Surgery git (oesophagus, stomach liver spleen kidney hernia , pancreas, gall bladder, small intestine, large intestine, intestinal obstruction, appendix, , rectum, anal canal, thyroid brest . These all topics 4y mbbs all imp Q according diagrams fig and clinical features
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is your complete 4th Year MBBS Surgery revision - all topics, important diagrams, figures, and clinical features:
4th Year MBBS Surgery - Important Questions with Diagrams & Clinical Features
1. OESOPHAGUS
Q: Types of Hiatus Hernia + Clinical Features
(Bailey & Love's Surgery, 28th Ed.)
| Type | Description | Clinical Features |
|---|---|---|
| Type I (Sliding) | GEJ slides into chest | GORD, heartburn, regurgitation |
| Type II (Rolling/Para-oesophageal) | Fundus herniates alongside GEJ | Obstructive symptoms, volvulus risk |
| Type III (Mixed) | Both GEJ + fundus herniate | Both GORD + obstruction |
| Type IV | Stomach + other organs (colon, spleen) | Severe obstructive symptoms |
Key diagram - Hiatus Hernia on CXR:
- Gastric bubble seen in lower mediastinum behind the heart (seen on erect CXR)
- CT shows stomach + intestine in mediastinum with mediastinal shift
Important facts:
- Type I predisposes to GORD
- Types II/III/IV require surgical treatment if volvulus/strangulation occurs
- Barium swallow is diagnostic investigation of choice
Q: Barrett's Oesophagus - Definition, Diagnosis, Risk of Cancer
- Proximal migration of columnar (salmon-coloured) mucosa >1 cm above OGJ
- Caused by chronic GORD
- Prague C&M Classification - based on Circumferential (C) and Maximal (M) extent
- Risk of cancer progression:
- Non-dysplastic Barrett's: 0.2-0.5%/year
- Low-grade dysplasia: ~0.7%/year
- High-grade dysplasia: up to 7%/year
- Risk factors: Chronic GORD >5 years, age >50, male gender, smoking, central obesity
Q: Achalasia Cardia - Clinical Features + Treatment
- Failure of LES relaxation + absent peristalsis
- Clinical features: Progressive dysphagia (both solids AND liquids - classic), regurgitation, weight loss, chest pain
- Barium swallow: "Bird's beak" appearance (rat-tail narrowing at LES)
- Treatment:
- Heller's cardiomyotomy (open or laparoscopic)
- Per Oral Endoscopic Myotomy (POEM) - newer technique
- Pneumatic dilatation (non-surgical)
Q: Carcinoma Oesophagus
- Types: Squamous cell carcinoma (upper 2/3) vs Adenocarcinoma (lower 1/3, from Barrett's)
- Clinical features: Progressive dysphagia (solids first, then liquids), weight loss, regurgitation, hoarseness (recurrent laryngeal nerve), Horner's syndrome
- Investigation: Barium swallow (irregular filling defect), endoscopy + biopsy, CT for staging
- Treatment: Ivor Lewis oesophagectomy (transthoracic approach)
2. STOMACH
Q: Peptic Ulcer Disease - Key Points
(Bailey & Love; Pye's Surgical Handicraft)
Important Summary Box:
- Most peptic ulcers caused by H. pylori or NSAIDs
- Duodenal ulcers > Gastric ulcers in frequency
- Common sites: 1st part of duodenum and lesser curve of stomach
- Gastric ulcers may be malignant - biopsy mandatory
- Complications: Perforation, Bleeding, Stenosis (pyloric obstruction)
