ECG class for MBBS pg student with ecg in it please provide pr intervals and its issue and all about qrs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete ECG class for MBBS/PG students.
ECG Class for MBBS/PG Students
Complete Guide to PR Interval, QRS Complex & AV Conduction
1. THE CARDIAC CONDUCTION SYSTEM
Before reading an ECG, understand the electrical highway of the heart:
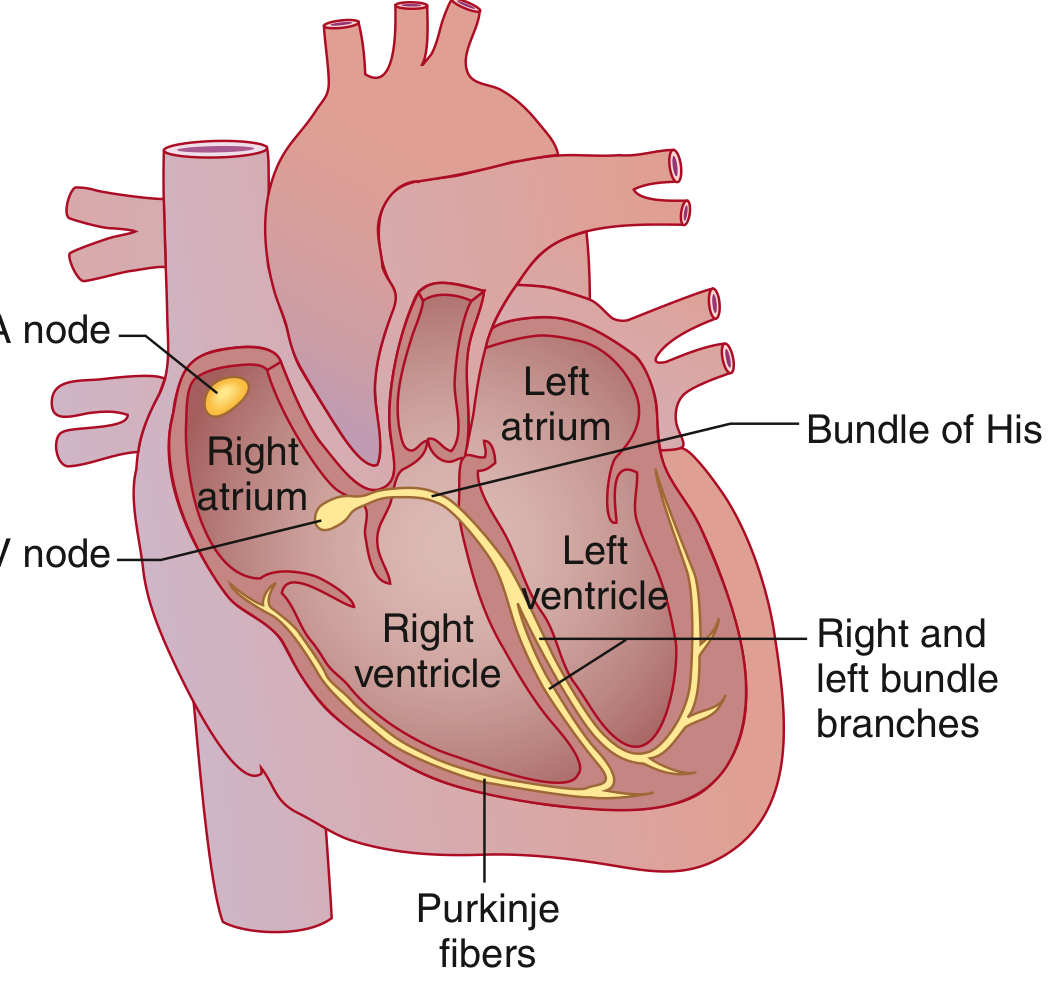
Sequence of activation:
- SA node (high lateral right atrium, near SVC) - dominant pacemaker
- Bachmann bundle - speeds depolarization to left atrium
- AV node - physiologic delay (only electrical bridge between atria and ventricles)
- Bundle of His
- Left bundle branch (anterior + posterior fascicles) and Right bundle branch
- Purkinje system - rapid conduction into ventricular muscle
The AV valve rings are electrically insulated - the AV node is the ONLY normal pathway between atria and ventricles. - Goldman-Cecil Medicine
2. NORMAL ECG INTERVALS - THE MASTER TABLE
| Parameter | Normal Value |
|---|---|
| Heart rate | 50-100 bpm |
| P wave duration | < 0.12 sec (120 ms) |
| PR interval | 0.09-0.20 sec (90-200 ms) |
| QRS duration | 0.075-0.11 sec (75-110 ms) |
| QTc (male) | 390-450 ms |
| QTc (female) | 390-460 ms |
| QRS axis | -30° to +90° |
- Goldman-Cecil Medicine, Table 42-1
ECG paper speed: 25 mm/sec | 1 small box = 0.04 sec | 1 large box = 0.2 sec
Heart rate calculation: HR = 60,000 ÷ RR interval (in ms). Memorize: 300-150-100-75-60-50 for 1-2-3-4-5-6 large boxes between QRS.
