first-order absorption and elimination
- Biexponential decline: t½ of 3 hours in first 12 hours, t½ of 9 hours between 12-24 hours (redistribution)
- Clearance and Vd are greater in children than adults on a per-kilogram basis
- Blood-brain barrier: Crosses only when meninges are inflamed; CSF concentrations highly variable (4-64% of serum levels with meningeal inflammation). Penetration is questionably adequate for TB meningitis.
- Protein binding: 10-40%
- Absorption constant: 0.7/h
- Systemic clearance: 1.3 L/h/kg
- Vd: 6.0 L/kg
5.3 Metabolism & Excretion
- 80% excreted unchanged in urine (renally cleared - major route)
- ~20% oxidized by aldehyde dehydrogenase → aldehyde and dicarboxylic acid derivatives (excreted in urine)
- 20% excreted in feces unchanged
5.4 Dose Adjustment in Renal Failure
- Ethambutol accumulates in renal failure - one of the most important clinical points
- GFR <30 mL/min: dose at 15-25 mg/kg 3 times a week instead of daily (Goodman & Gilman's)
- Hemodialysis patients: dose 3x/week
- Renal dysfunction increases risk of ocular toxicity - heightened vigilance needed
6. DOSING
6.1 Active Tuberculosis
| Population | Dose | Frequency |
|---|---|---|
| Adult (daily) | 15-25 mg/kg | Once daily |
| Adult (3x weekly DOT) | 25-30 mg/kg | Three times weekly |
| Adult (twice weekly DOT) | 50 mg/kg | Twice weekly |
| TB meningitis (higher dose used) | Up to 25 mg/kg | Once daily |
- 40-55 kg: 800 mg once daily or 5x/week
- 56-75 kg: 1200 mg once daily or 5x/week
- 76-90 kg: 1600 mg once daily or 5x/week
- 15-25 mg/kg/dose (max 1 g/24h) PO once daily, OR
- 50 mg/kg/dose PO twice weekly (max 2.5 g/week)
6.2 Nontuberculous Mycobacterial (NTM) Infections
- M. avium complex (MAC) in AIDS: 15-25 mg/kg/24h PO once daily (max 2.5 g/24h)
- M. kansasii: 15 mg/kg once daily
- Always in combination with at least 2 other active drugs (typically rifampin + macrolide for MAC)
7. OTHER USES
- Active TB (first-line, first 2 months of HRZE - dropped if isolate susceptible to H, R, Z)
- Disseminated M. avium complex (MAC) in AIDS (combination with clarithromycin/azithromycin + rifabutin)
- M. kansasii infection (combination therapy)
- Other susceptible NTM infections (M. gordonae, M. marinum, M. scrofulaceum, M. szulgai)
- Drug-resistant TB (higher doses used - up to 25 mg/kg) when susceptibility allows
- Resistance prevention - its primary role is to prevent emergence of resistance to companion drugs while susceptibility data are pending
8. ADVERSE EFFECTS
8.1 Optic Neuritis (Ethambutol Optic Neuropathy - EON) - The Defining ADR
| Daily Dose | Incidence of Optic Neuritis |
|---|---|
| 50 mg/kg/day | ~15% |
| 25 mg/kg/day | ~5% |
| 15 mg/kg/day | <1% |
- 15 mg/kg/day is the recommended dose for drug-susceptible TB due to this narrow therapeutic window
- Higher doses (25 mg/kg) are reserved for drug-resistant TB where higher efficacy is needed despite increased toxicity risk
- Usually bilateral, but may be unilateral
- Painless - no eye pain
- Decreased visual acuity
- Red-green dyschromatopsia (loss of red-green color discrimination) - most common early finding
- Blue-yellow color defects may be an even earlier, subtle finding (not detected on Ishihara testing)
- Loss of contrast sensitivity (early sign)
- Central, paracentral, or peripheral visual field defects
- Normal or slightly swollen optic discs with splinter hemorrhages
- Normal or sluggish pupils (late)
- Typically occurs 3-6 months after starting treatment
- Can occur after only a few days (rare)
- Can occur after 3 years (see case report - Peterson & Hawy) - delayed onset is possible
- Recovery: usually occurs when ethambutol is withdrawn, but can be permanent - optic atrophy develops in a minority
- Higher doses (>15 mg/kg/day)
- Renal dysfunction (reduced excretion → drug accumulation)
- Duration of therapy
- Pre-existing optic nerve disease
- Concurrent INH use (additive risk - INH rarely causes optic neuropathy alone, but risk increases with combination)
- Baseline: visual acuity (Snellen chart) + color vision (Ishihara plates) - mandatory before starting
- Repeat: monthly if on higher doses; every 6 months at standard 15 mg/kg dose (Kanski's)
- Inform patient to report any visual changes immediately
- OCT (optical coherence tomography) can detect early RNFL thinning before symptomatic loss
- Stop ethambutol immediately when any visual deterioration is detected
- Also consider stopping INH if used concurrently
- Monitor visual recovery closely - improvement continues over months after cessation
- Some cases: OCT shows progression of optic nerve fiber loss even after clinical improvement
- Ethambutol is relatively contraindicated in young children who cannot reliably report visual changes or participate in testing
- Tintinalli's: not recommended when visual acuity cannot be assessed
- Use with extreme caution in patients with pre-existing optic nerve disease
8.2 Peripheral Neuropathy
- Less common than optic neuropathy but documented
- Sensory more than motor
- Usually at higher doses (see case report)
- Reversible on discontinuation
8.3 Hyperuricemia
- Occurs in ~50% of patients (Goodman & Gilman's)
- Due to decreased renal excretion of uric acid
- Less severe than with pyrazinamide
- Rarely causes symptomatic gout at standard doses
- Monitor uric acid
8.4 Hypersensitivity
- Hypersensitivity reactions are rare with ethambutol
- Rash (0.5%)
- Drug fever (0.3%)
- Erythema multiforme (reported, Harriet Lane)
8.5 Other ADRs
- GI: nausea, vomiting, abdominal pain, diarrhea
- Headache, dizziness, mental confusion, disorientation
- Possible hallucinations
- Pruritus
- Joint pain
- Hepatotoxicity: rare but reported (Harriet Lane)
- Mania (Harriet Lane)
9. DRUG INTERACTIONS
| Interaction | Notes |
|---|---|
| Aluminum hydroxide antacids | Reduce ethambutol absorption - space by 4 hours |
| INH (concurrent use) | Additive risk of optic neuropathy |
| Renal failure / nephrotoxic drugs | Accumulation of ethambutol → increased ocular toxicity |
10. MONITORING
| Baseline | Ongoing |
|---|---|
| Visual acuity (Snellen) - mandatory | Monthly if on >15 mg/kg; every 6 months at standard dose |
| Color vision (Ishihara plates) - mandatory | Repeat immediately if any visual complaint |
| Serum uric acid | Periodic uric acid |
| Liver function tests | Periodic LFTs |
| Renal function (creatinine/GFR) | Periodic - guides dose adjustment |
| Hematologic status | Periodic CBC |
11. CONTRAINDICATIONS
- Pre-existing optic neuritis
- Children too young for reliable visual acuity and color vision testing (relative)
- Severe renal failure without appropriate dose reduction
12. CASE REPORTS OF NOTABLE ADRs AND THEIR MANAGEMENT
Case 1: Delayed and Reversible Ethambutol Optic Neuropathy After 3 Years (PMID: 35756837, Am J Ophthalmol Case Rep, 2022)
- EON can be significantly delayed - even 3 years into treatment
- Toxicity can occur even at doses <15 mg/kg/day - no dose is absolutely safe
- Improvement can continue over months after stopping the drug
- Any patient on ethambutol who presents with vision changes consistent with optic neuropathy should be treated as EON until proven otherwise - high index of suspicion at all times
Case 2: Ethambutol-Induced Optic Neuropathy with Irreversible Outcome (PMID: 35582729, Biomed Pap Med Fac Univ Palacky, 2023)
- Clinical visual improvement ≠ structural recovery
- OCT is essential for monitoring - it can detect ongoing neurodegeneration even when subjective vision appears to be improving
- Once optic atrophy sets in, damage is permanent and irreversible
- This is why early detection and immediate cessation are so critical
Case 3: Ethambutol Causes Peripheral Neuropathy - A Rare Adverse Effect (PMID: 35518548, Cureus, 2022)
- Ethambutol can cause peripheral neuropathy - not just optic neuropathy
- This is more likely at higher doses (NTM infections often use higher doses than TB)
- High index of suspicion for EMB neuropathy in patients presenting with limb symptoms on ethambutol
- Discontinuation leads to regression of neuropathy
13. QUICK REFERENCE TABLE
| Feature | Key Fact |
|---|---|
| Class | Synthetic arabinogalactan synthesis inhibitor |
| MOA | Inhibits arabinosyl transferase III (embCAB) → blocks arabinogalactan synthesis → disrupts cell wall |
| Bacteriostatic vs. cidal | Bacteriostatic (unique among first-line drugs) |
| Primary role | Resistance prevention - protects companion drugs while awaiting susceptibility results |
| Spectrum | M. tuberculosis, M. kansasii, MAC, some other NTM |
| Bioavailability | ~80% oral |
| CSF penetration | Variable; adequate only with meningeal inflammation (4-64%) |
| Excretion | 80% unchanged in urine - dose adjust in renal failure |
| Defining ADR | Optic neuritis (EON) - dose- and duration-dependent |
| EON incidence at 15 mg/kg | <1% |
| EON monitoring | Baseline + monthly (higher dose); every 6 months (15 mg/kg) |
| Action at visual symptoms | Stop immediately |
| EMB contraindicated when | Can't assess visual acuity (young children); pre-existing optic neuritis |
| Drug interactions | Aluminum antacids decrease absorption (space by 4h); no CYP interactions |
| Renal failure | Accumulates → increase dosing interval to 3x/week if GFR <30 |
| Standard adult TB dose | 15-25 mg/kg/day (max 1600 mg) |
| Duration in TB regimen | First 2 months (stopped if isolate is susceptible to H, R, Z) |
Comparative Summary Table: All Four First-Line TB Drugs (HRZE)
| Feature | Isoniazid (H) | Rifampin (R) | Pyrazinamide (Z) | Ethambutol (E) |
|---|---|---|---|---|
| Cidal/Static | Bactericidal | Bactericidal | Cidal (acidic) | Bacteriostatic |
| MOA | Inhibits mycolic acid (InhA) | Inhibits RNAP (rpoB) | Inhibits PanD, RpsA | Inhibits arabinosyl transferase (embB) |
| Prodrug? | Yes (KatG) | No | Yes (pncA) | No |
| Defining toxicity | Hepatitis + peripheral neuropathy | Flu-like syndrome + CYP interactions | Hepatotoxicity + hyperuricemia | Optic neuritis |
| Antidote available? | Yes - pyridoxine (B6) | No | No | No (stop drug) |
| CYP interactions? | Yes (inhibits 2C19, 3A) | Yes - major inducer | No | No |
| CSF penetration | Excellent (= serum) | Variable (10-20%) | Good | Poor-Variable (4-64%, inflamed) |
| Renal failure | Adjust dose | No adjustment | 3x/week | 3x/week |
| Monitoring | LFTs + neuropathy | LFTs + drug interactions | LFTs + uric acid | Visual acuity + color vision |
| Duration in 6-month regimen | All 6 months | All 6 months | First 2 months | First 2 months (if susceptible) |
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, pp. 2713-2934
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 186
- Lippincott Illustrated Reviews: Pharmacology, pp. 1055-1068
- Katzung's Basic and Clinical Pharmacology 16th Ed., pp. 1315-1330
- The Harriet Lane Handbook 23rd Ed. (Johns Hopkins)
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed., pp. 919-922
- Wang et al. (2022). PZA prolonged DILI. Medicine. PMID: 36181061
- Datta et al. (2024). Pyrazinamide-induced TEN. Ann Afr Med. PMID: 39034578
- Peterson & Hawy (2022). Delayed ETB optic neuropathy. Am J Ophthalmol Case Rep. PMID: 35756837
- Kyncl et al. (2023). ETB-induced optic neuropathy (irreversible). Biomed Pap. PMID: 35582729
- Rana et al. (2022). Ethambutol peripheral neuropathy. Cureus. PMID: 35518548
- Melnychuk et al. (2023). Meta-analysis of TPT adverse events. Clin Infect Dis. PMID: 37125482
if i have a pateint who consumed 100 fdc of ATT on a suicidal basis, how would i treat him
isoniazid massive overdose fixed dose combination tuberculosis suicide treatment
isoniazid overdose suicide case report management outcome
isoniazid poisoning pyridoxine treatment outcome
Emergency Management: 100 FDC ATT Overdose (Suicidal Ingestion)
STEP 0 - CALCULATE THE DOSE INGESTED FIRST
| Drug | Per Tablet | x 100 tablets | Toxic threshold |
|---|---|---|---|
| Isoniazid (H) | 75 mg | 7,500 mg (7.5 g) | Seizures >20-30 mg/kg; mortality risk >30 mg/kg |
| Rifampin (R) | 150 mg | 15,000 mg (15 g) | Less acutely lethal |
| Pyrazinamide (Z) | 400 mg | 40,000 mg (40 g) | Hepatotoxic |
| Ethambutol (E) | 275 mg | 27,500 mg (27.5 g) | Ocular toxicity |
- INH ingested: 7500 mg = 125 mg/kg (normal dose = 5 mg/kg; lethal territory begins at 30 mg/kg)
- Mortality risk without treatment: up to 20%
THE CLINICAL PICTURE TO EXPECT
- 30 min - 2 hours: Nausea, vomiting, slurred speech, ataxia, dizziness, mental status changes
- By 1-3 hours: Generalized tonic-clonic seizures - these will be REFRACTORY to standard anticonvulsants. This is your red flag.
