Explain physiology Control of digestive system activity in full detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full detailed answer.
Control of Digestive System Activity
The digestive system is controlled by three integrated systems working in concert: myogenic (intrinsic smooth muscle) mechanisms, the enteric nervous system (ENS), and extrinsic autonomic/hormonal regulation. Together they coordinate motility, secretion, absorption, and blood flow throughout the GI tract.
1. Structural Basis: The GI Wall
The wall of the GI tract is organized into five concentric layers:
- Serosa - outer connective tissue layer
- Longitudinal smooth muscle - outer muscle layer
- Circular smooth muscle - inner muscle layer (with myenteric plexus between the two muscle layers)
- Submucosa - loose connective tissue containing the submucosal plexus and larger vessels
- Mucosa - innermost layer, consisting of the epithelium, lamina propria, and muscularis mucosae
Individual smooth muscle fibers are 200-500 micrometers long and electrically connected via gap junctions, allowing each muscle layer to act as a syncytium - an action potential initiated anywhere can propagate throughout the entire muscle mass. This syncytial property is fundamental to coordinated peristalsis.
- Guyton and Hall Textbook of Medical Physiology, p. 776
2. Myogenic Control: Intrinsic Electrical Activity
Slow Waves (Basic Electrical Rhythm)
GI smooth muscle generates continuous, intrinsic electrical oscillations called slow waves. These are rhythmic oscillations in resting membrane potential (which averages about -56 mV) generated by interstitial cells of Cajal (ICC), which act as pacemakers.
- Slow waves are NOT action potentials - they do not directly cause contraction
- They set the maximum frequency of contractions for each segment:
- Stomach: ~3 waves/min
- Duodenum: ~12 waves/min
- Ileum: ~8 waves/min
- Mechanism: voltage-gated Ca²⁺ channels depolarize the cell → increase in [Ca²⁺]ᵢ → Ca²⁺-activated K⁺ channels open → repolarization
Spike Potentials
When slow waves reach threshold, true action potentials (spikes) are generated at their peaks. Unlike nerve fibers (which use fast Na⁺ channels), GI smooth muscle action potentials rely on slow calcium-sodium channels - hence their longer duration. The influx of Ca²⁺ during spikes directly triggers smooth muscle contraction via the calmodulin-myosin mechanism.
Tonic Contractions
Some GI smooth muscle (especially sphincters) displays tonic (sustained) contraction - continuous, not rhythmic. This can be driven by repetitive spikes, by partial depolarization via hormones, or by continuous Ca²⁺ entry without action potentials.
Factors Modulating Membrane Excitability
| Effect | Factors |
|---|---|
| Depolarization (more excitable) | Stretch of the muscle wall, ACh from parasympathetic nerves, excitatory GI hormones |
| Hyperpolarization (less excitable) | Norepinephrine, epinephrine, sympathetic stimulation |
- Guyton and Hall Textbook of Medical Physiology, pp. 776-778
3. The Enteric Nervous System (ENS): The "Mini-Brain"
The ENS is the most complex and autonomous component of GI control. It lies entirely within the gut wall from esophagus to anus and contains >100 million neurons - more than the entire spinal cord. It can function completely independently of the CNS but is modulated by autonomic input.