3. THE ECG WAVES - WHAT EACH REPRESENTS
| Wave/Segment | Electrical Event |
|---|---|
| P wave | Atrial depolarization |
| PR segment | Conduction through AV node + His-Purkinje (isoelectric) |
| PR interval | Onset of atrial depolarization → onset of ventricular depolarization |
| QRS complex | Ventricular depolarization |
| ST segment | Plateau of ventricular action potential (isoelectric) |
| T wave | Ventricular repolarization |
| U wave | Repolarization of Purkinje system (seen in hypokalemia) |
"The PR interval...includes the P wave and the PR segment - it is the time from initial depolarization of the atria to initial depolarization of the ventricles." - Costanzo Physiology 7e
4. THE PR INTERVAL IN DETAIL
Normal PR: 0.09-0.20 sec (90-200 ms)
What the PR interval measures:
- Time for impulse to travel from SA node → through atrial muscle → AV node → Bundle of His → Purkinje system → onset of ventricular depolarization
- Three contributors: atrial conduction + AV node delay + His-Purkinje conduction
- When PR is prolonged, the delay is usually within the AV node
5. PR INTERVAL ABNORMALITIES
A. PROLONGED PR INTERVAL (> 200 ms) = HEART BLOCK
🔴 FIRST-DEGREE AV BLOCK
- Definition: PR interval > 200 ms, every P wave is followed by a QRS
- Mechanism: Slow conduction through AV node, delay usually in the AV node itself
- No dropped beats - all P waves conduct