- Concurrent/progressive: Anion gap metabolic acidosis (lactic acidosis from prolonged seizure activity), coma
- Body fluids: Orange-red discoloration of urine, vomit, secretions (from rifampin)
- Seizures refractory to benzodiazepines and barbiturates
- Anion gap metabolic acidosis refractory to sodium bicarbonate
- Protracted coma
MANAGEMENT - SYSTEMATIC APPROACH
PHASE 1: IMMEDIATE RESUSCITATION (0-10 minutes)
- Assess consciousness (GCS)
- If seizing or GCS ≤8: prepare for rapid sequence intubation (RSI)
- Position: lateral decubitus to prevent aspiration
- Have suction ready - vomiting is expected
- High-flow O₂ via non-rebreather mask
- Pulse oximetry, SpO₂ target >95%
- If intubated: ventilate with target normal PaCO₂ (do not hyperventilate unless raised ICP suspected)
- Large-bore IV access x2 (or central line)
- 12-lead ECG
- Continuous cardiac monitoring
- BP, HR, RR monitoring every 5 minutes
- IV fluid resuscitation if hypotensive (normal saline 500 mL bolus, repeat as needed)
- GCS assessment
- Blood glucose - check and correct hypoglycemia immediately (can mimic seizures)
- Pupils
PHASE 2: DECONTAMINATION (Do as early as possible if patient is awake)
- Indication: Presentation within 1-2 hours of ingestion AND patient is awake/cooperative with protected airway
- Dose: 1 g/kg body weight orally (standard adult dose: 50-100 g)
- NOT given if: unconscious, seizing, absent gag reflex (aspiration risk)
- If intubated: can give via NG tube after tube placement confirmed
- FDC tablets will still be in stomach if patient presents early - AC can bind multiple drugs
- Consider if very early presentation (<1 hour) AND airway secured
- Less commonly done now; activated charcoal is preferred
- Not effective for drugs already absorbed
PHASE 3: THE ANTIDOTE - PYRIDOXINE (VITAMIN B6)
| Scenario | Dose |
|---|---|
| INH dose known (7500 mg ingested here) | 7500 mg (7.5 g) IV pyridoxine |
| Unknown INH dose (adult) | 5 g IV pyridoxine |
| Unknown INH dose (child) | 70 mg/kg IV (max 5 g) |
- Give 1 g IV every 2-3 minutes until seizures stop OR the full dose is given
- This means for 7.5 g: administered over approximately 15-22 minutes
- Give the remaining pyridoxine dose over 4-6 hours via slow IV infusion to prevent recurrent seizures
- The dose may be repeated
- Crush and administer via NG tube - this is acceptable
PHASE 4: SEIZURE MANAGEMENT
| Drug | Dose | Route | Notes |
|---|---|---|---|
| Diazepam | 0.1-0.2 mg/kg IV (adult: 5-10 mg) | IV | First-line BZD; repeat every 5 min as needed |
| Lorazepam | 0.05-0.1 mg/kg IV (adult: 2-4 mg) | IV | Alternative first-line |
| Midazolam | 0.1-0.2 mg/kg IM | IM | If no IV access |
| Pyridoxine | 7.5 g IV (in this case) | IV | Administer simultaneously |
- Phenytoin / fosphenytoin - NO ROLE in INH seizures (GABA-dependent mechanism fails when GABA itself cannot be synthesized)
- Barbiturates alone - insufficient without pyridoxine
- Propofol infusion for refractory status epilepticus
- Intubation and general anesthesia (barbiturate coma) as last resort
- Continuous EEG monitoring to detect non-convulsive status epilepticus post-intubation
PHASE 5: LABORATORY & INVESTIGATIONS
| Test | Why |
|---|---|
| Blood glucose | Rule out hypoglycemia mimicking overdose |
| Arterial blood gas (ABG) | Anion gap metabolic acidosis severity, lactic acid |
| Serum electrolytes + AG calculation | AG = Na - (Cl + HCO₃); expect elevated AG |
| Serum lactate | Expect elevated |
| Serum creatinine + BUN | Renal function (ethambutol accumulates in renal failure) |
| LFTs (ALT, AST, bilirubin, ALP) | Baseline for INH and PZA hepatotoxicity; expect acute elevation |
| PT/INR | Coagulation (rifampin affects Vit K factors) |
| CBC | Baseline; hemolytic anemia risk |
| Uric acid | PZA ingested - will be acutely elevated |
| Serum ammonia | If encephalopathy |
| Urine toxicology | Confirm and rule out co-ingestion |
| ECG | Arrhythmia, QTc prolongation |
| Serum INH level | If available - confirms dose, guides repeat pyridoxine |
- Repeat LFTs (PZA hepatotoxicity evolves)
- Repeat ABG
- Ophthalmology review within 24h (ethambutol toxicity - document baseline vision)
- Liver ultrasound if LFTs markedly elevated
PHASE 6: MANAGING THE METABOLIC ACIDOSIS
- Expected: Anion gap metabolic acidosis, primarily lactic acidosis from seizure-induced muscle activity
- Sodium bicarbonate: NO ROLE - will not correct INH-induced acidosis
- Correct the cause: Stop seizures with pyridoxine → lactate will be cleared naturally
- Supportive: Adequate IV fluid hydration helps renal clearance
- Note: Lactic acidemia in INH toxicity resolves more slowly than in typical epileptic seizures - do not panic if pH normalizes slowly
PHASE 7: ENHANCED ELIMINATION
- INH is dialyzable (low molecular weight, low protein binding ~10%)
- Consider HD in:
- Massive overdose (like this case - 7500 mg)
- Refractory seizures or coma despite adequate pyridoxine
- Severe metabolic acidosis
- Renal failure (prevents excretion of INH + ethambutol)
- Published case: HD successfully cleared INH and was used alongside pyridoxine in massive overdose
- PZA is also removed by hemodialysis
PHASE 8: ORGAN-SPECIFIC MONITORING (Ongoing)
Liver (INH + PZA hepatotoxicity)
- Acute hepatocellular injury expected from both drugs
- Monitor LFTs: ALT, AST, bilirubin, PT/INR every 12-24 hours initially
- PZA DILI can be prolonged - may last weeks to months (as per Wang et al. case)
- If acute liver failure develops:
- N-acetylcysteine (NAC) - consider (used in acute liver failure broadly)
- Hepatology consultation
- Liver transplant evaluation if fulminant failure
Eyes (Ethambutol - 27.5 g ingested)
- Baseline visual acuity + color vision assessment ASAP (once patient is cooperative)
- Ophthalmology review within 24 hours
- Acute massive ethambutol exposure may cause rapid onset toxic optic neuropathy
- Monitor closely over days-weeks
Kidneys
- Ethambutol is 80% renally excreted - accumulates in renal failure
- Rifampin can cause interstitial nephritis / acute tubular necrosis
- Monitor urine output, creatinine, BUN
- Maintain adequate hydration
Uric Acid / Gout
- PZA (40 g ingested) causes massive hyperuricemia
- Monitor serum uric acid
- If acute gout attack: colchicine, NSAIDs, or corticosteroids
- Ensure good hydration and urine output
Coagulation
- Rifampin at toxic doses can impair Vitamin K-dependent clotting factors
- Monitor PT/INR
- If bleeding: Vitamin K IV + fresh frozen plasma (FFP) if severe
PHASE 9: ICU ADMISSION & PSYCHIATRIC EVALUATION
- Potential for refractory status epilepticus
- Risk of coma requiring ventilatory support
- Multi-organ toxicity monitoring
- Need for possible hemodialysis
- Once medically stable: mandatory psychiatric assessment
- Suicide risk stratification
- Safeguarding: remove access to ATT medications
- Decide on inpatient psychiatric admission vs. supervised outpatient follow-up
- Notify social worker and family
- Document the psychiatric evaluation in notes
PHASE 10: DISCHARGE / SAFE CLEARANCE CRITERIA
- Observe for a minimum of 6 hours from time of ingestion (Tintinalli's)
- If still asymptomatic at 6 hours: low risk for severe toxicity - may be medically cleared
- Admit to ICU regardless - this is a massive ingestion
- Discharge only after:
- LFTs stabilizing
- No recurrence of seizures for 24+ hours off acute management
- Renal function stable
- Psychiatric assessment completed and safety plan in place
COMPLETE MANAGEMENT FLOWCHART
PATIENT ARRIVES - 100 FDC ATT INGESTED
│
▼
CALCULATE DOSE: INH 7500mg (125 mg/kg in 60kg adult)
│
▼
ABCD RESUSCITATION + 2 large IV lines + monitors
│
├─► SEIZING? ──YES──► Benzodiazepines IV + PYRIDOXINE 7.5g IV simultaneously
│ (1g every 2-3 min; then remainder over 4-6h)
│ DO NOT GIVE PHENYTOIN
│
├─► AWAKE + <1-2h? ──► ACTIVATED CHARCOAL 1g/kg PO
│
├─► GCS ≤8 ──────────► RSI + intubate + ventilate
│
▼
URGENT BLOODS: ABG, Lactate, LFTs, RFTs, Glucose, Uric acid, PT/INR, CBC
│
▼
PYRIDOXINE 7.5g IV (if not already given) ─── even in comatose patient
│
▼
METABOLIC ACIDOSIS ──► Correct seizures (stops lactic acidosis)
(DO NOT give NaHCO₃) Maintain hydration
│
▼
REFRACTORY SEIZURES / SEVERE TOXICITY ──► Consider HEMODIALYSIS
│
▼
ICU ADMISSION
Monitor: LFTs q12h, RFTs, uric acid, coagulation, vision
│
▼
EYES: Ophthalmology review within 24h (ethambutol 27.5g)
LIVER: Consider NAC if ALT >10x ULN; hepatology consult
KIDNEYS: Maintain hydration; monitor for interstitial nephritis
│
▼
MEDICALLY STABLE ──► MANDATORY PSYCHIATRIC EVALUATION
Suicide risk assessment
Safe medication dispensing (blister packs, supervised)
SUMMARY: WHAT KILLS THIS PATIENT (and how to stop it)
| Threat | Drug | Timing | Intervention |
|---|---|---|---|
| Refractory seizures → anoxic brain injury / death | INH (7.5g) | 30min-2h | IV Pyridoxine 7.5g + BZDs - STAT |
| Lactic acidosis → cardiovascular collapse | INH | Hours | Control seizures; no bicarb |
| Coma | INH | Hours | Pyridoxine reverses |
| Acute liver failure | INH + PZA | Days-weeks | Monitor LFTs; hepatology |
| Optic neuropathy / blindness | ETB (27.5g) | Days | Ophthalmology; document baseline |
| Hyperuricemia / gout crisis | PZA (40g) | Days | Hydration; uric acid monitoring |
| Interstitial nephritis / ATN | Rifampin | Days | Hydration; renal monitoring |
| Thrombocytopenia / hemolysis | Rifampin | Days | CBC monitoring |
Pyridoxine 7.5 g IV is the antidote. Give it immediately upon presentation - before you even fully stabilize the airway if seizures are active. This is the single intervention that saves this patient's life.