- H. pylori eradication + PPIs = mainstay of treatment
Clinical features - Duodenal ulcer:
- Epigastric pain, relieved by food/antacids ("hunger pain")
- Pain at night (wakes patient up)
- Periodicity of symptoms
Clinical features - Gastric ulcer:
- Epigastric pain aggravated by food
- Weight loss (due to food fear)
- Nausea/vomiting
Perforated peptic ulcer:
- Sudden severe epigastric pain (board-like rigidity)
- Erect CXR: Free gas under diaphragm (pneumoperitoneum) - KEY DIAGRAM
- Treatment: Surgical - Graham patch repair (omental patch)
Q: Carcinoma Stomach
- Most common type: Adenocarcinoma
- Sites: Pylorus/antrum most common
- Clinical features: Epigastric pain, weight loss, anorexia, early satiety, vomiting (if pyloric obstruction), dysphagia (cardia)
- Signs: Epigastric mass, Virchow's node (left supraclavicular lymph node), Sister Mary Joseph nodule (umbilical), Troisier's sign
- Spread: Transcoelomic → Krukenberg's tumour (ovaries)
3. HERNIA
Q: Types of Abdominal Wall Hernias - DIAGRAM
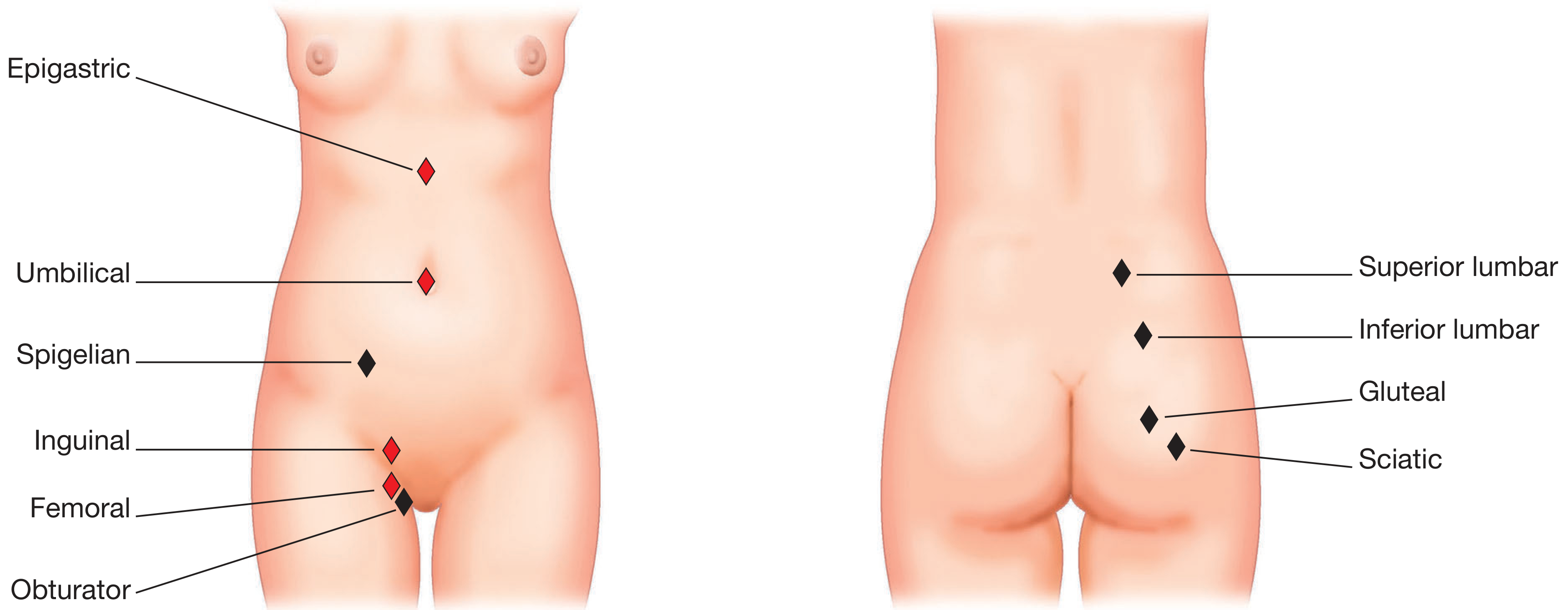
Red = Common; Black = Rare
Q: Inguinal Hernia - Anatomy + Classification
(S. Das Manual; Bailey & Love)
Indirect (Oblique) vs Direct Inguinal Hernia:
| Feature | Indirect (Oblique) | Direct |
|---|---|---|
| Origin | Through deep inguinal ring (lateral to inferior epigastric artery) | Through Hesselbach's triangle (medial to inferior epigastric artery) |
| Frequency | >80% of all inguinal hernias | Less common |
| Age | Children + young adults | Middle-aged/elderly |
| Gender | M & F (all in children/women) | Almost exclusively male |
| Reduces spontaneously | No | Yes (direct reduces easily) |
| Control by deep ring pressure | Yes (controlled) | No (not controlled) |
| Relationship to epigastric vessels | Lateral to inferior epigastric | Medial to inferior epigastric |
Hesselbach's Triangle boundaries:
- Medially: Lateral border of rectus abdominis
- Laterally: Inferior epigastric artery
- Below: Inguinal ligament
Diagram - Congenital Inguinal Hernia (persistent processus vaginalis):

Types by extent:
- Bubonocele - does not exit superficial ring
- Incomplete hernia - exits superficial ring, does not reach scrotum
- Complete hernia - reaches bottom of scrotum
Types by content: Enterocele (intestine), Epiplocele (omentum), Cystocele (bladder)
4. INTESTINAL OBSTRUCTION
Q: Intestinal Obstruction - Classification + Clinical Features
(Pye's Surgical Handicraft)
Causes by mechanism:
- Mechanical - Adhesions (most common post-op), strangulated hernia, carcinoma of colon, volvulus, intussusception, gallstone ileus
- Vascular - Mesenteric occlusion
- Neuromuscular - Paralytic ileus (post-op, peritonitis, hypokalemia)
Clinical Features:
- 4 Cardinal symptoms: Abdominal distension, Vomiting, Colicky abdominal pain, Absolute constipation (no flatus, no stool)
- Proximal small bowel obstruction → Early vomiting, less distension
- Distal obstruction → Pronounced distension
- Bowel sounds: High-pitched, tinkling, rushing sounds (metallic tinkling = SBO) → Absent in strangulation/peritonitis
