Spleen
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive material for a complete, well-illustrated answer. Here it is:
The Spleen
Anatomy
The spleen is the largest secondary lymphoid organ, weighing approximately 150 g in adults. It lies in the left upper quadrant (left hypochondrium), against the diaphragm at the level of ribs IX-X.
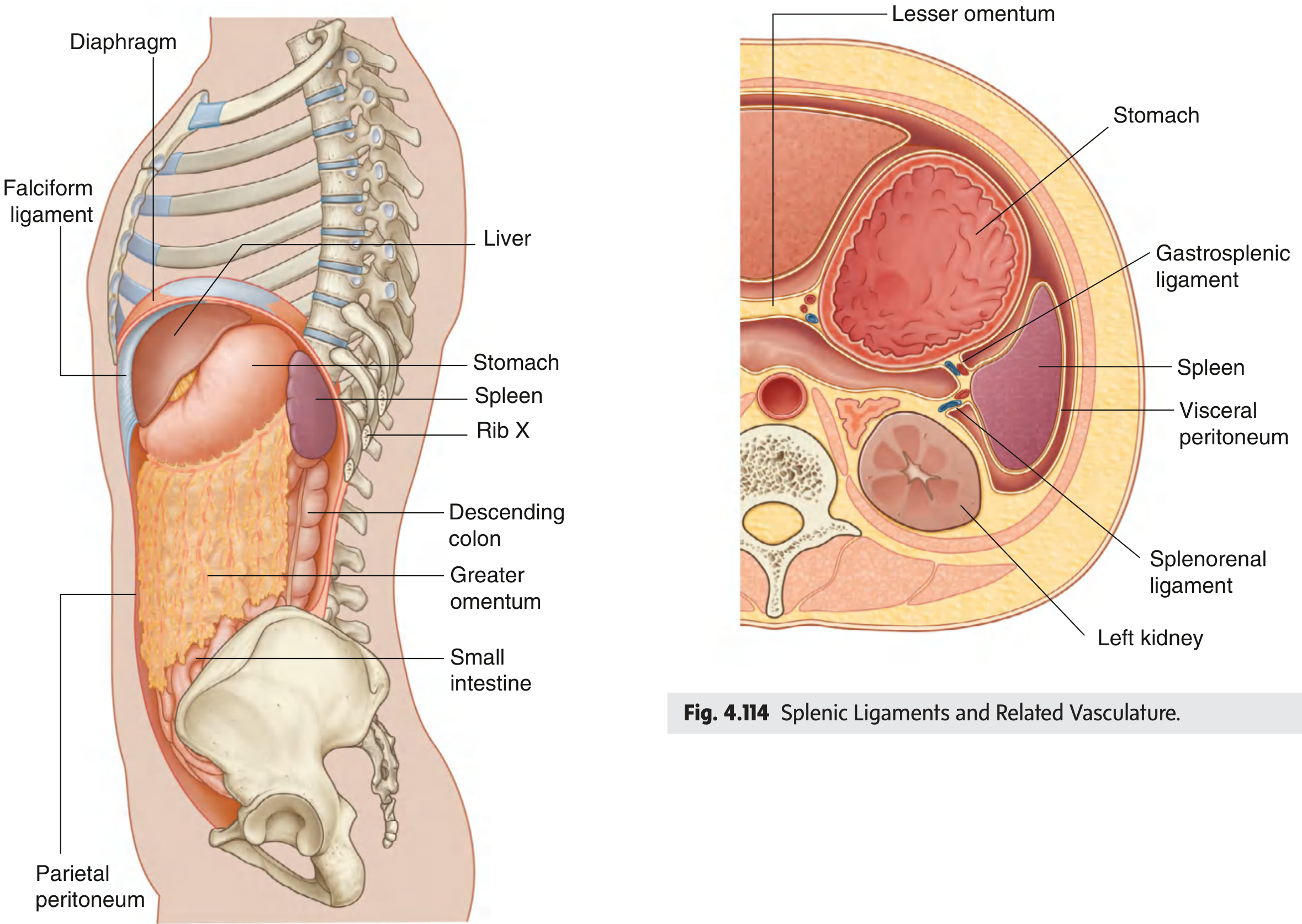
Fig. 4.113/4.114 - Spleen position and its ligamentous attachments (Gray's Anatomy for Students)
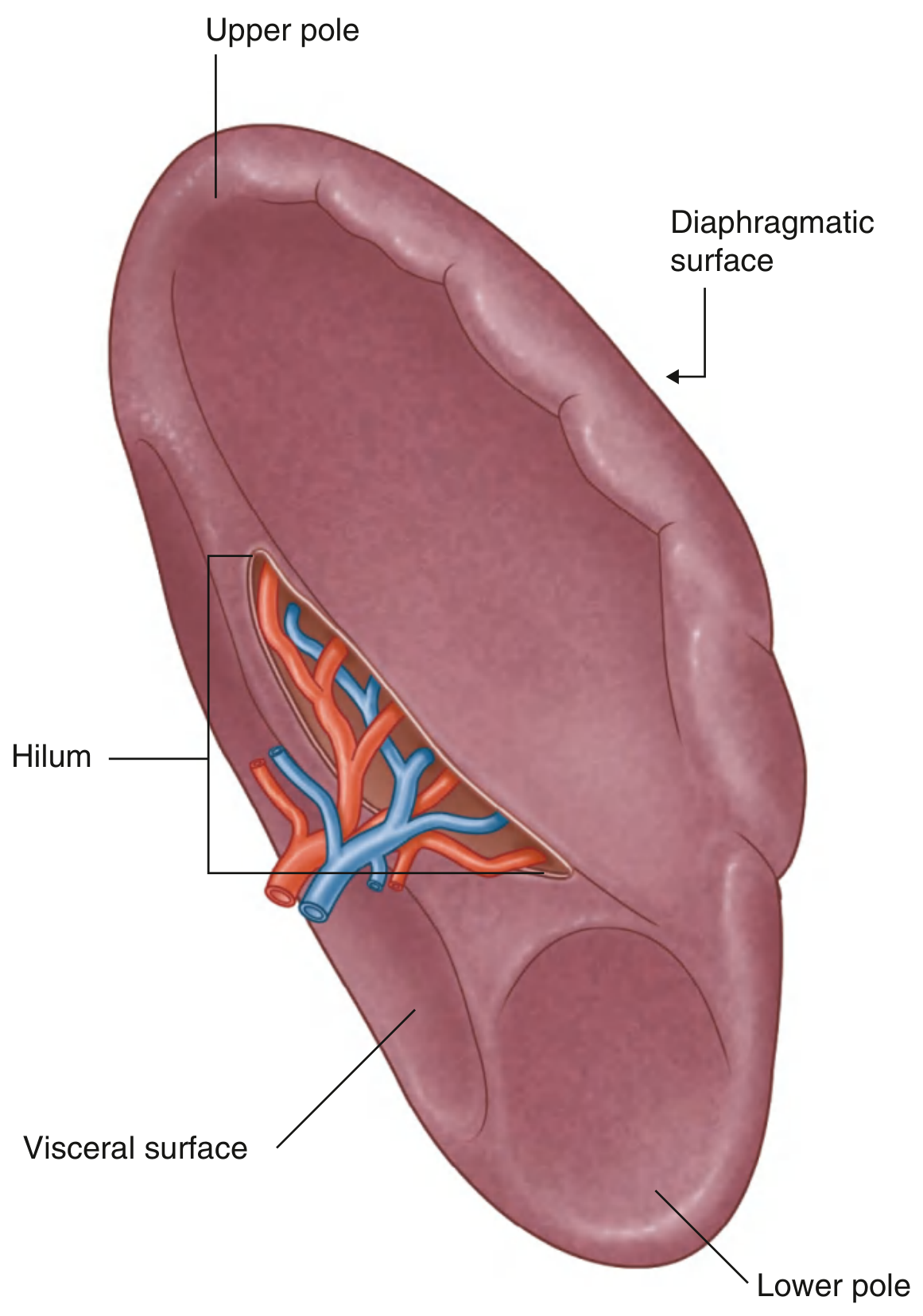
Fig. 4.115 - Surfaces and Hilum of the Spleen (Gray's Anatomy for Students)
Ligaments
The spleen is connected by two peritoneal ligaments (both parts of the greater omentum):
- Gastrosplenic ligament - to the greater curvature of the stomach; contains the short gastric and gastro-omental vessels
- Splenorenal ligament - to the left kidney; contains the splenic vessels (and occasionally the tail of the pancreas reaches the hilum here)
The spleen is entirely surrounded by visceral peritoneum except at the hilum on its medial surface, where the splenic vessels enter and exit.
Blood Supply
- Arterial: Splenic artery - from the celiac trunk
- Venous: Splenic vein drains into the portal circulation
Microstructure
The splenic parenchyma has two distinct compartments:
Red Pulp
- Composed of blood-filled vascular sinusoids lined by macrophages
- Functions as a blood filter - removes microbes, damaged/aged erythrocytes, and opsonized (antibody-coated) cells
- Sinusoids drain into venules -> splenic vein -> portal circulation
White Pulp
Contains the cells mediating adaptive immune responses to blood-borne antigens. It is organized around central arteries (branches of the splenic artery distinct from those supplying the sinusoids):
| Zone | Cell type | Function |
|---|---|---|
| Periarteriolar lymphoid sheath (PALS) | Mostly T cells | T cell zone, analogous to lymph node paracortex |
| Follicles (between marginal sinus and PALS) | B cells | Primary and secondary follicles, germinal centers |
| Marginal zone | Marginal zone B cells + specialized macrophages | Antigen sampling from blood; distinct B cell repertoire |
Antigens in the blood are delivered into the marginal sinus by circulating dendritic cells or sampled by marginal zone macrophages. Chemokines direct cell positioning: CXCL13/CXCR5 recruits B cells into follicles; CCL19/CCL21 via CCR7 directs naive T cells into the PALS.