drugs in BPalM regimen - in a similar way and also include thier toxicity and treatment
BPaLM regimen bedaquiline pretomanid linezolid moxifloxacin MDR-TB
bedaquiline pretomanid linezolid TB-PRACTECAL ZeNix trial
bedaquiline pretomanid linezolid MDR-TB efficacy adverse effects
BPaL BPaLM moxifloxacin MDR-TB trial outcome
linezolid peripheral neuropathy optic neuropathy tuberculosis case report treatment
PMID: 35812114
bedaquiline QT prolongation cardiac adverse effect case report
PMID: 36579197
TB-PRACTECAL trial BPaL moxifloxacin MDR-TB 6 months
BPaLM regimen WHO 2022 MDR-TB treatment outcomes
moxifloxacin adverse effect tendon QT toxicity case report
PMID: 39964841
PMID: 38455633
BPaLM REGIMEN - Complete Expert Reference
What is BPaLM?
- Multidrug-resistant TB (MDR-TB) - rifampin + INH resistant
- Pre-extensively drug-resistant TB (pre-XDR-TB)
DRUG 1: BEDAQUILINE (B)
1. Overview
- Forms: Tablets 100 mg
- Take with food (increases bioavailability 2-fold)
2. Mechanism of Action
- Active against both replicating AND non-replicating (persistent) bacilli - unlike INH which only kills replicating organisms
- Bactericidal AND sterilizing activity
- The M2 metabolite (N-monodesmethyl bedaquiline, 4-6x less active) is responsible for QT prolongation
- This mechanism is unique - no cross-resistance with any other class of TB drug (except clofazimine - see resistance)
3. Antimicrobial Spectrum
| Organism | Activity |
|---|---|
| M. tuberculosis | Excellent (MIC 0.03-0.12 mg/L) |
| M. avium complex (MAC) | Active |
| M. leprae, M. bovis, M. marinum | Active |
| M. kansasii, M. ulcerans, M. fortuitum, M. szulgai, M. abscessus | Active |
| Other bacteria | None |
4. Mechanisms of Resistance
- Prevalence of resistant mutants: 5×10⁻⁷ to 2×10⁻⁸
- D32V and A63P mutations in the membrane-spanning domain of the ATP synthase c-subunit gene
- Efflux pump mutations (MmpL5 upregulation) → cross-resistance with clofazimine - important clinical consequence: losing bedaquiline and clofazimine simultaneously via one mutation
- Never use as monotherapy
5. Pharmacokinetics
| Parameter | Value |
|---|---|
| Bioavailability | ~44% fasted; 2-fold increase with food |
| Protein binding | >99% |
| Volume of distribution | >10,000 L (massive tissue accumulation) |
| tmax | ~5 hours (large lag time in absorption) |
| Terminal t½ | ~5.5 months (reflects slow redistribution from tissues) |
| Metabolism | CYP3A4 → M2 metabolite (4-6x less active, causes QT prolongation) |
| Excretion | Primarily feces |
| Special populations | Clearance 52% higher in African descent; 16% lower in women |
| PK model | Three-compartment (central + 2 peripheral) |
| PK-PD driver | AUC/MIC |
6. Dosing
| Phase | Dose | Duration |
|---|---|---|
| Loading phase | 400 mg once daily | 2 weeks |
| Continuation phase | 200 mg three times a week | 22 weeks |
| Total duration | - | 24 weeks (6 months) |
- Always taken with food
- Total course = 400 mg x 14 days + 200 mg x 66 doses (3x/week x 22 weeks)
- No dose adjustment for renal or mild-moderate hepatic impairment
- Avoid in severe hepatic impairment
7. Adverse Effects
7.1 QT Prolongation - The Defining, Black-Box ADR
- FDA Black Box Warning for QT prolongation and associated mortality
- Caused by the M2 metabolite (not parent drug)
- QTc prolongation of ~12-15 ms on average at therapeutic doses
- Risk of Torsades de Pointes (TdP) - potentially fatal ventricular arrhythmia
- Risk amplified by: other QT-prolonging drugs (moxifloxacin, clofazimine, delamanid - all common MDR-TB companions), hypokalemia, hypomagnesemia, bradycardia, pre-existing cardiac disease
- Severity: Grade III QTc of 688 ms reported (PMID: 36579197 - world's first such case in MDR-TB regimen)
| QTc | Action |
|---|---|
| <450 ms | Continue; monthly ECG |
| 450-500 ms | Increase ECG frequency; correct electrolytes; review all QT-prolonging drugs |
| >500 ms | Withhold bedaquiline and all other QT-prolonging drugs; cardiology consultation; telemetry monitoring |
| Symptomatic arrhythmia | Stop immediately; emergency cardiac management |
7.2 Hepatotoxicity
- Elevated transaminases (common)
- Can cause clinical hepatitis
- Monitor LFTs at baseline and monthly
7.3 GI
- Nausea: 26% (most common - give with food, antiemetics if needed)
- Diarrhea: 13%
- Abdominal pain
- Arthralgia, headache (≥25% incidence)
7.4 Other
- Rash
- Chest pain, hemoptysis (reported in trials - may be disease-related)
8. Drug Interactions
| Drug | Interaction | Consequence |
|---|---|---|
| Rifampin, rifapentine (CYP3A4 inducers) | Dramatically reduces bedaquiline exposure | Therapeutic failure - avoid rifampin with bedaquiline |
| Moxifloxacin, clofazimine, delamanid | Additive QT prolongation | Life-threatening arrhythmia risk; mandatory ECG monitoring |
| CYP3A4 inhibitors (ketoconazole, lopinavir/ritonavir) | Increases bedaquiline + M2 levels | More QT prolongation; increase ECG monitoring |
| Alcohol | Additive hepatotoxicity | Advise abstinence |
| Efavirenz (CYP3A4 inducer in ARVs) | Reduces bedaquiline levels | Consider alternative ARV; monitor closely |
| Dolutegravir, raltegravir | Less interaction than older ARVs | Preferred ARV partners |
9. Monitoring
| Baseline | Ongoing |
|---|---|
| ECG (QTc) | Monthly ECG |
| LFTs | Monthly LFTs |
| Electrolytes (K⁺, Mg²⁺) | Correct hypokalemia/hypomagnesemia before and during |
| TSH | If symptomatic |
| Review all QT-prolonging drugs | Ongoing review |
10. Contraindications
- QTc >450 ms at baseline (relative; cardiology consultation required)
- Severe hepatic impairment
- Concurrent strong CYP3A4 inducers without close monitoring
- Should only be used when no other effective options exist (FDA label)
11. Case Report: Grade III QT Prolongation on MDR-TB Regimen (PMID: 36579197, Cureus, 2022)
- When combining bedaquiline + moxifloxacin (as in BPaLM), the additive QT risk is real and serious
- ECG monitoring must begin before the first dose and continue through treatment
- Moxifloxacin is more often the offending agent for severe QT prolongation than bedaquiline alone
- Delamanid is a reasonable substitution (also QT-prolonging but at lower doses may be manageable)
12. Quick Reference
| Feature | Key Fact |
|---|---|
| Class | Diarylquinoline |
| MOA | Inhibits subunit c of mycobacterial ATP synthase → energy depletion |
| Unique | First truly new MOA in >50 years; kills both replicating AND dormant bacilli |
| FDA approval | 2012 (XDR-TB) |
| Dose | 400 mg/day x 2 weeks → 200 mg 3x/week x 22 weeks WITH FOOD |
| Half-life | ~5.5 months |
| Defining toxicity | QT prolongation (M2 metabolite) - BLACK BOX WARNING |
| QTc threshold to stop | >500 ms |
| Key interaction | CYP3A4 inducers (rifampin) drastically lower levels |
| Resistance cross-over | Clofazimine (MmpL5 efflux pump) |
| WHO classification | Group A - standard of care for MDR-TB |
DRUG 2: PRETOMANID (Pa)
1. Overview
- Form: Tablets 200 mg
- Take with food (increases bioavailability)
- Discovered: Stover et al., 2000 (TB Alliance)
2. Mechanism of Action - Dual Action (Context-Dependent)
| Condition | Mechanism |
|---|---|
| Aerobic (replicating bacilli) | Inhibits mycolic acid and protein synthesis at the step between hydroxymycolate and ketomycolate → disrupts cell wall |
| Anaerobic (non-replicating persistent bacilli) | Generates reactive nitrogen species (NO) via its des-nitro metabolite → kills dormant intracellular bacilli; also poisons the respiratory complex → ATP depletion |
- Most TB drugs kill only actively replicating bacteria
- Pretomanid's anaerobic mechanism kills the dormant, persisting population inside macrophages and hypoxic granulomas that are responsible for treatment failure and relapse
- This is the same population that makes TB treatment require months
3. Antimicrobial Spectrum
- Specific to M. tuberculosis (MIC 0.015-0.25 mg/L)
- Lacks activity against other mycobacteria (key limitation)
- No activity against any other bacterial genus
4. Mechanisms of Resistance
| Mechanism | Details |
|---|---|
| fgd mutations (most common) | Changes in FGD structure → reduced drug activation |
| fbiA mutations | Disrupts F420 biosynthesis → impairs activation pathway |
| Rv3547 mutations | Same activation enzyme used by delamanid → potential cross-resistance with delamanid |
| Resistance frequency | 1 in 10⁶ mutants (at 5 mg/L) |
5. Pharmacokinetics
| Parameter | Value |
|---|---|
| Bioavailability | Increases with food (take with food) |
| Half-life | ~16 hours |
| Metabolism | Multiple pathways; ~20% by CYP3A4 |
| Excretion | Both urine and feces |
| PK-PD | Time-dependent activity in mouse TB models |
6. Dosing
| Dose | Frequency | Duration |
|---|---|---|
| 200 mg | Once daily | 6 months (26 weeks) |
| Always with food | - | - |
- No dose titration - flat dose throughout
- No dose adjustment described for renal failure in guidelines
- Avoid in severe hepatic impairment
7. Adverse Effects
| Adverse Effect | Notes |
|---|---|
| Peripheral neuropathy | Synergistic with linezolid; mechanism partly pretomanid-related |
| Hepatotoxicity | Elevated liver enzymes; monitor LFTs routinely |
| QT prolongation | Additive with bedaquiline and moxifloxacin |
| Nausea, GI symptoms | Common |
| Headache | Common |
| Acne | Reported in combination trials |