ECG (First-degree AV block):
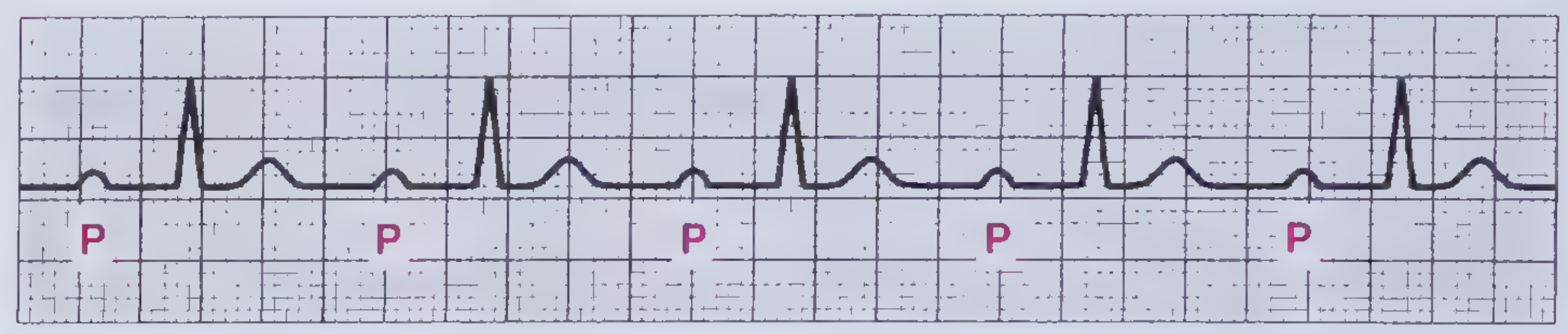 Note: Wide PR interval before each tall QRS - every P conducts
Note: Wide PR interval before each tall QRS - every P conducts
Clinical:
- Usually asymptomatic, excellent prognosis
- Common causes: vagal tone, beta-blockers, digoxin, inferior MI, rheumatic fever, Lyme disease
- Pacemaker only if PR > 300 ms with symptoms (rare)
"First-degree AV block is defined by a PR interval >200 ms on ECG." - Frameworks for Internal Medicine
🟠 SECOND-DEGREE AV BLOCK - TWO TYPES
Definition: Some P waves conduct (followed by QRS), some don't (dropped beats)
Type 1 - Mobitz I (Wenckebach)
- ECG pattern: PR interval progressively lengthens beat-by-beat until one P wave is completely blocked (no QRS)
- After the dropped beat, PR resets to its shortest value
- The RR interval shortens as PR lengthens (Wenckebach periodicity)
- Location of block: Within the AV node itself
- Vascular supply: Right coronary artery (inferior MI territory)
- Memory trick: "Longer, longer, longer, drop. Then you have a Wenckebach"
ECG (Mobitz I - Wenckebach):
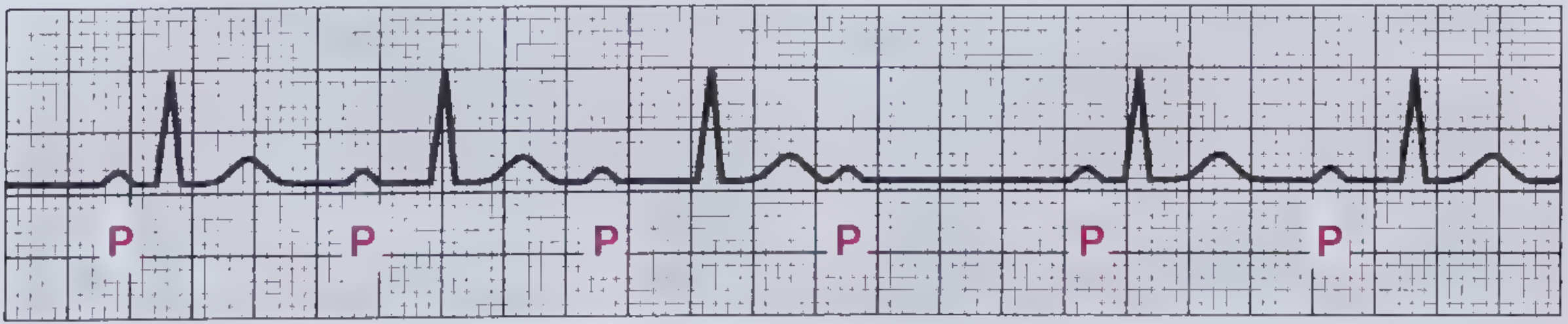 PR progressively lengthens over 4 beats, then the 5th P wave is blocked (no QRS)
PR progressively lengthens over 4 beats, then the 5th P wave is blocked (no QRS)
Clinical: Usually benign, may be asymptomatic. Rarely needs pacing unless symptomatic.