Signs of strangulation (EMERGENCY):
- Local tenderness over bowel
- Rising WBC (neutrophilia)
- Shock
Key Radiological Features:
- Erect AXR: Multiple air-fluid levels
- Small bowel: Valvulae conniventes (plicae semilunares) - run across the entire width of bowel, parallel and close together
- Large bowel (haustra): Do NOT traverse full width, wider apart
- Gallstone ileus: Gas in biliary tree on X-ray
Investigations:
- WBC: Rising count warns of ischaemia
- Serum amylase: Moderately elevated in strangulation
- U&E: Electrolyte imbalance/dehydration
Treatment: Resuscitate → NG tube (nasogastric decompression) → Surgery
5. APPENDIX
Q: Acute Appendicitis - Classic Clinical Features
- Pain: Central (periumbilical) colicky pain migrating to Right Iliac Fossa (McBurney's point) - pathognomonic
- Anorexia, nausea, vomiting
- Low-grade fever
- Absolute constipation (or diarrhoea if pelvic appendix)
Examination Signs:
- McBurney's point tenderness (2/3 of way from umbilicus to ASIS)
- Rovsing's sign - palpation in LIF causes pain in RIF (indicating peritoneal irritation)
- Psoas sign - pain on extending right hip (retrocaecal appendix)
- Obturator sign - pain on internal rotation of right hip (pelvic appendix)
- Rebound tenderness (Blumberg's sign)
- Guarding and rigidity in RIF
Alvarado Score (MANTRELS):
- Migration of pain: 1
- Anorexia: 1
- Nausea/Vomiting: 1
- Tenderness in RIF: 2
- Rebound: 1
- Elevated temperature: 1
- Leucocytosis: 2
- Shift to left: 1
- Score ≥7 = appendicitis likely
Complication: Appendix mass (conservative - Ochsner-Sherren regimen) vs Appendix abscess (drain first, interval appendicectomy later)
6. LIVER
Q: Portal Hypertension - Causes + Clinical Features
- Definition: Portal pressure >12 mmHg
- Normal portal pressure: 5-10 mmHg
Causes:
- Pre-hepatic: Portal vein thrombosis, splenic vein thrombosis
- Hepatic (most common): Cirrhosis (alcoholic, viral hepatitis)
- Post-hepatic: Budd-Chiari syndrome, cardiac failure
Clinical Features - Consequences of portal hypertension:
- Oesophageal varices - haematemesis (most dangerous)
- Splenomegaly (hypersplenism - thrombocytopenia, anaemia)
- Ascites (low albumin + high portal pressure)
- Caput medusae (dilated para-umbilical veins)
- Haemorrhoids (ano-rectal varices)
Portosystemic anastomoses (sites of varices):
- OGJ (oesophageal varices)
- Para-umbilical (caput medusae)
- Ano-rectal junction (haemorrhoids)
- Retroperitoneal (Retzius veins)
7. SPLEEN
Q: Splenomegaly - Causes to Know for Surgery
Massive splenomegaly causes (exam favourite):
- Malaria (most common tropical cause)
- Kala-azar (Visceral leishmaniasis)
- Myelofibrosis
- CML
- Gaucher's disease
Indications for Splenectomy:
- Trauma (rupture)
- Hereditary spherocytosis
- ITP (refractory)
- Hypersplenism
- Staging Hodgkin's lymphoma
Post-splenectomy complications: Overwhelming Post-Splenectomy Infection (OPSI) - vaccinate against Pneumococcus, Meningococcus, H. influenzae before elective splenectomy
8. GALL BLADDER
Q: Gallstone Disease - Types + Clinical Features
- Cholesterol stones (most common in Western countries) - radiolucent