| Anemia | Particularly with linezolid co-administration |
| Rash | Common |
| Hyperamylasemia | Monitor amylase/lipase |
| Pancreatitis | <5% in trials |
| Elevated CPK | <5% |
| Electrolyte disturbances | <5% |
| Seizures | <5% (rare) |
8. Drug Interactions
| Drug | Interaction | Consequence |
|---|---|---|
| Rifampin / rifapentine | CYP3A4 induction | Reduced pretomanid levels → therapeutic failure; avoid |
| Bedaquiline, moxifloxacin | Additive QT prolongation | Mandatory ECG monitoring |
| CYP3A4 inhibitors | Possible increased pretomanid levels | Monitor |
9. Monitoring
| Baseline | Ongoing |
|---|---|
| LFTs | Monthly LFTs |
| ECG | Monthly ECG |
| Amylase/lipase | If abdominal symptoms |
| Neurological assessment | Monthly (peripheral neuropathy assessment) |
| Visual acuity | Baseline + monthly (combined with linezolid) |
10. Contraindications
- Concurrent rifampin or other potent CYP3A4 inducers
- Severe hepatic impairment
- Not used as monotherapy
11. Quick Reference
| Feature | Key Fact |
|---|---|
| Class | Bicyclic nitroimidazoloazine; prodrug |
| Activation | FGD1 (Rv3547), F420 cofactor |
| MOA (aerobic) | Inhibits mycolic acid + protein synthesis |
| MOA (anaerobic) | Releases NO → kills dormant bacilli; poisons respiratory complex |
| Unique | One of only a few drugs active against non-replicating persistent bacilli |
| FDA approval | 2019 |
| Dose | 200 mg once daily WITH FOOD for 6 months |
| Half-life | ~16 hours |
| Key toxicity | Hepatotoxicity + contributes to neuropathy; QT prolongation |
| Avoid with | Rifampin (CYP3A4 inducer reduces levels) |
| Cross-resistance | With delamanid (same activation enzyme) |
DRUG 3: LINEZOLID (L)
1. Overview
- Forms: Tablets 600 mg; Oral suspension 100 mg/5 mL; IV premixed 600 mg/300 mL
- Take with or without food
- Brand: Zyvox and generics
2. Mechanism of Action
- Unique binding site on 23S rRNA - no cross-resistance with any other class (aminoglycosides, macrolides, tetracyclines, fluoroquinolones all bind elsewhere on the ribosome)
- Inhibits strains of M. tuberculosis in vitro at 4-8 µg/mL
- Achieves good intracellular concentrations - active against intracellular mycobacteria
- MAO inhibitor activity - inhibits monoamine oxidase → major drug interactions
3. Antimicrobial Spectrum (TB-relevant)
| Organism | Activity |
|---|---|
| M. tuberculosis | Active (MIC 4-8 µg/mL) |
| MDR-TB strains | Active regardless of INH/rifampin resistance |
| XDR-TB strains | Active (no cross-resistance with any first or second-line TB drugs) |
| M. avium complex | Some activity (used in complex NTM cases) |
| S. aureus, MRSA | Excellent |
| VRE | Excellent |
| Drug-resistant gram-positives | Broad coverage |
4. Resistance in TB
- Rare in clinical practice so far
- Mutations in 23S rRNA gene (rrl) or ribosomal protein L3 (rplC) genes
- Cross-resistance with other oxazolidinones (tedizolid, sutezolid)
- No cross-resistance with any first-line or other second-line TB drug
5. Pharmacokinetics
| Parameter | Value |
|---|---|
| Oral bioavailability | ~100% (excellent) |
| Distribution | Good; penetrates most tissues including CNS |
| Protein binding | ~31% |
| Intracellular penetration | Excellent |
| Metabolism | ~65% hepatic (MAO-independent, non-CYP) + ~35% renal |
| Excretion | Urine (30% unchanged; rest as metabolites) |
| Half-life | ~5.5 hours |
| CYP involvement | NOT a substrate, inducer, or inhibitor of major CYP enzymes |
6. Dosing
6.1 TB (MDR/XDR-TB - BPaL/BPaLM)
| Dose | Frequency | Duration | Notes |
|---|---|---|---|
| 1200 mg | Once daily | 6 months | Standard BPaL/BPaLM dose |
| 600 mg | Once daily | 6 months | Preferred by many experts to reduce toxicity; data suggest equally effective |
| 300 mg | Once daily | Based on TDM | In patients unable to tolerate higher doses; therapeutic drug monitoring-guided |
- Original ZeNix trial used 1200 mg → high efficacy but high toxicity (>80% had adverse events)
- ZeNix trial also showed 600 mg arm had similar efficacy with significantly less toxicity
- Many experts now favor 600 mg/day or TDM-guided dosing with dose reduction if AUC/MIC targets are met
- Pyridoxine supplementation recommended for all patients (reduces neuropathy risk)
6.2 Standard Infections (Non-TB)
| Indication | Adult dose |
|---|---|
| MRSA pneumonia, bacteremia | 600 mg Q12h |
| VRE infections | 600 mg Q12h |
| Skin/soft tissue (uncomplicated) | 400 mg Q12h |
7. ADVERSE EFFECTS - The Major Limitation
7.1 Myelosuppression (Bone Marrow Suppression)
- Thrombocytopenia: Most common; dose- and duration-dependent; occurs in up to 30-50% on prolonged courses
- Anemia: Normocytic or macrocytic (interferes with pyridoxine-dependent pathways in heme synthesis); common
- Neutropenia/Leukopenia: Less common but severe
- Mechanism: Mitochondrial toxicity in bone marrow precursors
- Onset: Typically after 2+ weeks; cumulative
- Management:
- Weekly CBC for first month; then biweekly for duration of MDR-TB treatment
- Platelet count <100,000: reduce dose or interrupt linezolid
- Platelet count <50,000: stop linezolid
- Neutrophil count <1000: stop linezolid
- Anemia: consider dose reduction; pyridoxine supplementation helps
- Recovery: usually reversible on stopping
7.2 Peripheral Neuropathy
- One of the most treatment-limiting ADRs in MDR-TB patients
- Mechanism: Mitochondrial toxicity in peripheral nerves
- Pattern: Length-dependent axonal sensory polyneuropathy - starts in lower extremities, bilateral, progressive
- Onset: Usually after months (>3 months) of therapy
- Symptoms: Numbness, burning, paresthesias (feet > hands), ataxic gait
- EMG/NCS: Axonal sensory polyneuropathy
- Management:
- Reduce linezolid dose (1200 → 600 → 300 mg) as first step
- Pyridoxine (vitamin B6) supplementation - recommended for all patients
- If severe: stop linezolid
- Recovery: partial - peripheral neuropathy may NOT fully resolve even after stopping (see case report)
- This is why 600 mg dosing is increasingly preferred over 1200 mg
7.3 Optic Neuropathy
- Less common than peripheral neuropathy but potentially more feared (risk of permanent blindness)
- Mechanism: Mitochondrial toxicity in optic nerve fibers
- Pattern: Bilateral, usually central or cecocentral scotoma; painless visual loss
- Onset: Usually after >3 months
- Symptoms: Progressive painless visual impairment, color vision changes
- Fundoscopy: Optic disc swelling or pallor
- Management:
- Monthly visual acuity + color vision checks (same as ethambutol protocol)
- Stop linezolid immediately when optic neuropathy is detected
- Recovery: variable - some patients improve after stopping, others have permanent deficit
7.4 Serotonin Syndrome (Pharmacodynamic Interaction)
- Mechanism: Linezolid is a reversible, nonselective MAO inhibitor → blocks serotonin metabolism → serotonin accumulates
- Occurs when combined with serotonergic drugs
- Triggering drugs: SSRIs (fluoxetine, paroxetine, sertraline, citalopram), SNRIs (venlafaxine, duloxetine), TCAs (amitriptyline), triptans, meperidine, tramadol, trazodone, methylene blue, dextromethorphan
- Clinical presentation (Serotonin Syndrome triad):
- Neuromuscular: Tremor, myoclonus, clonus (ankle clonus is pathognomonic), hyperreflexia, incoordination
- Autonomic: Hyperthermia, tachycardia, hypertension, diaphoresis, diarrhea
- Mental status: Agitation, confusion, delirium, coma
- Severity: Mild → severe; can be fatal (hyperthermia >41°C, rigidity, multi-organ failure)
- Management:
- Stop ALL serotonergic agents including linezolid immediately
- Benzodiazepines IV (diazepam/lorazepam) for agitation and myoclonus
- Cyproheptadine (serotonin antagonist) - 12 mg stat, then 2 mg every 2h up to 32 mg/day
- Temperature control: cooling blankets, paracetamol (NOT NSAIDs - platelet issues)
- ICU admission for severe cases
- Do NOT use physostigmine (worsens cholinergic symptoms)
- Supportive: IV fluids, monitor electrolytes, rhabdomyolysis screen
7.5 Lactic Acidosis
- Mechanism: Mitochondrial dysfunction → impaired oxidative phosphorylation → anaerobic metabolism → lactic acid
- Rare but potentially life-threatening
- Presentation: Non-anion gap or anion gap metabolic acidosis, nausea, abdominal pain, weakness
- Management: Stop linezolid; supportive care; IV bicarbonate if severe
7.6 Tyramine Interaction (Dietary)
- MAO inhibitory activity → avoid foods rich in tyramine (aged cheese, cured meats, fermented products, red wine, fava beans)
- Can cause hypertensive crisis (tyramine usually broken down by intestinal MAO)
7.7 Other ADRs
- Nausea, vomiting, diarrhea (common, usually mild)
- Headache
- Hypoglycemia in patients on insulin/sulfonylureas
- Elevated blood pressure if combined with sympathomimetics
8. Drug Interactions
| Drug | Interaction | Consequence |
|---|---|---|
| SSRIs, SNRIs, TCAs, trazodone | MAO inhibition | Serotonin syndrome - contraindicated |
| MAO inhibitors | Additive MAO inhibition | Severe serotonin/hypertensive crisis - contraindicated; 14-day washout required |
| Tyramine-rich foods | Dietary tyramine not metabolized | Hypertensive crisis |
| Sympathomimetics (epinephrine, norepinephrine, dopamine) | Potentiated pressor effect | Severe hypertension |
| Insulin/sulfonylureas | Enhanced hypoglycemia | Monitor glucose |
| Serotonergic opioids (meperidine, tramadol) | Serotonin syndrome | Avoid |