Type 2 - Mobitz II
- ECG pattern: PR interval is constant, then a P wave suddenly fails to conduct (no QRS) - without any prior lengthening
- QRS is often wide (bundle branch block pattern)
- Location of block: Below AV node - His-Purkinje system or bundle branches
- Vascular supply: Left anterior descending artery (anterior MI - look for ST elevation V1-V4)
- DANGER: High risk of progression to complete (3rd degree) heart block
ECG (Mobitz II):
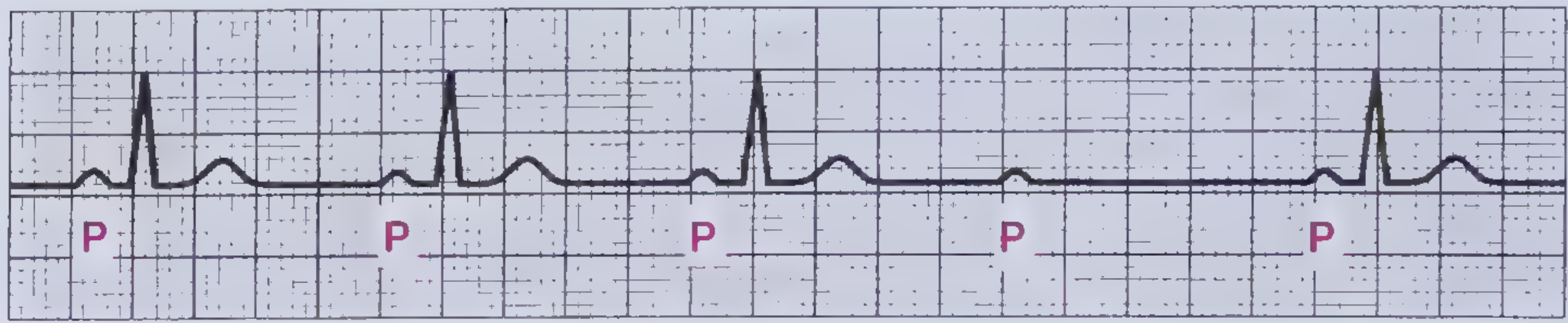 PR intervals are equal in conducted beats, then suddenly a P wave is blocked (after 4th P wave)
PR intervals are equal in conducted beats, then suddenly a P wave is blocked (after 4th P wave)
Clinical: Patients are frequently symptomatic (syncope, dyspnea). Permanent pacemaker almost always required. - Frameworks for Internal Medicine
🔴🔴 THIRD-DEGREE (COMPLETE) AV BLOCK
- Definition: Total AV dissociation - no impulse passes from atria to ventricles
- ECG pattern:
- Regular P-P intervals (atrial rhythm, ~70-80 bpm)
- Regular R-R intervals (ventricular escape rhythm, slower)
- P waves and QRS complexes are completely independent - P waves march through QRS/T waves
- Atrial rate > Ventricular rate
ECG (Third-degree AV block):
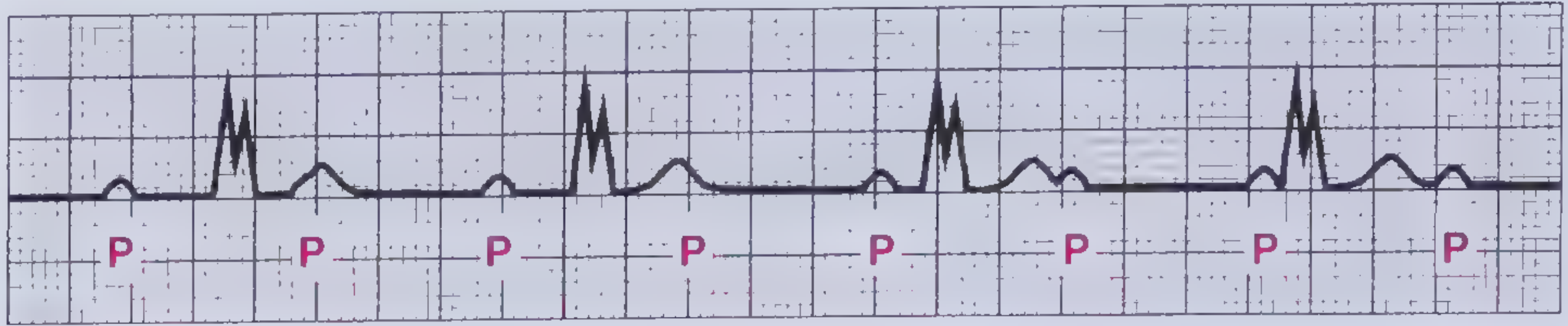 P waves march through at their own rate, QRS complexes (widened) fire at a much slower independent rate
P waves march through at their own rate, QRS complexes (widened) fire at a much slower independent rate
QRS width tells you where the escape pacemaker is:
| Escape location | QRS | Rate |
|---|---|---|
| Above Bundle of His (junctional) | Narrow | 40-60 bpm |
| Below Bundle of His (ventricular) | Wide | 20-40 bpm |
Clinical: Usually very symptomatic - syncope (Stokes-Adams attacks), dyspnea. 1-year mortality with syncope can be up to 50% without treatment. Permanent pacemaker mandatory.