- Pigment stones - radioopaque (small, black)
- Mixed stones - most common overall
Charcot's Triad (Acute cholangitis):
- Right hypochondrial pain
- Fever + rigors
- Jaundice
Reynold's Pentad (Suppurative cholangitis - severe):
- Charcot's triad + Hypotension + Altered consciousness
Murphy's Sign (Acute cholecystitis):
- Arrest of inspiration when examiner's fingers compress right hypochondrium
- Pain on palpation of right hypochondrium during deep inspiration
Complications of gallstones:
- In gallbladder: Cholecystitis, empyema, perforation, carcinoma
- In bile duct: Obstructive jaundice, cholangitis, pancreatitis
- In bowel: Gallstone ileus (gas in biliary tree on AXR)
9. PANCREAS
Q: Acute Pancreatitis - Causes, Features, Severity
Causes (GET SMASHED mnemonic):
- Gallstones (most common), Ethanol, Trauma, Steroids, Mumps, Autoimmune, Scorpion sting, Hyperlipidaemia/Hypercalcaemia, ERCP/Emboli, Drugs
Clinical Features:
- Severe epigastric pain radiating to back ("boring" pain)
- Patient leans forward for relief
- Nausea, vomiting
- Fever
- Grey-Turner's sign (flank bruising - haemorrhagic pancreatitis)
- Cullen's sign (periumbilical bruising)
- Serum amylase/lipase elevated (>3x normal)
Ranson's Criteria (severity assessment):
At admission:
- Age >55
- WBC >16,000
- Blood glucose >200 mg/dL
- LDH >350 IU/L
- AST >250 IU/L
Within 48 hours:
- Haematocrit drop >10%
- BUN rise >5 mg/dL
- Calcium <8 mg/dL
- PaO2 <60 mmHg
- Base deficit >4 mEq/L
- Fluid sequestration >6L
Score ≥3 = severe pancreatitis
Q: Chronic Pancreatitis
(Pye's Surgical Handicraft)
- Most common cause: Alcoholism
- Triad: Pain + Steatorrhoea + Diabetes mellitus
- Steatorrhoea: Bulky, foul-smelling, fatty stools (due to lipase deficiency)
- Plain X-ray: Pancreatic calcifications (pathognomonic)
- ERCP: Dilated duct with strictures ("chain of lakes" appearance)
- Treatment: Pancreatic enzyme replacement (Creon), manage diabetes
10. SMALL INTESTINE
Q: Meckel's Diverticulum - Rule of 2s
- 2% of population
- 2 feet (60 cm) from ileocaecal junction
- 2 inches long
- 2% symptomatic
- 2 types of ectopic tissue (gastric and pancreatic)
- Presents before age 2 most commonly
- Contains gastric epithelium → causes peptic ulceration + bleeding
11. LARGE INTESTINE / COLORECTAL CANCER
Q: Colorectal Cancer - Dukes' Staging + Clinical Features
(Pye's Surgical Handicraft)
Dukes' Staging:
| Stage | Description | 5-year Survival |
|---|---|---|
| A | Tumour confined to mucosa/submucosa | 95% |
| B | Tumour invades muscle wall | 68% |
| C | Lymph node metastases present | 34% |
| D | Distant metastases | <10% |
Clinical Features:
- Change in bowel habit (most common symptom)
- Rectal bleeding (distal tumours)
- Iron deficiency anaemia (right-sided, caecal tumours - occult bleeding)
- Weight loss
- Palpable abdominal mass
- Intestinal obstruction (late complication)
- 50% of tumours located in sigmoid colon or rectum
Colonoscopic appearance:
Pedunculated adenomatous polyp - precursor to colorectal cancer
Hereditary Colorectal Cancer:
- Familial Adenomatous Polyposis (FAP): Hundreds/thousands of polyps → inevitable cancer → prophylactic colectomy + proctectomy