| Pyridoxine | Reduces neuropathy risk | Use as supplement (not drug interaction per se) |
9. Monitoring for MDR-TB Treatment
| Parameter | Frequency |
|---|---|
| CBC (especially platelets) | Weekly x 4 weeks; then every 2 weeks |
| Visual acuity + color vision | Baseline + monthly |
| Neurological assessment (neuropathy screen) | Monthly |
| LFTs | Monthly |
| Lactic acid | If symptoms of lactic acidosis |
| Consider TDM of linezolid | If dose optimization needed; AUC-guided |
10. Case Report: Linezolid-Induced Optic and Peripheral Neuropathy in MDR-TB (PMID: 35812114, Front Neurol, 2022)
- NCS/EMG: Length-dependent axonal sensory polyneuropathy
- Fundoscopy: Bilateral optic neuropathy
- Diagnosis: Toxic neuropathy - linezolid-induced Management: Linezolid discontinued. Outcome:
- Visual symptoms: Improved after stopping linezolid
- Peripheral neuropathy: No improvement or deterioration - remained unchanged at follow-up Teaching points:
- Optic + peripheral neuropathy together = hallmark of linezolid mitochondrial toxicity
- Optic neuropathy is more reversible than peripheral neuropathy - acting early improves visual outcomes
- Peripheral neuropathy from linezolid may be permanent - this must be communicated to patients before starting
- Monthly neurological and visual surveillance is mandatory for all patients on long-term linezolid
- Pyridoxine supplementation should start from day 1 of linezolid therapy
11. Quick Reference
| Feature | Key Fact |
|---|---|
| Class | Oxazolidinone |
| MOA | Binds 23S rRNA of 50S subunit → prevents 70S initiation complex formation → inhibits protein synthesis |
| TB activity | Bactericidal against M. tuberculosis (MIC 4-8 µg/mL) |
| WHO classification | Group A for MDR-TB |
| Dose in BPaLM | 600-1200 mg/day for 6 months (600 mg preferred) |
| Standard dose | 600 mg Q12h for gram-positive infections |
| Key toxicity source | Mitochondrial ribosome inhibition (all serious ADRs) |
| Triad of serious ADRs | Myelosuppression + peripheral neuropathy + optic neuropathy |
| Fatal interaction | SSRIs/SNRIs → serotonin syndrome |
| Antidote for serotonin syndrome | Stop drug + benzodiazepines + cyproheptadine |
| Prevention of neuropathy | Pyridoxine supplementation from day 1 |
| Threshold to stop | Platelets <50,000; neutrophils <1000; any optic neuropathy |
| Reversibility | Myelosuppression: usually reversible; Optic neuropathy: often reversible; Peripheral neuropathy: may be permanent |
DRUG 4: MOXIFLOXACIN (M)
1. Overview
- Forms: Tablets 400 mg; IV solution 400 mg/250 mL
- Take with or without food (no significant food interaction)
2. Mechanism of Action
- DNA strand breaks that accumulate in the bacterium
- Inhibition of DNA replication and transcription
- Bactericidal activity
- Lung lesions (TB cavities and caseous foci)
- CSF (unlike ethambutol/streptomycin) - useful for TB meningitis
- Aerobic AND anaerobic bacterial environments
3. Antimicrobial Spectrum (TB-relevant)
| Organism | Activity |
|---|---|
| M. tuberculosis | Excellent; among the most potent anti-TB fluoroquinolones |
| MDR-TB (INH + RIF resistant) | Active (if no fluoroquinolone resistance) |
| Pre-XDR TB | Active only if no fluoroquinolone resistance |
| XDR-TB | May be resistant (fluoroquinolone resistance is a defining feature of XDR) |
| M. kansasii, M. avium | Some activity |
| Community-acquired pneumonia | Excellent |
| Gram-positive + gram-negative organisms | Broad |
4. Mechanisms of Resistance
| Mechanism | Details |
|---|---|
| gyrA mutations (most common in TB) | Codons 90 and 94 of DNA gyrase A subunit - most commonly Asp94Gly, Asp94Asn, Ala90Val |
| gyrB mutations | Less common but documented |
| Efflux pump upregulation | Can confer low-level resistance |
| Cross-resistance | Complete among all fluoroquinolones (ciprofloxacin, levofloxacin, moxifloxacin) |
5. Pharmacokinetics
| Parameter | Value |
|---|---|
| Oral bioavailability | ~90% (excellent) |
| Protein binding | ~50% |
| Distribution | All body fluids, tissues; excellent lung and CNS penetration |
| tmax | 1-3 hours |
| Half-life | ~12-16 hours (allows once-daily dosing) |
| Metabolism | ~52% hepatic (glucuronide + sulfate conjugates); NOT CYP-dependent significantly |
| Excretion | Bile/feces (~25% unchanged) + urine (~20% unchanged) |
| PK-PD driver | AUC/MIC (concentration-dependent) |
- Mild-moderate renal impairment (not renally cleared)
- Mild-moderate hepatic impairment
6. Dosing
| Indication | Dose | Frequency | Duration |
|---|---|---|---|
| MDR-TB (BPaLM) | 400 mg | Once daily | 6 months |
| CAP, complicated SSTI, intra-abdominal infections | 400 mg | Once daily | 5-14 days |
| TB meningitis (used with standard regimen) | 400 mg | Once daily | As per regimen |
7. OTHER USES OF MOXIFLOXACIN
- MDR-TB (BPaLM regimen, 6 months)
- Community-acquired pneumonia (CAP) - especially atypical organisms, penicillin-resistant pneumococcus
- Acute bacterial sinusitis (when other agents fail)
- Complicated skin and skin structure infections (cSSSI)
- Complicated intra-abdominal infections (with metronidazole for anaerobic coverage)
- Atypical mycobacterial infections (some NTM)
- Respiratory fluoroquinolone - widely used for respiratory infections with atypical coverage
- Ophthalmology: Topical 0.5% moxifloxacin eye drops for bacterial conjunctivitis, keratitis
8. ADVERSE EFFECTS
8.1 QT Prolongation - The Critical ADR in BPaLM
- Most important in the context of BPaLM - moxifloxacin is often a bigger contributor to QT prolongation than bedaquiline in combined regimens
- Mechanism: Blocks hERG (IKr) cardiac potassium channel → delayed repolarization → prolonged QTc
- Mean QTc increase: ~8-12 ms at 400 mg/day
- Combined with bedaquiline and/or pretomanid: additive QT prolongation → Torsades de Pointes risk
- The Grade III QT case (PMID: 36579197): moxifloxacin was identified as the offending agent (QTc 688 ms normalized after removing moxifloxacin, not bedaquiline)
- Same as bedaquiline protocol above
- Correct electrolytes (especially K⁺, Mg²⁺) before and during
- Avoid other QT-prolonging drugs when possible
- If QTc >500 ms: stop moxifloxacin
8.2 GI Toxicity (Common)
- Nausea, vomiting, diarrhea
- Abdominal pain
- Usually mild, self-limiting
8.3 CNS Toxicity
- Headache, dizziness (common)
- Insomnia
- Confusion, anxiety
- Seizures (rare but documented - use with caution in epilepsy)
- Psychosis (rare)
8.4 Tendinopathy and Tendon Rupture (Class Effect - All Fluoroquinolones)
- Black Box Warning (all fluoroquinolones): risk of tendinitis and tendon rupture
- Achilles tendon most commonly affected; bilateral in 50%
- Risk factors: age >60, corticosteroid use, renal failure, prior tendon disease
- Can occur during treatment or up to months after
- Management:
- At first sign of tendon pain/swelling: stop moxifloxacin immediately
- Rest, immobilization
- Ice packs, analgesia
- Orthopedic evaluation
- Corticosteroids are contraindicated (worsen tendon rupture risk)
- Recovery: weeks to months; some ruptures require surgical repair
8.5 Hepatotoxicity
- Elevated transaminases (uncommon)
- Rare acute hepatitis
- Monitor LFTs at baseline and during prolonged courses
8.6 Photosensitivity
- Fluoroquinolone class effect
- Advise sun protection, avoid prolonged UV exposure
- Wear protective clothing; use SPF 30+ sunscreen
8.7 Peripheral Neuropathy (Class Effect)
- Less common with moxifloxacin than with linezolid
- Fluoroquinolone class effect
- Usually reversible on stopping
8.8 Dysglycemia
- Both hypoglycemia and hyperglycemia reported (fluoroquinolone class effect)
- More common in diabetics on insulin/sulfonylureas
- Monitor blood glucose
8.9 Rare but Serious
- Aortic aneurysm and dissection (FDA Black Box Warning for fluoroquinolones)
- Clostridium difficile-associated diarrhea (antibiotic-associated)
- Rhabdomyolysis (rare)
- Uveitis (rare)
9. Drug Interactions
| Drug | Interaction | Consequence |
|---|---|---|
| Antacids, multivitamins, sucralfate, iron, zinc | Chelation of moxifloxacin by di/trivalent cations | Dramatically reduced absorption; space by at least 4 hours |
| Bedaquiline, pretomanid, clofazimine, delamanid | Additive QT prolongation | Life-threatening arrhythmia; mandatory ECG monitoring |
| Class IA antiarrhythmics (quinidine, procainamide) | Additive QT | Contraindicated |
| Class III antiarrhythmics (amiodarone, sotalol) | Additive QT | Contraindicated or extreme caution |
| Corticosteroids | Increased tendon rupture risk | Use combination with caution; monitor tendons |
| Insulin/sulfonylureas | Enhanced hypoglycemia | Monitor blood glucose |
| NSAIDs | Lowered seizure threshold | Use cautiously in patients at risk for seizures |
| Warfarin | Possible enhanced anticoagulant effect | Monitor INR |
10. Monitoring
| Baseline | Ongoing |
|---|---|
| ECG (QTc) | Monthly ECG throughout treatment |
| Electrolytes (K⁺, Mg²⁺) | Correct before starting; monitor monthly |
| LFTs | Monthly |
| Blood glucose (in diabetics) | More frequent monitoring |
| Neurological assessment | Monthly |
| Tendon examination | At each visit; educate patient |
11. Contraindications
- Known QT prolongation at baseline (relative; cardiology consultation)
- Severe hepatic impairment (Child-Pugh C)
- Hypokalemia or hypomagnesemia (correct first)