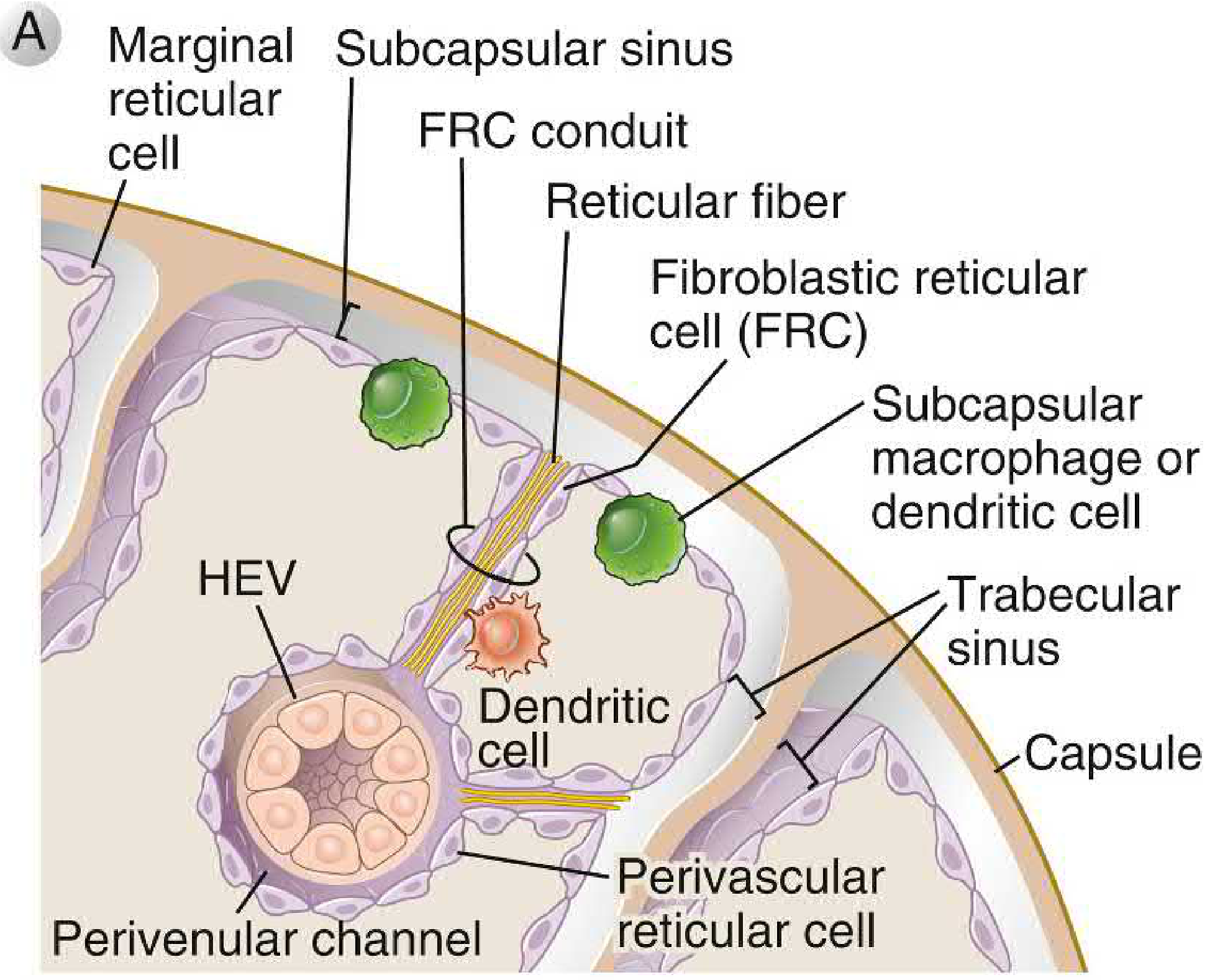
Fig. 2.19A - Microanatomy of the lymph node/spleen cortex showing FRC conduits, HEV, and cellular organization (Cellular and Molecular Immunology)
Functions
- Blood filtration - Red pulp macrophages remove aging/damaged RBCs, platelets, immune complexes, and opsonized microorganisms from the circulation
- Immune surveillance - Initiates adaptive immune responses to blood-borne antigens (T and B cell activation in white pulp)
- Antibody production - Important site of IgM production, especially against encapsulated bacteria
- Hematopoiesis - Acts as a site of extramedullary hematopoiesis in certain disease states
- Platelet and granulocyte reservoir - The spleen sequesters ~30% of the platelet pool
Clinical note: Individuals without a spleen are particularly susceptible to disseminated infections with encapsulated bacteria (Streptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae) because opsonization, phagocytosis, and antibody production in the spleen are all lost.