- HNPCC (Lynch syndrome): MSI defect, right-sided tumours
12. RECTUM
Q: Carcinoma Rectum - Important Points
- Most common rectal cancer: Adenocarcinoma
- Digital rectal examination (DRE) detects 75% of rectal cancers
- Spread: Local, lymphatic (along superior rectal artery), haematogenous (liver via portal vein)
- Investigations: Rigid/flexible sigmoidoscopy + biopsy, MRI rectum (pre-op staging), CT chest/abdomen/pelvis
- Treatment:
- Anterior resection (upper rectum) - sphincter-preserving
- Abdominoperineal resection (APR) (lower 1/3 rectum) - requires permanent colostomy
- Total Mesorectal Excision (TME) is standard
13. ANAL CANAL
Q: Haemorrhoids (Piles) - Classification + Clinical Features
Anatomy key: Anal canal = from anorectal junction to anal verge (~4 cm)
- Dentate line (pectinate line) = key landmark (midpoint of anal canal)
- Above dentate line: Internal haemorrhoids (painless, bleed)
- Below dentate line: External haemorrhoids (painful, may thrombose)
Degrees of Internal Haemorrhoids:
- 1st degree: Bleed only, do not prolapse
- 2nd degree: Prolapse on defaecation, reduce spontaneously
- 3rd degree: Prolapse on defaecation, require manual reduction
- 4th degree: Permanently prolapsed, cannot be reduced
Primary positions of haemorrhoids (3, 7, 11 o'clock in lithotomy position)
Q: Fissure-in-Ano
- Tear in anal mucosa, most common at posterior midline (6 o'clock)
- Severe pain during/after defaecation
- Bright red rectal bleeding on toilet paper
- Associated with "sentinel pile" (skin tag at lower end)
- Hypertrophied anal papilla at upper end
- Treatment: Diltiazem cream/GTN ointment (medical); lateral internal sphincterotomy (surgical)
Q: Fistula-in-Ano
- Goodsall's Rule:
- Posterior external openings → curved/horseshoe tract → internal opening at posterior midline
- Anterior external openings → straight tract → internal opening directly in front
- Parks' Classification: Intersphincteric, Transsphincteric, Suprasphincteric, Extrasphincteric
14. THYROID
Q: Thyroid Swelling - Classification + Examination
Key clinical feature: Thyroid swelling moves with swallowing (and with tongue protrusion if thyroglossal cyst)
Types of Goitre:
- Diffuse: Simple, toxic (Grave's disease), Hashimoto's thyroiditis
- Multinodular goitre (MNG)
- Solitary thyroid nodule
Grave's Disease (Toxic Diffuse Goitre) - Clinical Features:
- Eye signs: Exophthalmos, lid lag, lid retraction, ophthalmoplegia
- Thyroid: Diffuse smooth goitre + bruit
- Pretibial myxoedema
- Tremor, palpitations, weight loss, heat intolerance, diarrhoea
- TSH low, T3/T4 elevated
Carcinoma of Thyroid - Types:
| Type | Age | Spread | Prognosis |
|---|---|---|---|
| Papillary (most common, 60-80%) | Young adults | Lymphatics | Best |
| Follicular (15-20%) | Middle age | Haematogenous (bone, lung) | Good |
| Medullary (5%) | Any; familial (MEN 2) | Both | Moderate |
| Anaplastic (5%) | Elderly | Local invasion | Worst |
- Papillary carcinoma: Psammoma bodies (calcification) on histology
- Medullary carcinoma: Secretes calcitonin (tumour marker)
15. BREAST