- Myasthenia gravis (fluoroquinolones worsen neuromuscular blockade)
- History of fluoroquinolone-associated tendon injury
- Concomitant QT-prolonging drugs where risk cannot be managed
12. Quick Reference
| Feature | Key Fact |
|---|---|
| Class | 8-methoxyfluoroquinolone |
| MOA | Inhibits DNA gyrase (topoisomerase II) and topoisomerase IV → DNA strand breaks |
| PK-PD driver | AUC/MIC (concentration-dependent) |
| Dose in BPaLM | 400 mg once daily for 6 months |
| Half-life | ~12-16 hours |
| Key toxicities | QT prolongation, tendinopathy/tendon rupture, GI, CNS |
| Black Box Warnings | QT prolongation + Torsades; Tendinitis/rupture; Aortic aneurysm/dissection |
| Key interaction | Antacids chelate → space by 4h; QT-prolonging drugs → additive risk |
| Before starting | Check gyrA/gyrB resistance; QTc; electrolytes |
| Stop if | QTc >500 ms; any tendon pain |
| Resistance | gyrA/gyrB mutations (codons 90, 94); complete cross-resistance among all FQs |
BPaLM COMPLETE MONITORING PROTOCOL
| Test | Before start | Week 2 | Monthly | Additional |
|---|---|---|---|---|
| ECG (QTc) | ✓ | ✓ | ✓ | Any cardiac symptom |
| Electrolytes (K⁺, Mg²⁺) | ✓ | ✓ | ✓ | Correct abnormals first |
| LFTs | ✓ | - | ✓ | Any hepatic symptoms |
| CBC (platelets especially) | ✓ | ✓ weekly | Biweekly | Any bleeding/pallor |
| Visual acuity + color vision | ✓ | - | ✓ | Any visual change → immediate |
| Peripheral neuropathy screen | ✓ | - | ✓ | Any tingling/numbness |
| Fluoroquinolone susceptibility (DST) | ✓ | - | - | To confirm moxifloxacin eligibility |
BPaLM TOXICITY COMPARISON TABLE
| Toxicity | Bedaquiline | Pretomanid | Linezolid | Moxifloxacin |
|---|---|---|---|---|
| QT prolongation | ✓✓ (M2 metabolite) | ✓ (mild) | ✗ | ✓✓ (often biggest contributor) |
| Hepatotoxicity | ✓ | ✓ | ✓ (mild) | ✓ (mild) |
| Myelosuppression | ✗ | ✗ | ✓✓✓ (major) | ✗ |
| Peripheral neuropathy | ✗ | ✓ | ✓✓✓ (major; mitochondrial) | ✓ (mild) |
| Optic neuropathy | ✗ | ✗ | ✓✓ | ✗ |
| GI | ✓✓ (nausea common) | ✓ | ✓ | ✓ |
| Serotonin syndrome | ✗ | ✗ | ✓✓✓ (MAO inhibitor!) | ✗ |
| Tendinopathy | ✗ | ✗ | ✗ | ✓✓ (class effect) |
| CNS | ✗ | ✗ (rare seizures) | ✗ | ✓ (headache, dizziness) |
WHY BPaLM WORKS SO WELL
| Drug | What it Targets |
|---|---|
| Bedaquiline | Energy metabolism (ATP synthesis) - kills replicating + dormant bacilli |
| Pretomanid | Cell wall (aerobic) + dormant bacilli via NO (anaerobic) |
| Linezolid | Protein synthesis (23S rRNA) - works regardless of resistance patterns |
| Moxifloxacin | DNA gyrase - kills rapidly dividing bacilli; excellent lung penetration |
- Goodman & Gilman's Pharmacological Basis of Therapeutics, pp. 3036-3109
- Katzung's Basic & Clinical Pharmacology 16th Ed., pp. 1319-1322
- Harriet Lane Handbook 23rd Ed. (Linezolid dosing)
- Sinha et al. (2025). BPaL-based regimens in non-trial settings. Clin Infect Dis. PMID: 39964841
- Simanjuntak et al. (2023). Pretomanid-containing regimens meta-analysis. Narra J. PMID: 38455633
- Bano et al. (2022). Linezolid neuropathy in MDR-TB. Front Neurol. PMID: 35812114
- Yadav (2022). Grade III QT prolongation on MDR-TB AOLR. Cureus. PMID: 36579197
how do patients presnt in toxicities of each drugs like suicidal ingestion ? how do we approach and manage them?
isoniazid overdose seizure pyridoxine treatment management
isoniazid acute overdose seizure treatment emergency
bedaquiline moxifloxacin acute overdose QT torsades management
isoniazid toxicity pyridoxine seizure refractory treatment
fluoroquinolone overdose QT torsades resuscitation emergency
PMID: 33660266
antituberculosis drug acute poisoning overdose clinical features
linezolid overdose serotonin syndrome lactic acidosis management
isoniazid overdose toxidrome management pyridoxine dose refractory seizures UpToDate guidelines
bedaquiline moxifloxacin acute overdose clinical presentation QT torsades de pointes management antidote
rifampin pyrazinamide ethambutol acute overdose toxidrome clinical features management emergency
https://www.ncbi.nlm.nih.gov/books/NBK557436
linezolid serotonin syndrome ICU management emergency treatment case
linezolid overdose acute toxicity management activated charcoal serotonin syndrome lactic acidosis emergency toxicology
pyrazinamide ethambutol rifampin acute overdose toxicity presentation
ATT DRUG TOXICITY: CLINICAL PRESENTATION AND EMERGENCY MANAGEMENT
Universal First-Step for ANY ATT Overdose
| Step | Action |
|---|---|
| A - Airway | Assess and secure; RSI if seizures/unconscious |
| B - Breathing | Oxygen, SpO2 monitoring; ventilate if apneic |
| C - Circulation | IV access x2; cardiac monitoring; BP; 12-lead ECG |
| D - Disability | GCS, pupils, blood glucose |
| E - Exposure | Look for empty tablet bottles; estimate dose ingested |
| Decontamination | Activated charcoal 1 g/kg PO if within 1 hour, alert, able to protect airway |
| Labs | CBG, LFTs, RFTs, serum lactate, ABG, CBC, electrolytes, coagulation |
| Psychiatric assessment | Safety screening after medical stabilization; suicidal intent evaluation |
FIRST-LINE DRUGS
DRUG 1: ISONIAZID (INH) OVERDOSE
The Classic Toxidrome: "The Seizure Triad"
Mechanism of Toxicity
- INH metabolites directly bind and inactivate pyridoxal-5'-phosphate (the active form of B6)
- INH inhibits pyridoxine phosphokinase (the enzyme that converts pyridoxine → pyridoxal-5'-phosphate)
- GABA synthesis fails → loss of inhibitory neurotransmission → seizures
- Multiple metabolic pathways fail → lactic acidosis from impaired pyruvate → acetyl-CoA conversion
Threshold and Timeline
| Dose ingested | Expected toxicity |
|---|---|
| <20 mg/kg | Mild (dizziness, nausea, slurred speech) |
| 20-40 mg/kg | Moderate (severe nausea, agitation, early seizures) |
| 40-200 mg/kg | Severe (status epilepticus, coma, lactic acidosis) |
| >200 mg/kg | Potentially fatal without immediate treatment |
Clinical Presentation by Timeline
| Time post-ingestion | Features |
|---|---|
| 0-30 min | Nausea, vomiting, dizziness, blurred vision, tachycardia |
| 30-90 min | Agitation, slurred speech, confusion, ataxia |
| 1-3 hours | Seizures (tonic-clonic, refractory to standard anticonvulsants), coma |
| 2-6 hours | Severe anion-gap metabolic acidosis (lactic acid), hyperpnea, hyperglycemia |
| Hours-days | Hepatotoxicity (delayed), peripheral neuropathy (chronic) |
- Seizures that do NOT respond to phenytoin (this is a critical clue - INH seizures are GABA-mediated, not Na-channel dependent)
- Seizures that partially respond to benzodiazepines but are persistent/recurrent
- Any patient with status epilepticus + high AG metabolic acidosis + TB history = presumptive INH overdose until proven otherwise
- Seizures preceded by prodrome of anxiety, restlessness, and sensory disturbances
Emergency Management
Step 1: Stabilize Airway and Secure Access
- High-flow O2, SpO2 monitoring
- IV access x2 large-bore
- Cardiac monitor, 12-lead ECG
- Draw labs including serum lactate, ABG, glucose, LFTs
Step 2: Seizure Control (Do in parallel with Step 3)
| Drug | Adult Dose | Route |
|---|---|---|
| Diazepam | 10-20 mg IV at 5 mg/min; repeat q5 min | IV |
| Lorazepam | 0.1 mg/kg IV (max 4 mg/dose); repeat x2 | IV |
| Midazolam | 10 mg IM (if no IV access) | IM |
Step 3: PYRIDOXINE - THE ANTIDOTE (Most Critical Step)
| Situation | Pyridoxine Dose |
|---|---|
| Known amount ingested | Give equal grams of pyridoxine IV (e.g., 10 g INH ingested → 10 g pyridoxine) |
| Unknown amount ingested (adult) | 5 g IV over 5-10 minutes as empirical dose |
| Standard initial protocol | 4 g IV bolus, then 1 g IM every 30 minutes until seizures stop |
| Maintenance (StatPearls/NCBI, 2024) | 4 g IV first dose, then 1 g IM q30 min |
| If no IV: | IM or IO route acceptable |
- Onset of effect: seizures typically stop within 30-60 minutes of adequate pyridoxine
- If seizures persist after pyridoxine + adequate benzodiazepines: consider propofol, phenobarbital, or ketamine infusion
- Repeat pyridoxine if seizures recur
Step 4: Activated Charcoal
- 1 g/kg PO (max 50 g) if within 1 hour and able to protect airway
- Repeat dose at 50g q4h if life-threatening ingestion (MDAC = multi-dose activated charcoal) - INH is well-adsorbed
Step 5: Metabolic Acidosis Management
- High anion-gap lactic acidosis develops as a direct result of impaired metabolism
- Most resolves once seizures stop (seizure activity generates lactate) and pyridoxine is given
- Sodium bicarbonate only if pH <7.10 or hemodynamic compromise (50-100 mEq IV)
- Do NOT give bicarb aggressively - correct the cause (stop seizures + give pyridoxine)
Step 6: Enhanced Elimination - Hemodialysis
- INH is "Moderately Dialyzable" (normal renal function) and "Dialyzable" (impaired renal function)
- However, EXTRIP recommends AGAINST routine ECTR (hemodialysis) in addition to standard care (weak recommendation)
- ECTR removes pyridoxine as well as INH - this is a critical point (the antidote is dialyzed away)
- Exception: ECTR (hemodialysis) is suggested if:
- Standard-dose pyridoxine cannot be administered, AND
- Seizures are refractory to GABA-A agonists
- Historical controls with adequate pyridoxine dosing had excellent outcomes without dialysis
Step 7: ICU Admission
- All severe INH overdose patients require ICU admission
- Continuous EEG monitoring if seizures recur