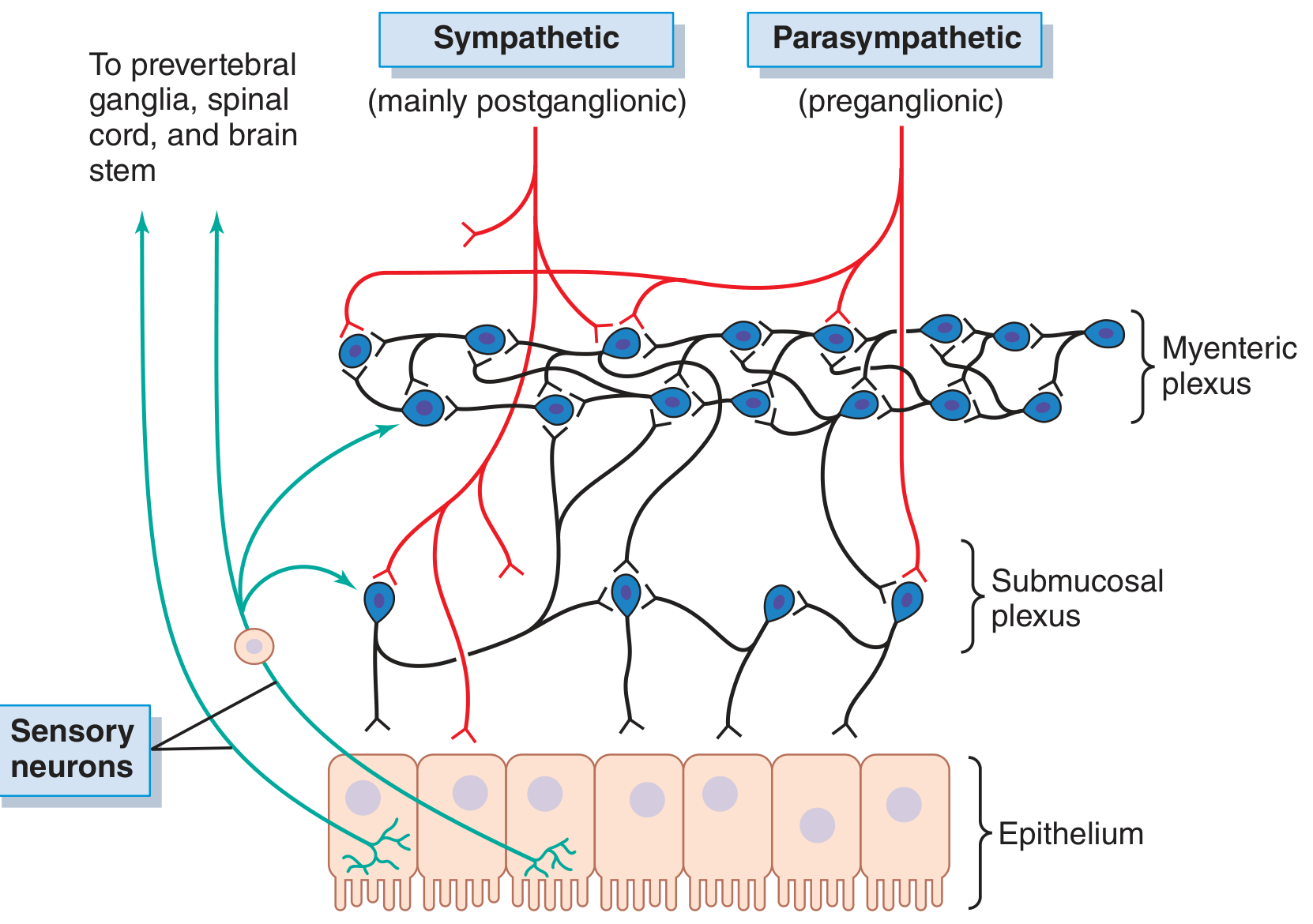
Neural control of the gut wall (Guyton & Hall, Fig. 63.4): myenteric plexus (outer), submucosal plexus (inner), with extrinsic sympathetic (red) and parasympathetic (red preganglionic) connections, and sensory neurons projecting to prevertebral ganglia, spinal cord, and brain stem (green).