- Cellular and Molecular Immunology, p. 120-124
Splenomegaly
Splenomegaly is clinically significant and its causes are categorized:
Causes by Category (Robbins Pathology)
| Category | Examples |
|---|---|
| Infections | Infectious mononucleosis, tuberculosis, typhoid fever, brucellosis, CMV, malaria, kala-azar (leishmaniasis), schistosomiasis, toxoplasmosis, syphilis |
| Congestive (portal hypertension) | Liver cirrhosis, portal/splenic vein thrombosis, right-sided cardiac failure |
| Lymphohematogenous disorders | Hodgkin/non-Hodgkin lymphoma, leukemias, multiple myeloma, myeloproliferative neoplasms, hemolytic anemias |
| Immunologic-inflammatory | Rheumatoid arthritis (Felty syndrome), SLE |
| Storage/infiltrative | Gaucher disease, amyloidosis, sarcoidosis |
Massive Splenomegaly (>1500 g or reaching iliac crest/crossing midline)
The most common causes are: chronic myeloid leukemia, primary myelofibrosis, polycythemia vera, indolent lymphoma, hairy cell leukemia, beta-thalassemia major, visceral leishmaniasis (kala-azar), malaria, and Gaucher disease.
- Frameworks for Internal Medicine, p. 336
- Robbins, Cotran & Kumar, p. 589-590
Examination Technique (Cecil Medicine)
- Percussion first for dullness in the left upper quadrant
- Palpation with the right hand + left-hand counterpressure behind the spleen, or with patient in right lateral decubitus position
- Hook fingers under the left lower rib cage as patient takes a deep breath
- ~3% of healthy teenagers may have a normally palpable spleen
Hypersplenism
Long-standing splenomegaly leads to hypersplenism: elevated portal pressure causes collagen deposition in sinusoidal basement membranes, slowing blood flow through the cords, and prolonging exposure of blood cells to macrophages - resulting in excessive destruction and pancytopenia (anemia, thrombocytopenia, leukopenia).
Pathological Conditions
Splenic Infarcts
The spleen lacks significant collateral blood supply, making it prone to infarction. It is one of the most frequent sites where emboli lodge (along with kidneys and brain). In sickle cell disease, autoinfarction is an inevitable childhood consequence, resulting in a small, fibrotic, non-functional spleen (functional asplenia).
Nonspecific Acute Splenitis
In any blood-borne infection, the spleen enlarges (200-400 g), becomes soft, and shows acute red pulp congestion with neutrophils and plasma cells throughout. Follicular necrosis can occur with hemolytic streptococcal infection.
Splenic Trauma and Surgery
Injury Grading (AAST Scale - Bailey & Love)
| Grade | Type | Description |
|---|---|---|
| I | Haematoma | Subcapsular, <10% surface area |
| II | Laceration | Capsular tear, <1 cm parenchymal depth; or subcapsular haematoma 10-50% surface area |
| III | Laceration | Capsular tear, 1-3 cm depth, not involving trabecular vessel; or intraparenchymal haematoma ≥5 cm |
| IV | Laceration | >3 cm depth or involving trabecular vessel; or >25% devascularisation |
| V | Laceration/Vascular | Completely shattered spleen or hilar devascularisation |
Management
- Children: Most isolated splenic injuries can be managed non-operatively
- Adults: Especially with physiological compromise or multiple injuries, laparotomy should be considered
- Selective angioembolisation can play a role in select situations
- Splenectomy: In the compromised patient, splenectomy is the safer option
Post-Splenectomy
-
Transient rise in platelet and white cell count (may mimic sepsis)
-
Vaccination against Pneumococcus is advisable within 2-3 weeks post-operatively, after the immune system has recovered
-
Risk of OPSI (overwhelming post-splenectomy infection) - lifelong risk of fulminant sepsis with encapsulated organisms
-
Bailey and Love's Short Practice of Surgery, 28th Ed.
Sources: Gray's Anatomy for Students | Cellular and Molecular Immunology (Abbas) | Robbins, Cotran & Kumar Pathologic Basis of Disease | Frameworks for Internal Medicine | Goldman-Cecil Medicine | Bailey and Love's Short Practice of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.