B. SHORT PR INTERVAL (< 120 ms)
Three causes:
- WPW (Wolff-Parkinson-White) syndrome - accessory pathway (Bundle of Kent) bypasses AV node, creates a delta wave (slurred upstroke of QRS) + wide QRS
- Junctional rhythm - impulse originates in AV junction, travels retrograde to atria
- Enhanced AV nodal conduction (Lown-Ganong-Levine syndrome)
"A short PR interval may reflect ventricular preexcitation (Wolff-Parkinson-White syndrome), a junctional rhythm, or enhanced AV nodal conduction." - Goldman-Cecil Medicine
Causes of PR Prolongation - Summary
| Category | Examples |
|---|---|
| Drugs | Digoxin, beta-blockers, calcium channel blockers, amiodarone |
| Ischemia | Inferior MI (RCA), anterior MI (LAD) |
| Infections | Rheumatic fever, Lyme disease, myocarditis |
| Fibrosis/Calcification | Aging, calcific aortic stenosis |
| Electrolyte | Hyperkalemia |
| Congenital | ASD, AVSD |
| Others | Hypothyroidism, sarcoidosis |
6. THE QRS COMPLEX - EVERYTHING YOU NEED
Definition
The QRS complex represents ventricular muscular depolarization - the most clinically information-rich portion of the ECG.
Nomenclature Rules (Critical for exams)
- Capital letters (Q, R, S) = large deflections ≥ 5 mm (0.5 mV)
- Lowercase letters (q, r, s) = small deflections < 5 mm (0.5 mV)
- Q / q = initial negative deflection (before any R wave)
- R / r = any positive deflection
- S / s = negative deflection AFTER an R wave
- QS = entirely negative complex (no R wave at all)
- R' or r' = second positive deflection (after an S wave)
- rSR' pattern = typical Right Bundle Branch Block (RBBB) pattern in V1
Normal QRS Duration
- Normal: 0.075-0.11 sec (75-110 ms, ~2 small boxes)
- Guyton notes normal as 0.06-0.08 sec
-
0.09 sec = abnormally long (mild widening)
-
0.12 sec = pathological block in ventricular conduction system
"If the QRS duration is prolonged, an intraventricular and/or interventricular conduction delay is present." - Goldman-Cecil Medicine
7. CAUSES OF WIDE QRS (> 120 ms)
Bundle Branch Blocks
When bundle branches are blocked, impulse conducts through slow ventricular muscle instead of fast Purkinje fibers - QRS widens to ≥ 0.14 sec.