The Two Plexuses
A) Myenteric Plexus (Auerbach's Plexus)
- Located between the longitudinal and circular muscle layers
- Extends the entire length of the GI tract as a continuous linear chain of interconnected neurons
- Primary function: controls GI motility
- When stimulated, produces:
- Increased tonic contraction (muscle tone)
- Increased intensity of rhythmic contractions
- Slightly increased rate of rhythmic contractions
- Increased speed of conduction along the gut wall
- Contains both excitatory and inhibitory neurons; inhibitory neurons are critical for sphincter relaxation (pyloric sphincter, ileocecal valve, LES)
B) Submucosal Plexus (Meissner's Plexus)
- Located in the submucosa, between the circular muscle layer and the mucosa
- Primary function: controls GI secretion, absorption, and local blood flow
- Integrates sensory signals from the epithelium
- Controls local intestinal secretion/absorption and mucosal infolding via submucosal muscle
The two plexuses communicate with each other extensively, and both receive input from sensory neurons in the mucosal epithelium.
- Guyton and Hall, p. 778; Ganong's Review of Medical Physiology, p. 274
ENS Neurons: Three Functional Types
| Type | Function |
|---|---|
| Sensory (afferent) neurons | Innervate receptors in the mucosa responding to mechanical, thermal, osmotic, and chemical stimuli |
| Interneurons | Integrate sensory input; relay signals within and between the two plexuses |
| Motor (efferent) neurons | Act on smooth muscle (motility), secretory cells, and blood vessels |
Neurotransmitters of the ENS
Over 25 neurotransmitters have been identified in enteric neurons, including:
-
Acetylcholine (ACh) - most common excitatory transmitter; increases motility and secretion
-
Norepinephrine - almost always inhibitory
-
Vasoactive intestinal polypeptide (VIP) - inhibitory motor neuron transmitter; relaxes sphincters
-
Nitric oxide (NO) - inhibitory; critical for LES and sphincter relaxation
-
Serotonin (5-HT) - activates peristaltic reflex; 95% of body's serotonin is in GI mucosa
-
Substance P - excitatory
-
Somatostatin - inhibitory
-
Enkephalins (leu- and met-) - modulate pain and motility
-
ATP - inhibitory
-
Dopamine, CCK, neuropeptide Y, bombesin - various modulatory roles
-
Guyton and Hall, p. 778
4. Autonomic (Extrinsic) Nervous Control
The ENS receives continuous modulation from the sympathetic and parasympathetic nervous systems via extrinsic nerve fibers.
Parasympathetic Nervous System: Enhances GI Activity
Cranial division (vagus nerve - CN X):
- Provides extensive innervation to the esophagus, stomach, pancreas, and small intestine down to the proximal half of the large intestine
- Preganglionic fibers synapse on postganglionic neurons located in the myenteric and submucosal plexuses
- Net effect: stimulation of the ENS → enhanced GI motility and secretion
Sacral division (pelvic nerves, S2-S4):
- Innervates the distal half of the large intestine (descending colon, sigmoid, rectum, anus)
- Especially important for defecation reflexes
When parasympathetic nerves are stimulated:
- Gastric motility and acid secretion increase
- Intestinal peristalsis accelerates
- Pancreatic enzyme secretion increases
- Pyloric sphincter relaxes (facilitating gastric emptying)
Sympathetic Nervous System: Inhibits GI Activity
- Postganglionic sympathetic fibers originate from the thoracolumbar spinal cord (T5-L2)
- They reach the gut via the celiac, superior mesenteric, and inferior mesenteric ganglia (prevertebral ganglia)
- Two mechanisms of inhibition:
- Direct hyperpolarization of GI smooth muscle via norepinephrine (makes the resting membrane potential more negative → reduces excitability)
- Inhibition of ENS interneurons and motor neurons at synaptic level
- Additional effects: vasoconstriction of GI blood vessels (reducing blood flow); stimulation of sphincters (causing tightening)
Key sympathetic effects:
-
Reduces peristalsis
-
Increases sphincter tone
-
Reduces secretion
-
During the "fight-or-flight" response, essentially halts digestion
-
Guyton and Hall, pp. 778-779; Medical Physiology (Boron & Boulpaep), p. 1283
5. Hormonal (Endocrine) Control
GI hormones are released from enteroendocrine cells in the mucosa into the portal circulation and act on distant target cells via specific receptors. Their effects persist even after all nervous connections are severed. This is the primary way the gut segments "communicate" with each other.