Q: Breast Lump - Triple Assessment
Triple Assessment:
- Clinical examination (history + palpation)
- Imaging - Mammography (<35 yrs: USS; >35 yrs: Mammogram + USS)
- Histology/cytology - FNAC or Core biopsy
Mammogram showing breast cancer:

Note: 15-20% of palpable breast cancers are NOT visible on mammography - always biopsy a palpable lump
Carcinoma Breast - Clinical Features:
- Painless lump (most common presentation)
- Skin changes: Dimpling/puckering (Peau d'orange = skin of orange appearance from lymphatic blockage)
- Nipple retraction/inversion
- Nipple discharge (bloody = worrying)
- Axillary lymphadenopathy
Breast Cancer - TNM Staging Points:
- T1: ≤2 cm; T2: 2-5 cm; T3: >5 cm; T4: Chest wall/skin involvement
- N1: Mobile ipsilateral axillary nodes; N2: Fixed axillary nodes; N3: Internal mammary nodes
Benign vs Malignant Lump features:
| Feature | Benign (Fibroadenoma) | Malignant |
|---|---|---|
| Age | <35 | >40 |
| Surface | Smooth, regular | Irregular |
| Consistency | Soft/firm, rubbery | Hard |
| Mobility | Highly mobile ("breast mouse") | Fixed |
| Tenderness | May be tender | Usually non-tender |
| Skin | Normal | Dimpling, Peau d'orange |
| Nipple | Normal | Retracted |
16. KIDNEY (Surgical aspects)
Q: Renal Cell Carcinoma (Hypernephroma)
- Classic Triad: Haematuria + Loin pain + Palpable mass (in only 10% of cases - late presentation)
- Paraneoplastic features: Polycythaemia (EPO), hypercalcaemia, hypertension, Stauffer syndrome (liver dysfunction without metastases)
- Spread: Early venous spread → IVC/renal vein tumour thrombus
- Metastases to: Lung ("cannon ball" metastases), bone, liver, brain
Q: Nephroblastoma (Wilms' Tumour)
- Peak age: 3-4 years
- Large unilateral abdominal mass (do NOT palpate excessively - may rupture)
- Associated with WAGR syndrome (Wilms', Aniridia, GU abnormalities, mental Retardation)
Quick Revision Summary Table - Most Asked Diagrams in 4Y MBBS Surgery
| Topic | Most Important Diagram/Figure |
|---|---|
| Intestinal obstruction | Erect AXR with air-fluid levels; small bowel (valvulae conniventes) vs large bowel (haustra) |
| Perforation | Erect CXR - gas under diaphragm |
| Hernia | Sites diagram (epigastric, umbilical, inguinal, femoral); Direct vs indirect inguinal hernia anatomy |
| Colorectal cancer | Dukes' staging; adenoma-carcinoma sequence |
| Hiatus hernia | Types I-IV diagram; CXR retrocardiac gastric bubble |
| Barrett's oesophagus | Prague C&M classification diagram |
| Achalasia | Barium swallow "bird's beak" |
| Haemorrhoids | Degrees 1-4; lithotomy position clock face |
| Fistula-in-ano | Goodsall's rule |
| Thyroid cancer | Types table with psammoma bodies (papillary) |
| Breast cancer | Triple assessment; mammogram with spiculated lesion |
| Pancreatitis | Cullen's sign + Grey-Turner's sign; Ranson's criteria |
Sources: Bailey & Love's Short Practice of Surgery 28th Ed.; Pye's Surgical Handicraft 22nd Ed.; S. Das Manual of Clinical Surgery 13th Ed.; Schwartz's Principles of Surgery 11th Ed.; Robbins Pathology.
This is a shared conversation. Sign in to Orris to start your own chat.