| Feature | RBBB | LBBB |
|---|---|---|
| V1 pattern | rSR' ("M" shape, rabbit ears) | QS or rS (broad, deep S) |
| V6 pattern | Wide S wave | Broad, tall R wave (no septal q) |
| T wave direction | Opposite to terminal QRS | Opposite to QRS |
| Significance | Often benign; can occur with RV strain, PE, ASD | More often pathological - IHD, cardiomyopathy |
Memory: In V1 - "WiLLiaM MaRRoW" (W in LBBB, M in RBBB)
Other Causes of Wide QRS
| Cause | Mechanism |
|---|---|
| Ventricular tachycardia (VT) | Depolarization starts in myocardium, not Purkinje |
| Hyperkalemia | Slows conduction in all myocardial cells |
| Pre-excitation (WPW) | Accessory pathway bypasses His-Purkinje |
| Ventricular hypertrophy | Longer path for impulse, QRS 0.09-0.12 sec |
| Ventricular pacing | Artificial pacing from ventricle = wide QRS (LBBB morphology) |
| Antiarrhythmic drugs | Sodium channel blockers (quinidine, procainamide, flecainide) |
"When the Purkinje fibers are blocked, the cardiac impulse must be conducted by ventricular muscle instead...QRS duration increases to 0.14 sec or longer." - Guyton & Hall Medical Physiology
8. PATHOLOGICAL Q WAVES
- A pathological Q wave = Q wave ≥ 1 small box wide (≥ 40 ms) AND ≥ 25% depth of the R wave in the same lead
- Indicates transmural (full-thickness) myocardial infarction (old or established)
- Represents electrically silent dead myocardium - the electrode "sees through" the infarct to the opposite wall's negative forces
Q wave locations and territory:
| Q waves in leads | Infarcted territory | Artery |
|---|---|---|
| V1-V4 | Anterior | LAD |
| II, III, aVF | Inferior | RCA (80%) |
| I, aVL, V5-V6 | Lateral | LCx |
| V1-V2 tall R | Posterior | RCA/LCx |
9. QRS AXIS
Normal axis: -30° to +90°
| Axis | Degrees | Significance |
|---|---|---|
| Normal | -30° to +90° | Normal |
| Left axis deviation (LAD) | -30° to -90° | Left anterior fascicular block, inferior MI, LVH |
| Right axis deviation (RAD) | +90° to +180° | RVH, PE, RBBB, lateral MI |
| Extreme axis | ±180° | VT, severe disease |
Quick bedside rule:
- Lead I positive + aVF positive = Normal axis
- Lead I positive + aVF negative = Left axis deviation
- Lead I negative + aVF positive = Right axis deviation
10. QRS IN VENTRICULAR HYPERTROPHY
Left Ventricular Hypertrophy (LVH) - Sokolow-Lyon criteria:
- S in V1 + R in V5 or V6 > 35 mm
- R in aVL > 11 mm
- Plus "strain pattern": ST depression + T wave inversion in lateral leads (I, aVL, V5-V6)
Right Ventricular Hypertrophy (RVH):
- Dominant R wave in V1 (R > S in V1)
- Right axis deviation
- ST depression + T inversion in V1-V3/V4
11. QUICK COMPARISON TABLE - AV BLOCKS
| Feature | 1st Degree | 2nd Degree Mobitz I | 2nd Degree Mobitz II | 3rd Degree |
|---|---|---|---|---|
| PR interval | >200 ms, constant | Progressively lengthens, then drops | Fixed, then sudden drop | Cannot measure (AV dissociation) |
| Dropped beats | None | Yes, after PR prolongation | Yes, sudden | All - none conducts |
| QRS width | Narrow | Usually narrow | Often wide | Narrow (junctional) or Wide (ventricular) |
| Location of block | AV node | AV node | His-Purkinje | Complete |
| Risk | Low | Low | HIGH | VERY HIGH |
| Treatment | None usually | None usually | Permanent pacemaker | Permanent pacemaker |
12. HIGH-YIELD EXAM POINTS
- PR > 200 ms = 1st degree AV block (but it's a conduction delay, not true block)
- PR progressively lengthens then drops = Mobitz I (Wenckebach)
- Fixed PR then sudden drop + wide QRS = Mobitz II (dangerous, needs pacemaker)
- P waves and QRS completely independent = Complete (3rd degree) heart block
- Short PR + delta wave + wide QRS = WPW
- QRS > 120 ms = Bundle branch block / VT / hyperkalemia / drugs
- Pathological Q = transmural MI in that territory
- RBBB: rSR' in V1 ("M" shape) | LBBB: broad notched R in V5/V6, no septal q
- Paced rhythm always produces wide QRS with LBBB morphology
- 1-year mortality of complete heart block with syncope = up to 50% without pacemaker
Sources:
- Goldman-Cecil Medicine International Edition, 2-Volume Set (Chapter 42)
- Costanzo Physiology, 7th Edition (Chapter 4)
- Frameworks for Internal Medicine (Chapter 3)
- Guyton and Hall Textbook of Medical Physiology (Chapter 12)
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
- Tintinalli's Emergency Medicine, Comprehensive Study
More ecgs and in pdf format with qrs diseases
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Running Command
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty"
This is a shared conversation. Sign in to Orris to start your own chat.