| Hormone | Source Cells / Site | Stimuli for Release | Key Actions |
|---|---|---|---|
| Gastrin | G cells of gastric antrum, duodenum, jejunum | Protein/peptides, stomach distension, vagal stimulation (GRP), alkaline pH | Stimulates gastric acid secretion, stimulates gastric mucosal growth; inhibited by low luminal pH |
| Cholecystokinin (CCK) | I cells of duodenum & jejunum | Fat (fatty acids, monoglycerides), protein, acid | Contracts gallbladder → bile release; stimulates pancreatic enzyme and bicarbonate secretion; inhibits gastric emptying; promotes pancreatic growth |
| Secretin | S cells of duodenum, jejunum, ileum | Acid in duodenum, fat | Stimulates pancreatic bicarbonate secretion, biliary bicarbonate, pepsin secretion; inhibits gastrin release, inhibits gastric emptying |
| GIP (Glucose-dependent Insulinotropic Peptide) | K cells of duodenum & jejunum | Protein, fat, carbohydrate | Stimulates insulin release; inhibits gastric acid secretion; inhibits food intake |
| Motilin | M cells of duodenum & jejunum | Fat, acid, nervous stimulation | Stimulates gastric and intestinal motility; initiates migrating motor complex (MMC) during fasting |
| GLP-1 | L cells of duodenum, jejunum, ileum, colon | Carbohydrate, fat, protein | Stimulates insulin secretion (glucose-dependent); inhibits gastric emptying, acid secretion, and food intake |
- Guyton and Hall, Table 63.1, pp. 779-780
6. Paracrine and Luminal Control
Beyond classical endocrine hormones, the GI tract uses paracrine signaling (local cell-to-cell communication):
- Histamine from enterochromaffin-like (ECL) cells directly stimulates parietal cells to secrete HCl via H₂ receptors - the basis for H₂-blocker therapy
- Somatostatin from D cells inhibits gastrin, acid secretion, and other GI hormones in a paracrine fashion
- Prostaglandins from the mucosa protect the gastric epithelium and modulate secretion
Luminal receptors in the mucosa are also key control elements:
- Chemoreceptors detect osmolality, acidity, fat content, and specific nutrients
- Mechanoreceptors (stretch receptors) respond to luminal distension
- These activate the ENS directly (via the submucosal plexus) or trigger hormone release
For example: gastric contents with elevated osmolality or high lipid content entering the duodenum activate osmo- and chemoreceptors → increased CCK release → delayed gastric emptying (enterogastric reflex).
- Medical Physiology (Boron & Boulpaep), p. 1282
7. Integrated Motor Control: Peristalsis and the Peristaltic Reflex
Peristalsis is the quintessential motor output of GI control and depends on the coordinated activity of all three control systems.
Mechanism of the peristaltic reflex ("law of the intestine"):
- Distension of the gut wall is detected by stretch-sensitive mucosal mechanoreceptors
- The ENS coordinates two simultaneous responses:
- Above the bolus: excitatory neurons release ACh and substance P → circular muscle contracts, longitudinal muscle relaxes → propulsion
- Below the bolus: inhibitory neurons release VIP and NO → circular muscle relaxes, longitudinal muscle contracts → receptive relaxation (ahead of the bolus)
- The net result is a wave of contraction progressing aborally (toward the anus)
Segmentation contractions produce local mixing (churning) without net propulsion - controlled primarily by the ENS myenteric plexus responding to local distension.
Mass peristalsis (colon): occurs 1-3 times per day, propels colonic contents 20+ cm distally; often initiated by eating (gastrocolic reflex via extrinsic and hormonal signals).