- Ventilatory support if coma/respiratory compromise
- Monitor LFTs daily for first 3-5 days (delayed hepatotoxicity)
Summary: INH Overdose
| Feature | Detail |
|---|---|
| Lethal dose | ~80-150 mg/kg; suicidal ingestion often 500+ mg/kg |
| Defining triad | Refractory seizures + High AG lactic acidosis + Coma |
| Why seizures resist phenytoin | GABA depletion (not Na-channel mechanism) |
| Antidote | Pyridoxine gram-for-gram IV |
| Empirical pyridoxine dose | 5 g IV (if dose unknown) |
| Benzodiazepines | Useful but insufficient alone |
| Dialysis | Not recommended routinely; washes out pyridoxine |
| Key pitfall | Giving phenytoin → wastes time; missing pyridoxine → death |
DRUG 2: RIFAMPIN OVERDOSE
The Classic Toxidrome: "Red Man + Hepatic Failure"
Mechanism of Toxicity
- Massive inhibition of RNA polymerase - in excess, affects mitochondrial RNA synthesis
- Severe hepatocellular toxicity with hepatic necrosis at overdose concentrations
- CNS depression via unclear mechanisms (possibly mitochondrial and membrane effects)
- Periorbital and facial edema (hypersensitivity/direct toxicity)
Clinical Presentation
| System | Features |
|---|---|
| Skin/Mucosae | Orange-red discoloration of skin, urine, tears, saliva, sweat, sputum (pathognomonic) |
| Eyes | Periorbital edema, red-orange discoloration of tears, scleral icterus (later) |
| CNS | Drowsiness → stupor → coma; headache, confusion, delirium |
| GI | Nausea, vomiting, abdominal pain, orange-red stool |
| Cardiovascular | Hypotension, tachycardia (in severe cases) |
| Liver | Jaundice (within 24-48h), elevated LFTs → fulminant hepatic failure (severe overdose) |
| Renal | Acute kidney injury (renal tubular toxicity) - especially with massive overdose |
| Hematological | Thrombocytopenia, coagulopathy (in severe hepatic failure) |
- 0-2 hours: GI symptoms, discoloration
- 2-8 hours: CNS depression, hypotension
- 24-72 hours: Hepatotoxicity peaks; liver failure in massive overdose
Emergency Management
Step 1: Standard ABCDE + ECG
- Orange discoloration of secretions - warn nursing staff (diagnostic, not alarming by itself)
- ABG, LFTs, coagulation, bilirubin, RFT
Step 2: Activated Charcoal
- 1 g/kg PO if within 1-2 hours and airway protected
- Multi-dose activated charcoal (MDAC) reduces enterohepatic recirculation of rifampin significantly - give 25-50 g q4h x 24h in significant ingestions
Step 3: Supportive Care
- IV fluid resuscitation for hypotension
- Vasopressors (norepinephrine) if fluid-refractory
- No specific antidote for rifampin toxicity
Step 4: Hepatic Monitoring and N-acetylcysteine
- Serial LFTs every 6-8 hours for first 48 hours
- If hepatotoxicity develops:
- N-acetylcysteine (NAC) 150 mg/kg IV over 15-60 min (loading), then 50 mg/kg over 4h, then 100 mg/kg over 16h - replenishes glutathione, protects hepatocytes
- Stop other hepatotoxic drugs (pyrazinamide, INH if combined ingestion)
- Hepatology consultation
- If fulminant hepatic failure: transplant evaluation
Step 5: Renal Protection
- IV fluids to maintain urine output 1-2 mL/kg/hr
- Avoid nephrotoxic drugs
- Dialysis if AKI with fluid overload or severe electrolyte disturbances
Step 6: Enhanced Elimination
- Rifampin is highly protein-bound (~80-88%) - NOT well dialyzable
- Multi-dose activated charcoal is more effective than dialysis for enhancing elimination
Summary: Rifampin Overdose
| Feature | Detail |
|---|---|
| Hallmark sign | Orange-red discoloration of all secretions (pathognomonic) |
| CNS features | Drowsiness → coma |
| Main danger | Fulminant hepatic failure (delayed 24-72h) |
| Antidote | None specific; NAC for hepatoprotection |
| Key treatment | MDAC (multi-dose activated charcoal) |
| Watch for | Coagulopathy, renal failure, hypotension |
| Dialysis | Not helpful (highly protein-bound) |
DRUG 3: PYRAZINAMIDE OVERDOSE
The Classic Toxidrome: "Hepatic + Hyperuricemia"
Mechanism of Toxicity
- Massive hepatocellular injury from toxic metabolite pyrazinoic acid
- Inhibition of urate secretion → severe gout
- Possible CNS toxicity at extreme doses
Clinical Presentation
| System | Features |
|---|---|
| GI/Liver | Nausea, vomiting, severe jaundice, RUQ pain; fulminant hepatic failure in massive overdose |
| Joints | Acute gout attack - severe polyarthralgia (urate crystals in joints, especially small joints) |
| CNS | Headache, dizziness; coma in extreme toxicity |
| Renal | AKI (associated with hyperuricemia, renal urate deposition) |
| Hematological | Sideroblastic anemia, thrombocytopenia |
Emergency Management
- Activated charcoal 1 g/kg PO if within 1 hour
- No specific antidote
- NAC for hepatoprotection (same protocol as above)
- IV hydration to protect renal function from urate nephropathy
- For acute gout: colchicine 1 mg PO, then 0.5 mg after 1 hour (NSAIDs contraindicated in renal failure; steroids if both contraindicated)
- Serial LFTs, uric acid, renal function
- Hepatology consultation if LFTs >5x ULN or jaundice
DRUG 4: ETHAMBUTOL OVERDOSE
The Classic Toxidrome: "Acute Visual Toxicity"
Mechanism of Toxicity
- Excessive chelation and inhibition of zinc-metalloenzymes in the retina and optic nerve → retrobulbar optic neuritis
- At toxic doses, can also cause peripheral neuropathy and CNS depression
Clinical Presentation
| System | Features |
|---|---|
| Visual | Sudden/rapid onset visual loss (central field), blurred vision, loss of color vision (red-green most prominent); can progress to blindness |
| Neurological | Peripheral neuropathy (fingers, toes), confusion, dizziness, headache |
| GI | Nausea, vomiting, abdominal pain |
| Other | Rash, hyperuricemia, elevated LFTs |
Emergency Management
Step 1: STOP ethambutol immediately
Step 2: Activated charcoal 1 g/kg if within 1 hour
Step 3: Ophthalmology emergency consultation
- Formal visual acuity assessment
- Color vision testing (Ishihara plates)
- Fundoscopy: optic disc edema, pallor
- Visual field testing
Step 4: No antidote; supportive care
- No specific antidote exists for ethambutol-induced optic neuropathy
- Zinc supplementation has been tried (ethambutol chelates zinc) but evidence is limited
Step 5: Consider high-dose corticosteroids
- Methylprednisolone 1 g/day IV x 3 days has been used for acute optic neuritis (same approach as other optic neuritis causes)
- Evidence for ethambutol specifically is anecdotal but used in practice by ophthalmologists
Step 6: Monitor and serial vision testing
- Vision may improve if drug stopped early; the sooner you stop, the better the visual outcome
- Visual recovery is incomplete/absent if treatment delayed
BPaLM DRUGS - TOXICITY PRESENTATION AND MANAGEMENT
DRUG 5: BEDAQUILINE OVERDOSE
The Classic Toxidrome: "Cardiac Toxidrome - QT/TdP"
Mechanism of Toxicity in Overdose
- M2 metabolite accumulates → blocks cardiac hERG (IKr) potassium channel → delayed ventricular repolarization → prolonged QTc → Torsades de Pointes (TdP) → ventricular fibrillation → sudden cardiac death
- At high doses: may cause hepatocellular injury
Clinical Presentation
| Timeline | Features |
|---|---|
| 0-5 hours | Nausea, vomiting, headache, dizziness |
| 5-48 hours | QT prolongation on ECG (typically QTc 450-600+ ms); may be asymptomatic |
| Any time | Palpitations, pre-syncope, syncope |
| Critical event | Torsades de Pointes (polymorphic VT) → cardiac arrest |
- Prolonged QTc (>500 ms)
- Premature ventricular contractions (PVCs)
- Palpitations, dizziness, presyncope
- TdP itself: episodes of rapid polymorphic VT, often self-terminating but may degenerate to VF
Emergency Management
Step 1: Continuous Cardiac Monitoring
- Immediate 12-lead ECG
- Continuous telemetry
- Identify QTc: measure multiple leads, use Fridericia correction
Step 2: Activated Charcoal (if within 1 hour)
- 1 g/kg PO if alert and airway intact
- MDAC may be considered (25-50 g q4h) - bedaquiline undergoes some enterohepatic recirculation
Step 3: Correct Electrolytes IMMEDIATELY
| Electrolyte | Target | Intervention |
|---|---|---|
| Potassium | 4.0-4.5 mEq/L | IV KCl infusion (20-40 mEq/h via central line) |
| Magnesium | 2.0-2.5 mg/dL | MgSO4 2 g IV over 15-20 min (immediate) |
| Calcium | Normal | IV calcium gluconate 1-2 g if low |
Step 4: QTc-Based Management
| QTc | Action |
|---|---|
| <450 ms | Monitor; correct electrolytes; observe 24h minimum |
| 450-500 ms | Cardiology consult; remove ALL other QT-prolonging drugs; correct electrolytes; increase ECG frequency |
| >500 ms | Stop bedaquiline; stop ALL QT-prolonging companion drugs; ICU admission; continuous ECG |
| TdP occurring | Emergency management below |
Step 5: If Torsades de Pointes occurs
- Magnesium sulfate 2 g IV bolus over 1-2 minutes - first-line for TdP regardless of serum magnesium level
- If TdP persists: repeat MgSO4 2 g IV bolus; then MgSO4 1-2 g/h infusion
- Overdrive pacing (transcutaneous or transvenous) at rate 90-110 bpm - shortens QT interval by increasing heart rate; highly effective for drug-induced TdP
- If hemodynamically unstable: unsynchronized defibrillation 200J (synchronized cardioversion for VT; unsynchronized for VF/pulseless TdP)
- Isoproterenol infusion 1-4 mcg/min if overdrive pacing unavailable - increases heart rate, shortens QT
- Avoid class Ia and III antiarrhythmics (amiodarone, quinidine, sotalol) - these further prolong QT!