8. Migrating Motor Complex (MMC): The Fasting Pattern
During fasting, the small intestine runs a cyclic housekeeping program called the Migrating Motor Complex, controlled largely by motilin:
- Phase I: Motor quiescence (~45 min)
- Phase II: Irregular contractions (~30 min)
- Phase III: Regular, high-amplitude contractions sweeping from stomach to ileum (~5-10 min) - the "intestinal housekeeper" that clears residual food, bacteria, and debris
- The cycle repeats every ~90 minutes during fasting
- Feeding abolishes the MMC and transitions to the fed (postprandial) motor pattern
9. Sphincter Control
Six major sphincters gate GI flow, each controlled by specific neural and hormonal mechanisms:
| Sphincter | Key Control Mechanisms |
|---|---|
| Upper esophageal sphincter (UES) | Striated muscle; controlled by swallowing center in medulla (CN V, IX, X, XII); highest resting pressure of all GI sphincters |
| Lower esophageal sphincter (LES) | Smooth muscle; maintained by cholinergic tone + intrinsic myogenic properties; relaxed by vagus nerve, VIP, and NO |
| Pyloric sphincter | Controlled by ENS, hormones (CCK, secretin inhibit emptying), and vagal input |
| Ileocecal sphincter | ENS control; maintains one-way flow from ileum to cecum |
| Internal anal sphincter | Smooth muscle; relaxes reflexly in response to rectal distension (rectoanal inhibitory reflex); absent in Hirschsprung disease |
| External anal sphincter | Striated muscle; under voluntary cortical control |
General rule: Stimuli proximal to a sphincter cause relaxation; stimuli distal cause contraction - this ensures unidirectional forward flow.
10. CNS Integration: Higher Brain Centers
The ENS does not act in complete isolation. Afferent fibers from the gut wall ascend via:
- The vagus nerve (most afferent traffic, ~80% of vagal fibers are afferent, not efferent)
- The splanchnic nerves → prevertebral ganglia → spinal cord → brain
The hypothalamus, limbic system, and cortex modulate GI function through:
- Cephalic phase responses: sight, smell, thought of food → vagal activation → gastric acid and enzyme secretion begin before food even reaches the stomach
- Stress response: sympathetic activation → reduced GI motility, vasoconstriction, nausea, altered bowel habit (irritable bowel syndrome has a strong CNS-gut axis component)
The gut-brain axis is bidirectional: the gut sends far more signals to the brain than it receives back, making it a major sensory organ as well as a motor one.
Summary: Levels of Control
| Level | Mechanism | Primary Function |
|---|---|---|
| Myogenic | Slow waves (ICC), action potentials, syncytial propagation | Sets the intrinsic rhythm; baseline contractility |
| Enteric (intrinsic neural) | ENS (myenteric + submucosal plexuses), >100M neurons | Coordinates peristalsis, local reflexes, secretion, blood flow; autonomous operation |
| Autonomic (extrinsic neural) | Parasympathetic (vagus + pelvic) enhances; Sympathetic inhibits | Fine-tunes ENS; integrates with CNS; mediates cephalic and stress responses |
| Hormonal/endocrine | Gastrin, CCK, secretin, GIP, motilin, GLP-1 | Longer-range coordination between gut segments; postprandial regulation |
| Paracrine/luminal | Histamine, somatostatin, prostaglandins, mucosal receptors | Local fine-tuning; protective reflexes; nutrient sensing |
| CNS/cortical | Hypothalamus, limbic system, cephalic phase | Anticipatory responses; stress modulation; voluntary defecation control |
Sources:
- Guyton and Hall Textbook of Medical Physiology (Guyton & Hall), pp. 776-780 - structural anatomy, electrical activity, ENS plexuses, autonomic control, GI hormones
- Medical Physiology (Boron & Boulpaep), pp. 1282-1285 - smooth muscle motor activity, sphincter physiology, colonic motor patterns
- Ganong's Review of Medical Physiology, p. 274 - ENS as third division of the ANS, plexus functions
This is a shared conversation. Sign in to Orris to start your own chat.