- Potassium replete to 4.5 mEq/L (supranormal)
Step 6: Dialysis
- Not effective for bedaquiline (>99% protein-bound, massive Vd >10,000 L)
- Lipid emulsion therapy (intralipid 20%) has been used for highly lipophilic drug overdoses - limited evidence but may be considered as last resort
Step 7: Prolonged Monitoring
- Due to 5.5-month half-life, QT monitoring must continue for days to weeks after overdose
- Cardiology follow-up is mandatory
DRUG 6: PRETOMANID OVERDOSE
The Classic Toxidrome: "Hepatic + Metabolic"
Clinical Presentation (expected)
| System | Features |
|---|---|
| GI/Liver | Nausea, vomiting, RUQ pain; hepatic toxicity, elevated LFTs |
| CNS | Headache, dizziness; possible seizures at extreme doses |
| Cardiac | QT prolongation (contributes alongside bedaquiline/moxifloxacin) |
| Metabolic | Electrolyte disturbances (hypokalemia, hypomagnesemia) |
| Pancreas | Hyperamylasemia, possible pancreatitis |
| Neurological | Peripheral neuropathy (mainly chronic, but may accelerate) |
Emergency Management
- Standard ABCDE
- Activated charcoal 1 g/kg within 1 hour
- Continuous ECG monitoring for QT prolongation
- Serial LFTs every 6-8 hours
- NAC for hepatoprotection if LFTs rising
- Treat QT/TdP as per bedaquiline protocol above
- No specific antidote
- Poison Control Center consultation (specialized drug - limited overdose data)
DRUG 7: LINEZOLID OVERDOSE
The Classic Toxidrome: "Serotonin Syndrome + Lactic Acidosis"
Mechanism of Toxicity in Overdose
- MAO inhibition + excess serotonergic tone → Serotonin Syndrome
- Mitochondrial ribosome inhibition → impaired oxidative phosphorylation → Lactic acidosis
Clinical Presentation: Serotonin Syndrome
- Clonus (spontaneous, inducible, or ocular) - most specific sign
- Hyperreflexia + agitation
- Tremor + hyperreflexia
- Hypertonia + hyperthermia + clonus
- Inducible clonus + agitation or diaphoresis
| Component | Features |
|---|---|
| Neuromuscular | Tremor, myoclonus, clonus (ankle/patellar), hyperreflexia, incoordination, ataxia, lower limb rigidity |
| Autonomic | Diaphoresis, hyperthermia (sometimes extreme >41°C), tachycardia, hypertension, diarrhea, dilated pupils (mydriasis) |
| Mental status | Agitation, anxiety, confusion, delirium, coma |
| Grade | Features |
|---|---|
| Mild | Tachycardia, diaphoresis, tremor, myoclonus |
| Moderate | Above + clonus, hyperreflexia, hyperthermia ≤38.5°C, agitation |
| Severe | Hyperthermia >41°C, muscle rigidity, autonomic instability, rhabdomyolysis, multi-organ failure |
| Feature | Serotonin Syndrome | NMS (Neuroleptic Malignant Syndrome) | Anticholinergic |
|---|---|---|---|
| Onset | Hours | Days | Hours |
| Muscle signs | Clonus, hyperreflexia | Rigidity, bradyreflexia | Normal |
| Pupils | Dilated | Normal/small | Dilated |
| Bowel sounds | Hyperactive | Normal/reduced | Reduced |
| Cause | Serotonergic drugs | Antipsychotics | Anticholinergics |
Emergency Management: Linezolid Overdose/Serotonin Syndrome
Step 1: STOP ALL SEROTONERGIC DRUGS + LINEZOLID IMMEDIATELY
Step 2: Airway and Supportive Care
- If muscle rigidity + respiratory compromise: RSI and intubation
- Avoid succinylcholine for RSI if hyperkalemia suspected (rhabdomyolysis)
- Rocuronium 1.2 mg/kg preferred for RSI in serotonin syndrome with rigidity
Step 3: Activated Charcoal
- 1 g/kg PO if within 1 hour of ingestion
- Only if airway protected - serotonin syndrome patients can deteriorate rapidly
Step 4: Benzodiazepines - First-Line for Agitation and Neuromuscular Symptoms
| Drug | Dose | Purpose |
|---|---|---|
| Lorazepam | 2-4 mg IV q5-10 min | Agitation, myoclonus, seizures |
| Diazepam | 5-10 mg IV q10 min | As above |
| Midazolam | 5-10 mg IV/IM | If no IV access |
Step 5: Cyproheptadine - The Specific Serotonin Antagonist
| Dose | Route | Notes |
|---|---|---|
| 12 mg loading dose | PO/NG tube | First dose |
| 2 mg every 2 hours | PO/NG | If symptoms persist |
| 8 mg every 6 hours | PO/NG | Maintenance once stable |
| Max adult dose | 0.5 mg/kg/day | - |
- Works at 5-HT1A and 5-HT2 receptors
- Reduces the serotonergic hyperactivity that benzodiazepines cannot fully address
- Only available orally/NG - not IV; monitor airway before NG administration
Step 6: Temperature Management
- Remove all clothing and blankets
- Ice packs to axilla, groin, neck (cooling blankets)
- Cold IV fluids
- Mist and fan cooling
- Do NOT use antipyretics (acetaminophen, aspirin) - temperature is from muscle activity, not hypothalamic upregulation; antipyretics don't work
- If temperature >41.1°C and not responding to above: Rapid sequence intubation + neuromuscular blockade (pancuronium, vecuronium) + active cooling
- Target temperature <38.5°C
Step 7: Lactic Acidosis Management (simultaneous)
- ABG and serial serum lactate every 2-4 hours
- IV fluid resuscitation for circulation
- Sodium bicarbonate if pH <7.10 or hemodynamically compromised: 1-2 mEq/kg IV
- Continuous renal replacement therapy (CRRT) if severe persistent acidosis
- Lactic acidosis resolves with drug cessation + time (mitochondria recover)
Step 8: Rhabdomyolysis (if muscle rigidity is severe)
- CK, BMP (creatinine, BUN) every 6-8 hours
- Aggressive IV hydration (150-200 mL/hr normal saline) to maintain urine output 200-300 mL/hr
- Urinary alkalinization (sodium bicarbonate in IVF) if CK >5000 U/L
- Monitor for AKI, hyperkalemia, hypocalcemia, hypophosphatemia
Step 9: Bone Marrow Monitoring
- Daily CBC in first 48-72 hours after overdose
- Platelet transfusion if <10,000 or active bleeding
- G-CSF if severe neutropenia (<500 ANC)
Step 10: Enhanced Elimination
- Linezolid is ~31% protein-bound and renally eliminated (30% unchanged)
- Hemodialysis can remove linezolid - indicated if severe lactic acidosis (pH <7.1) or renal failure
- Exchange transfusion has been reported in pediatric cases
Summary: Linezolid Overdose
| Feature | Detail |
|---|---|
| Two defining toxidromes | Serotonin syndrome (MAO inhibition) + Lactic acidosis (mitochondrial toxicity) |
| Most specific sign of SS | Inducible ankle clonus |
| First-line treatment | Stop drug; IV benzodiazepines; cyproheptadine |
| Specific antagonist | Cyproheptadine 12 mg PO loading dose |
| Temperature danger | >41°C → rhabdomyolysis, DIC, organ failure |
| Avoid | Haloperidol, physostigmine, antipyretics for temperature |
| Key mistake | Treating only one of the two toxidromes (missing lactic acidosis or SS) |
| Monitor after stopping | CBC daily (myelosuppression may persist or worsen briefly after stopping) |
DRUG 8: MOXIFLOXACIN OVERDOSE
The Classic Toxidrome: "Cardiac + CNS + GI"
Mechanism of Toxicity in Overdose
- Dose-dependent hERG channel blockade → QTc prolongation → TdP
- CNS toxicity: excessive inhibition of GABA-A receptors (fluoroquinolone class effect) → CNS excitation, seizures
- GI mucosal toxicity: nausea, vomiting, diarrhea
Clinical Presentation
| System | Features |
|---|---|
| Cardiac | Palpitations, presyncope, syncope; ECG shows QTc prolongation, TdP; may degenerate to VF/cardiac arrest |
| CNS | Headache, dizziness, agitation, seizures (GABA inhibition), confusion, psychosis |
| GI | Nausea, vomiting, diarrhea, abdominal pain |
| Musculoskeletal | Tendon pain (acute); peripheral neuropathy (mild) |
| General | Hypotension (vasodilation), tachycardia |
Emergency Management
For QT Prolongation:
- Continuous ECG monitoring
- Stop moxifloxacin immediately (and all other QT-prolonging drugs)
- IV magnesium sulfate 2 g IV bolus (first-line, immediately)
- Correct K⁺ to 4.0-4.5 mEq/L
- Activated charcoal 1 g/kg if within 1-2 hours (moxifloxacin is well-absorbed in 1-3 hours; if presentation is early, charcoal may reduce bioavailability)
- If QTc >500 ms: ICU, continuous telemetry
For TdP:
- Same as bedaquiline section above: MgSO4 + overdrive pacing + defibrillation if needed
- Do NOT give amiodarone or sotalol (worsen QT further)
For Seizures (CNS toxicity):
- Benzodiazepines first-line (lorazepam 0.1 mg/kg IV)
- Phenobarbital second-line for refractory seizures
- Avoid fluoroquinolone-incompatible agents - NSAIDs (co-prescribed NSAIDs lower seizure threshold further)
Enhanced Elimination:
- Moxifloxacin is ~50% protein-bound - somewhat dialyzable
- Hemodialysis can be considered in severe cases with QT >600 ms and deteriorating, though moxifloxacin's half-life (12-16 hours) means it clears more naturally than bedaquiline
MASTER COMPARISON TABLE: TOXIDROMES BY DRUG
| Drug | Defining Toxidrome | Signature Feature | Antidote / Specific Treatment |
|---|---|---|---|
| INH | Seizure + Lactic acidosis + Coma | Refractory seizures, NOT responding to phenytoin | PYRIDOXINE gram-for-gram IV |
| Rifampin | Red man + CNS depression + Hepatic failure | Orange-red discoloration of ALL secretions | NAC + MDAC; no specific antidote |
| Pyrazinamide | Hepatic failure + Gout | Jaundice + severe gout attack together | NAC + colchicine; no antidote |
| Ethambutol | Optic neuropathy | Sudden visual loss, color vision loss | Stop drug; ophtho emergency; consider corticosteroids |
| Bedaquiline | Cardiac (QT → TdP) | Long-duration QT risk (weeks; 5.5-month t½) | MgSO4 + overdrive pacing; defibrillate if VF |
| Pretomanid | Hepatic + metabolic | Elevated LFTs + electrolyte disturbances | Supportive + NAC; no antidote |
| Linezolid | Serotonin syndrome + Lactic acidosis | Clonus + hyperthermia + agitation | Cyproheptadine + benzodiazepines + cooling |
| Moxifloxacin | Cardiac (QT → TdP) + CNS excitation | QTc prolongation + seizures | MgSO4 + overdrive pacing + benzodiazepines for seizures |
IF ALL 8 DRUGS INGESTED (FDC Suicidal Overdose)
- Seizures (INH-driven) - pyridoxine + benzodiazepines FIRST
- QT/TdP (bedaquiline + moxifloxacin) - continuous ECG; MgSO4; correct electrolytes
PYRIDOXINE IV - GIVE IMMEDIATELY AND EMPIRICALLY even before confirming the diagnosis. A dose of 5 g IV pyridoxine has virtually no toxicity and can be life-saving in INH-driven seizures.
- EXTRIP Workgroup, Mowry et al. (2021). Extracorporeal treatments for isoniazid poisoning. Pharmacotherapy, PMID: 33660266
- Yadav (2022). Grade III QT prolongation on MDR-TB AOLR. Cureus, PMID: 36579197
- Ferreira et al. (2024). Linezolid toxicity case report (lactic acidosis + serotonin syndrome). Cureus 2024
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Harriet Lane Handbook 23rd Ed.
- StatPearls: Pyridoxine; Linezolid toxicity
- CDC Provisional Guidelines for Bedaquiline Safety Monitoring